www.yahoo.com

We all know and love Nurses, but isn’t it wonderful when a research study validates something you already know? We think you’ll enjoy this article.
If you’ve ever had a loved one in the hospital, you know how important nurses are. Studies show that the amount of time that nurses spend with patients is related to fewer errors. And according to a new study, investing in nursing is key to patient outcomes, including the risk of dying while in the hospital.
The study’s researchers, a team from the University of Pennsylvania, wanted to understand why certain hospitals have better outcomes than others. Specifically, the UPenn team was trying to explain why hospitals in the Kaiser Permanente health care system — an integrated health network in eight states that includes hospitals, insurance, and doctors’ offices all in one system — have such efficient and high-quality care.
Other organizations have tried to mimic Kaiser Permanente’s organizational structure in order to improve care, but with mixed results. The researchers thought there might be a different X factor that could explain Kaiser’s success: nurses.
In order to find out, the study looked at more than 550 hospitals in California, New Jersey, Pennsylvania, and Florida, including 25 California-based Kaiser Permanente hospitals and 56 Magnet hospitals. Magnet hospitals are recognized by the American Nurses Credentialing Center for being good workplaces for nurses.
Nurses in each hospital answered surveys about their work environment, level of education, job satisfaction, and the number of patients visited during a typical shift. The researchers also pulled data on patient mortality.
“It turns out that, by and large, nursing differences accounted for much of the mortality difference that we saw in Kaiser Permanente hospitals,” says study author Matthew McHugh, PhD, RN, a professor at the University of Pennsylvania School of Nursing.
The results were clear: The odds of dying were about 20 percent lower in Kaiser Permanente and Magnet hospitals, and differences in nursing accounted for “a sizeable portion of the advantage,” according to the study. The analysis adjusted for factors such as hospital size and the severity of patients’ conditions.
“It turns out that these differences we see in nursing, in terms of work environment, staffing levels, investment in nursing around a highly educated workforce, those things translate into better outcomes,” McHugh tells Yahoo Health.
There were a few specific factors that made Kaiser and Magnet hospitals stand out from the rest, McHugh explains:
1. Better work environments
Happier nurses mean healthier patients, research shows. “We find that places where nurses have a good experience working are places where nurses are better able to do their jobs. They’re more autonomous, they’re supported by management, and they’re integrated into hospital decision-making,” McHugh says.
Empowered nurses have better relationships with physicians, “so when they say ‘something isn’t right,’ they’ll be taken seriously,” McHugh adds. And patients can receive faster and more efficient care when nurses are authorized to make decisions such as when to remove a catheter, for example.
In fact, a study published last year in the Journal of Nursing Administration found that empowered nursing units are more effective and report better patient care compared to units with less authority.
Tangible changes matter, too. In response to the nurse shortage in the early 2000s, Kaiser Permanente made a deliberate, research-based effort to invest in nursing, says Marilyn Chow, PhD, RN, Vice President of National Patient Care Services and Innovation for Kaiser Permanente.
A study of Kaiser hospitals conducted in 2005 and 2006 found that nurses spent more than 35 percent of their time on documentation. Starting in 2005, the system switched to electronic medical records, which helped streamline paperwork. They also observed that nurses spent a lot of time hunting and gathering equipment and information — checking to see if a medication was ready, for instance. In response, Kaiser Permanente rearranged the work environment to make things more convenient. (Nurses now receive a notification when meds are ready for pickup.)
“We wanted to make sure that we were a place that nurses wanted to work,” Chow tells Yahoo Health. “If you have nurses who are happy and joyful at their work, they will definitely pass that on and be caring and compassionate.”
2. More nurses with Bachelor’s degrees
The role of the nurse is much more complex than it used to be, Chow explains. “The role is not only surveillance, but facilitating and coordinating the care, and not just for one patient, but for four to five patients … there are so many things to take care of,” she says. Patients also arrive sicker and leave the hospital earlier, Chow and McHugh say, which puts an extra demand on nurses to coordinate care and teach patients and family members what to do when they arrive home.
“Hospitals are very complex, and integrating all of that information requires a certain set of skills and requires you have a pool of knowledge within the overall nursing staff,” McHugh explains. He adds that the study observed a wide variation in nurse education from hospital to hospital, and that variation was associated with adverse events.
3. More nurses, period
Kaiser Permanente hospitals have a 4-to-1 patient-to-nurse ratio, on average, compared to 5-to-1 in non-Magnet hospitals, the UPenn study found.
Having more nurses ensures that there are enough eyes in rooms monitoring patients. It also means that nurses have sufficient time to follow up with patients and communicate effectively. “Nurses are at the bedside and are working with all the other providers. They’re the essential person for monitoring patient condition, and if something bad does happen, intervening and mobilizing the intervention response,” McHugh says.
We all know and love Nurses, but isn’t it wonderful when a research study validates something you already know? We think you’ll enjoy this article


 members.
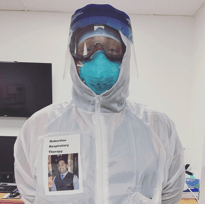
members.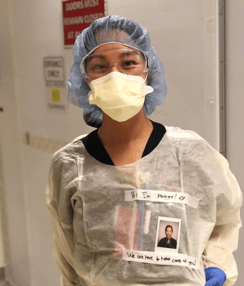 The movement is catching on amongst health care workers. Peggy Ji, an ER Doctor in Los Angeles, wrote on Instagram, "I was inspired by Robertino Rodriguez who works as a respiratory therapist in this COVID pandemic. I didn’t have a preprinted photo or a color printer so my polaroid will have to do. I wanted to bring a personal touch to caring for patients through my PPE. My hope is that our patients will know there’s a reassuring smile under this mask, and that we’re here for them."
The movement is catching on amongst health care workers. Peggy Ji, an ER Doctor in Los Angeles, wrote on Instagram, "I was inspired by Robertino Rodriguez who works as a respiratory therapist in this COVID pandemic. I didn’t have a preprinted photo or a color printer so my polaroid will have to do. I wanted to bring a personal touch to caring for patients through my PPE. My hope is that our patients will know there’s a reassuring smile under this mask, and that we’re here for them."


 Black Lives Matter protests are happening all across America and as people take to the streets to protest, medical workers are doing their part in supporting protesters.
Black Lives Matter protests are happening all across America and as people take to the streets to protest, medical workers are doing their part in supporting protesters. For the first time in history, the world will unite in celebrating the benefits that Nurses and Midwives bring to the health of the global population. The World Health Organization (WHO), has declared 2020 as The Year of the Nurse and the Midwife (YONM).
For the first time in history, the world will unite in celebrating the benefits that Nurses and Midwives bring to the health of the global population. The World Health Organization (WHO), has declared 2020 as The Year of the Nurse and the Midwife (YONM).
 As you know, Nursing is a demanding profession that requires a lot of dedication and commitment. The field has challenges that you must constantly work to overcome.
As you know, Nursing is a demanding profession that requires a lot of dedication and commitment. The field has challenges that you must constantly work to overcome. Pediatric Nurse, Meghan Nesom is an inspiration and a true example of strength. She has received heart breaking news that won't stop her from continuing her passion of healing others. Meghan reminds all of us how amazing Nurses are and no matter what they are going through in their personal lives, they will always try their hardest to stay positive and moving forward. Staying positive is something Meghan has clearly passed on to her son and once you see his response to his mother's diagnosis, you'll completely agree.
Pediatric Nurse, Meghan Nesom is an inspiration and a true example of strength. She has received heart breaking news that won't stop her from continuing her passion of healing others. Meghan reminds all of us how amazing Nurses are and no matter what they are going through in their personal lives, they will always try their hardest to stay positive and moving forward. Staying positive is something Meghan has clearly passed on to her son and once you see his response to his mother's diagnosis, you'll completely agree.

