
The U.S. has grown more diverse with every passing year, and healthcare is feeling that shift directly. Nurses are increasingly caring for patients whose cultural backgrounds, languages, and belief systems differ from their own. Many of these patients — particularly those from African, Latino, and Asian communities — face some of the steepest barriers to healthcare access and carry a disproportionate share of the country's health disparities. Since COVID-19, "disparity" has become a household word, but the underlying problem it names — that race and ethnicity still shape health outcomes across nearly every measure — is far from new.
Nursing sits at the center of this challenge. As the largest group of healthcare providers in the country, nurses show up in every setting where care happens: hospitals, outpatient clinics, rural health centers, detention facilities, and beyond. That reach means nursing education has an outsized role to play in whether the profession helps close health disparities or unintentionally reinforces them.
What Cultural Sensitivity Actually Requires
It's tempting to think of cultural sensitivity as simply knowing that different cultures exist. But real cultural sensitivity goes further — it means understanding and respecting each patient's background, from their religious practices to their family structure to their social circumstances, and letting that understanding shape how nurses communicate, what they recommend, and how they deliver care.
Cultural sensitivity is best understood as one piece of a larger picture that includes cultural competence and cultural humility. Competence is built through education, immersion experiences, and stronger communication skills — but a nurse's age, self-awareness, and training also shape how culturally attuned they become.
Nursing decisions are never made in a vacuum. Every day, nurses draw on core ethical principles — autonomy, justice, non-maleficence, and beneficence — to guide patient care. Cultural sensitivity training helps nurses apply those principles more effectively across diverse patient populations, and it fosters a more collegial workplace for an increasingly diverse nursing workforce.
The Weight of Bias
None of this works without confronting bias directly. Every person carries both implicit and explicit biases — attitudes shaped by upbringing, personal experience, and even social media exposure. Explicit bias is the kind we're consciously aware of holding. Implicit bias is trickier: it operates below conscious awareness, but it still shapes how caregivers treat patients and colleagues, often leading to unintentional discrimination and worse health outcomes.
Left unexamined, these biases calcify into stereotypes that damage both patient care and student-faculty relationships. That's not abstract — it plays out in real careers. Decades ago, as a pre-licensure nursing student struggling through my first college chemistry class, I sought guidance from my faculty advisor. Instead of support, I was told, "Maybe you should be a social worker." I pushed through, passed chemistry that summer, and more than forty years later, I hold a doctoral degree in nursing. I've heard nearly identical stories from other Black nurses — being warned the program "could be tough" for them, or that it "might be financially challenging" given their background. These aren't isolated incidents; they're a pattern underrepresented students still face, which is why mentorship and cultural sensitivity training need to be built into how we prepare the next generation of nurses.
Accrediting bodies have taken notice: The Joint Commission and the American Nurses Credentialing Center's Pathway to Excellence program now require healthcare organizations to assess their diversity, equity, and inclusion efforts. That accountability matters — but only if it's backed by real change in how nursing students are taught.
Take the DiversityNursing.com "Unconscious Bias" Quiz Today
Why Cultural Humility Matters More Than Checklists
At the heart of good nursing care is a simple idea: every patient deserves to be treated with dignity. Cultural humility is what makes that possible in practice, asking nurses to bring empathy and genuine curiosity into every patient interaction rather than imposing their own assumptions.
Cultural humility differs from a rigid, fact-based approach to competence: it treats self-awareness as an ongoing practice, not a box to check, requiring nurses to critically examine their own biases continuously. Done well, this fosters what researchers call cultural fluidity — a seamless exchange between a nurse's own values and those of the patients and colleagues around them.
Research backs this up. Arruzza and Chau (2021) found that nursing students are eager to learn about cultural competence but often start out without a clear sense of their own strengths and gaps; structured education leaves them more satisfied and better able to identify their own learning needs. Antón-Solanas and colleagues (2021) found something more sobering: unaddressed implicit and explicit bias can take a real toll on students' mental health and academic performance. This isn't only about patient outcomes — it directly affects whether nursing students, especially those from underrepresented backgrounds, succeed and stay in the profession.
What the Research Says About Getting This Right
The broader literature reinforces the same conclusion: nursing can genuinely help close healthcare disparities when academic programs fully integrate culturally competent education and invest in training faculty to teach it well. But the training itself has to evolve — early cultural competency education often leaned on stereotypes that have since been discredited, and outdated versions can do more harm than good.
Faculty can't be exempt from this work either. Nurse educators need their own cultural competency training to prepare students for multicultural patient care. Yet studies show students still witness racial stereotyping from academic and clinical staff, creating what researchers describe as pressure to be "exceptional to be considered average." Combine that with reduced social support and a shortage of diverse faculty role models, and it's easy to see how it wears down even capable students. Proposed remedies include focusing more on social determinants of health, building genuinely safe clinical learning spaces, and prioritizing the retention of diverse faculty.
Much of today's thinking traces back to Madeleine Leininger's Transcultural Nursing Theory, which established that nurses must recognize and respect the cultural backgrounds, beliefs, and practices of every patient. Programs built around this theory report stronger empathy, sharper critical thinking, and deeper commitment to the profession. The American Association of Colleges of Nursing has since built on this foundation with its Essentials framework. Not every intervention shows the same staying power, though — unconscious bias training shows mixed long-term results, suggesting deeply ingrained biases don't always shift easily.
There's also a broader accountability question. A health profession school's "social mission" should mean more than teaching science well; it means embedding equity into the curriculum itself. Yet a review by Orbán and colleagues (2021) of nine health profession accreditation standards found that none of the nursing accreditation bodies examined explicitly required curricula to address student diversity or health disparities — a real blind spot in how the profession holds itself accountable.
Moving Forward
Cultural competence is necessary, but it's not sufficient on its own. Real progress requires systemic change across healthcare organizations, academic institutions, and the broader socioeconomic conditions that shape health. Every nurse has a role to play: examining personal biases honestly, collaborating openly with colleagues and students, and creating space for students to speak up when something conflicts with cultural sensitivity — an act of patient advocacy in its own right. Clinical training programs should also make room for real-world exposure: rotations in community health clinics, neighborhood health centers, international clinics, and cultural immersion experiences give students something no textbook can — direct contact with the communities they'll eventually serve.
The goal isn't a nurse who has memorized facts about every culture they might encounter. It's a nurse who walks into any room ready to listen, willing to be corrected, and committed to treating the person in front of them with the dignity they deserve.
References
American Association of Colleges of Nursing. (2023). The essentials: Competencies for professional nursing education [PDF]. https://www.aacnnursing.org/Portals/0/PDFs/Publications/Essentials-2021.pdf
Antón-Solanas, I., Tambo-Lizalde, E., Hamam-Alcober, N., Vanceulebroeck, V., Dehaes, S., Kalkan, I., Kömürcü, N., Coelho, M., Coelho, T., Casa Nova, A., Cordeiro, R., Sagarra-Romero, L., Subirón-Valera, A. B., & Huércanos-Esparza, I. (2021). Nursing students' experience of learning cultural competence. PLOS ONE, 16(12), e0259802. https://doi.org/10.1371/journal.pone.0259802
Arruzza, E., & Chau, M. (2021). The effectiveness of cultural competence education in enhancing knowledge acquisition, performance, attitudes, and student satisfaction among undergraduate health science students: A scoping review. Journal of Educational Evaluation for Health Professions, 18, 3. https://doi.org/10.3352/jeehp.2021.18.3
Chae, D., Kim, J., Kim, S., Lee, J., & Park, S. (2020). Effectiveness of cultural competence educational interventions on health professionals and patient outcomes: A systematic review. Japan Journal of Nursing Science, 17(3). https://doi.org/10.1111/jjns.12326
Etienne, S., & Lewis, L. (2024). Racial implicit bias: Perspectives of nursing students. Journal of Professional Nursing, 50, 95–103. https://doi.org/10.1016/j.profnurs.2023.10.007
Hughes, V., Delva, S., Nkimbeng, M., Spaulding, E., Turkson-Ocran, R.-A., Cudjoe, J., Ford, A., Rushton, C., D'Aoust, R., & Han, H.-R. (2020). Not missing the opportunity: Strategies to promote cultural humility among future nursing faculty. Journal of Professional Nursing, 36(1), 28–33. https://doi.org/10.1016/j.profnurs.2019.06.005
Joseph, O., Flint, S. W., Raymond-Williams, R., Awadzi, R., & Johnson, J. (2021). Understanding healthcare students' experiences of racial bias: A narrative review of the role of implicit bias and potential interventions in educational settings. International Journal of Environmental Research and Public Health, 18(23), 12771. https://doi.org/10.3390/ijerph182312771
Key data on health and health care by race and ethnicity. (n.d.). KFF. Retrieved April 3, 2025, from https://www.kff.org/key-data-on-health-and-health-care-by-race-and-ethnicity/?entry=health-coverage-access-to-and-use-of-care-access-to-and-use-of-care
Nursing workforce fact sheet. (n.d.). Retrieved April 3, 2025, from https://www.aacnnursing.org/news-data/fact-sheets/nursing-workforce-fact-sheet
Ogundipe, A., Hylton, D., & Alexander, P. (2023). Inclusion of cultural competence and racial awareness in nursing education: An exploration of the nurse educator role. Nurse Education Today, 120, 105611. https://doi.org/10.1016/j.nedt.2022.105611
Orbán, J., Xue, C., Raichur, S., Misak, M., Nobles, A., Casimir, J., & Batra, S. (2021). The scope of social mission content in health professions education accreditation standards. Academic Medicine, 97(1), 111–120. https://doi.org/10.1097/acm.0000000000004437
Pryce-Miller, M., Bliss, E., Airey, A., Garvey, A., & Pennington, C. R. (2023). The lived experiences of racial bias for black, Asian and minority ethnic students in practice: A hermeneutic phenomenological study. Nurse Education in Practice, 66, 103532. https://doi.org/10.1016/j.nepr.2022.103532
The future of nursing 2020-2030: Charting a path to achieve health equity. (n.d.). https://nap.nationalacademies.org/catalog/25982/the-future-of-nursing-2020-2030-charting-a-path-to
U.S. Census Bureau. (n.d.). 2020 U.S. population more racially, ethnically diverse than in 2010. U.S. Department of Commerce. Retrieved April 3, 2025, from https://www.census.gov/library/stories/2021/08/2020-united-states-population-more-racially-ethnically-diverse-than-2010.html
Vela, M. B., Erondu, A. I., Smith, N. A., Peek, M. E., Woodruff, J. N., & Chin, M. H. (2022). Eliminating explicit and implicit biases in health care: Evidence and research needs. Annual Review of Public Health, 43(1), 477–501. https://doi.org/10.1146/annurev-publhealth-052620-103528
Vella, E., White, V. M., & Livingston, P. (2022). Does cultural competence training for health professionals impact culturally and linguistically diverse patient outcomes? A systematic review of the literature. Nurse Education Today, 118, 105500. https://doi.org/10.1016/j.nedt.2022.105500
 In our growing diverse society, health care workers need to understand that applying only traditional westernized medical practices isn't appropriate for many patients and families. Health professionals must have an awareness of different cultural practices and spiritual beliefs in order to reduce racial and ethnic disparities in health care.
In our growing diverse society, health care workers need to understand that applying only traditional westernized medical practices isn't appropriate for many patients and families. Health professionals must have an awareness of different cultural practices and spiritual beliefs in order to reduce racial and ethnic disparities in health care.
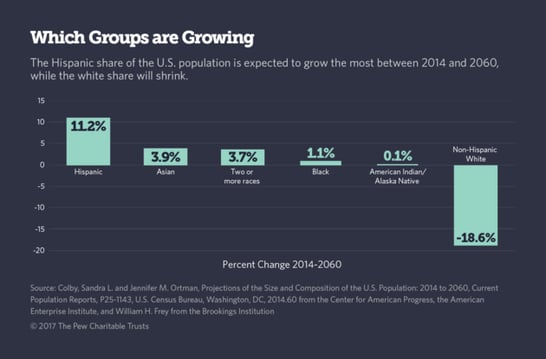
 The U.S. population is growing increasingly diverse. By 2020, the U.S. Census Bureau projects less than 50% of the children in the U.S. will be non-Hispanic and Caucasian. With demographics shifting, health care professionals trained in cultural competence will meet the needs of community health more effectively. Nurse practitioners earning their
The U.S. population is growing increasingly diverse. By 2020, the U.S. Census Bureau projects less than 50% of the children in the U.S. will be non-Hispanic and Caucasian. With demographics shifting, health care professionals trained in cultural competence will meet the needs of community health more effectively. Nurse practitioners earning their

 Frontier Nursing University conference discusses healthcare diversity
Frontier Nursing University conference discusses healthcare diversity
 Depending upon your physical location of employment, whether it’s in the city, suburbs or rural area, you may encounter language barriers with your patients every day or maybe only once or twice a year. Whatever the frequency is for you, it’s important that the information you have to deliver is conveyed as clearly as possible. Some medical terms we use here in the US may not have clear translations in your patient’s native language.
Depending upon your physical location of employment, whether it’s in the city, suburbs or rural area, you may encounter language barriers with your patients every day or maybe only once or twice a year. Whatever the frequency is for you, it’s important that the information you have to deliver is conveyed as clearly as possible. Some medical terms we use here in the US may not have clear translations in your patient’s native language. Growing up, we were taught to be modest. As we became adults and more comfortable with who we are as a person, modesty may have become more important in our lives, or perhaps, less important. It depends on our personal circumstances and beliefs.
Growing up, we were taught to be modest. As we became adults and more comfortable with who we are as a person, modesty may have become more important in our lives, or perhaps, less important. It depends on our personal circumstances and beliefs. How can you properly care for a patient if you don’t understand their personal needs? Communication is key. Making a patient comfortable goes far beyond providing warm blankets. It is about the patient trusting you and knowing you have things in common that show them you understand how they feel and what they need.
How can you properly care for a patient if you don’t understand their personal needs? Communication is key. Making a patient comfortable goes far beyond providing warm blankets. It is about the patient trusting you and knowing you have things in common that show them you understand how they feel and what they need. 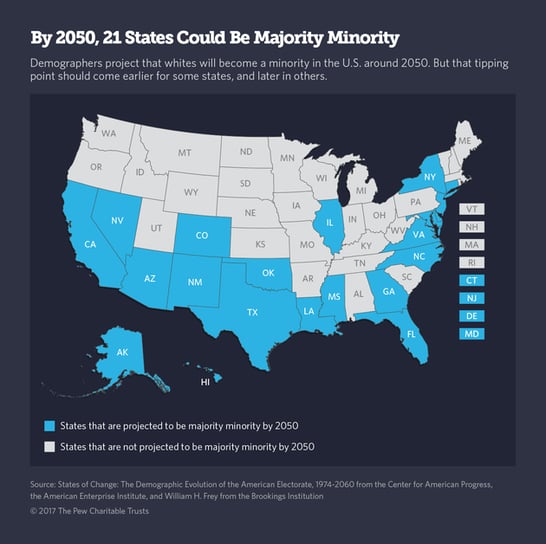

 Cultural respect is vital to reduce health disparities and improve access to high-quality healthcare that is responsive to patients’ needs, according to the
Cultural respect is vital to reduce health disparities and improve access to high-quality healthcare that is responsive to patients’ needs, according to the 