
 Being able to read, write, and speak a second language is a highly desired skill in almost every career. However, being a Multilingual or Bilingual Nurse within the healthcare industry has some exceptionally high benefits that make such skilled individuals a prized asset to any team.
Being able to read, write, and speak a second language is a highly desired skill in almost every career. However, being a Multilingual or Bilingual Nurse within the healthcare industry has some exceptionally high benefits that make such skilled individuals a prized asset to any team.
This is especially true in the United States where there's an influx of non-English speaking individuals. In fact, the US now has 41 million native Spanish speakers with another 11.2 million people using it as their second language. That's more people speaking Spanish in the US than all of Spain!
All of these native Spanish speakers, along with other non-English speakers, require healthcare services which emphasizes the value of having bilingual staff on hand. Consider these benefits of being a Bilingual Nurse:
- Numerous Job Opportunities. Most hospitals, clinics, insurance companies, schools and other healthcare organizations are centered around major cities, most of which contain high immigrant populations with areas of mega-cities dedicated to specific cultural groups. Take for example Miami's famed Cuban neighborhood entitled Little Havana or Seattle's bustling Little Saigon, the economic and social center of the region's Vietnamese community. Every one of the healthcare offices servicing these areas is in need of trained and experienced Nurses that can communicate directly with patients who aren't fluent in English. This means high demand and significant income opportunities for the flexible and Bilingual Nurse.
- Satisfaction for Helping a Diverse Population. Many individuals pursue Nursing out of a desire to help others. A Bilingual Nurse is in a unique position to significantly improve the quality of care patients receive due to their ability to not only assist them in the routine ways, but also to help them better understand medical terms, symptoms, and treatment options in their native tongue.
- Added Value to Employers. Individuals pursuing a MSN degree that are also able to speak a second language, enhance their potential worth to their employer. A Bilingual Nurse can converse and assist more diverse groups of people to better market the employer's organization as being open and welcoming to people from different language and cultural backgrounds.
- Exciting Foreign Job Prospects. Some people are born with an itch to travel, and being bilingual is perhaps the single biggest factor in fulfilling that desire. That's because the ability to speak another language, translate, and converse opens doors to employers in non-English speaking countries.
- Critical to Ensuring Data is Accurate. In this digital age of computers and consolidated electronic health records, it's important to stay on top of data input and security. Most larger hospitals and healthcare organizations have some basic translation services at their disposal to help with patients who are not native English speakers, but this often isn't the case with smaller offices, clinics, and other practices. And even if they do, too frequently errors in translations can come up. That's why it's so important for these organizations to keep a staff of Bilingual Nurses on hand to help collect information from the patient themselves and ensure that client files are correctly uploaded and stored. This provides inherent benefits both to accurate record keeping and patient safety.
In the end, not only are there many great benefits to being a Bilingual Nurse, but it's very important for healthcare organizations, whether they're large hospital systems or specialized clinics, to have Nurses with multiple language capabilities. The world today is becoming ever more diverse and interconnected. The ability to speak multiple languages alongside nursing or doctoring skills, is a very valuable and marketable commodity that also helps improve patient outcomes and safety.


 Technology has made people's lives much easier. There are specialized apps for almost everything and everyone. Some very helpful technology exists for Nurses designed to make your life easier. Here’s the 2015 Top 10.
Technology has made people's lives much easier. There are specialized apps for almost everything and everyone. Some very helpful technology exists for Nurses designed to make your life easier. Here’s the 2015 Top 10. How can you tell if a burn wound has become infected? Wouldn’t it be great if a new technology can alert you to an infection without having to remove the bandage? Scientists in the UK are in the development phase of a bandage that changes color to alert you to an infection. As you know, antibiotics are often prescribed to help stave off infection, however this new technology may help prevent the need for antibiotics.
How can you tell if a burn wound has become infected? Wouldn’t it be great if a new technology can alert you to an infection without having to remove the bandage? Scientists in the UK are in the development phase of a bandage that changes color to alert you to an infection. As you know, antibiotics are often prescribed to help stave off infection, however this new technology may help prevent the need for antibiotics.

 If you’re feeling unappreciated, read this story to know that many people very much appreciate what you do. They’re not always very good at expressing themselves in a positive way. But most of you understand your patients feelings because as this husband explains, they’re going through one of the worst days of their lives. Many of my friends are Nurses and they are awesome just like you, Every Day.
If you’re feeling unappreciated, read this story to know that many people very much appreciate what you do. They’re not always very good at expressing themselves in a positive way. But most of you understand your patients feelings because as this husband explains, they’re going through one of the worst days of their lives. Many of my friends are Nurses and they are awesome just like you, Every Day.
 If you’re thinking about continuing your education, this article offers some important questions to consider in helping you decide if an online program will accomplish what you want to achieve. We all know continuing your education, if at all possible both financially and personally, will enhance your career, your life and your earning potential.
If you’re thinking about continuing your education, this article offers some important questions to consider in helping you decide if an online program will accomplish what you want to achieve. We all know continuing your education, if at all possible both financially and personally, will enhance your career, your life and your earning potential.
 It seems that Google is involved in just about everything these days! Here’s the latest announcement. The American Heart Association is teaming up with Google on a project for heart health and conquering heart disease. Hopefully their huge investment will yield some promising results for everyone.
It seems that Google is involved in just about everything these days! Here’s the latest announcement. The American Heart Association is teaming up with Google on a project for heart health and conquering heart disease. Hopefully their huge investment will yield some promising results for everyone. Most of us have heard of macular degeneration, which eventually robs people of their eyesight. But, have you heard about a new procedure done at UC Davis Medical Center that has restored a woman’s eyesight? The patient led a very interesting career for 40+ years and started losing her eyesight shortly after retirement. Due to a new technology, she can now see her friends and family’s faces, read and enjoy the beautiful sights around her.
Most of us have heard of macular degeneration, which eventually robs people of their eyesight. But, have you heard about a new procedure done at UC Davis Medical Center that has restored a woman’s eyesight? The patient led a very interesting career for 40+ years and started losing her eyesight shortly after retirement. Due to a new technology, she can now see her friends and family’s faces, read and enjoy the beautiful sights around her.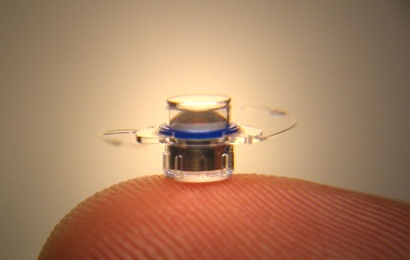 In a first-of-its-kind procedure for Northern California, UC Davis doctors implanted a pea-sized telescope in Bane’s eye, gradually restoring her ability to see faces, colors and print. Today the 92-year-old still enjoys reading, seeing friends and living independently – thanks to both her pioneering spirit and what she fondly calls her “bionic eye.”
In a first-of-its-kind procedure for Northern California, UC Davis doctors implanted a pea-sized telescope in Bane’s eye, gradually restoring her ability to see faces, colors and print. Today the 92-year-old still enjoys reading, seeing friends and living independently – thanks to both her pioneering spirit and what she fondly calls her “bionic eye.” Here’s an interesting article about how to make the mentor/mentee relationship work through a
Here’s an interesting article about how to make the mentor/mentee relationship work through a 
 As the Nursing shortage continues so does the need for Nurse Educators. We thought you’d enjoy this article
As the Nursing shortage continues so does the need for Nurse Educators. We thought you’d enjoy this article