
Healthcare organizations must know in order to be successful, you need a diverse workforce. The key to success in this area is retaining that staff and knowing how to defuse conflicts. This is especially true in settings like hospitals, where mistakes can mean life or death.
Poor communication is one of the leading causes of medical errors, according to the Joint Commission. Medical errors are the 3rd leading cause of death in the United States—right after heart disease and cancer, and it’s more prevalent than respiratory ailments, stroke and Alzheimer's disease—according to a study out this year from The BMJ. Author Martin Makary, MD, of Johns Hopkins University, and colleagues estimate that 251,000 Americans die each year from such mistakes. Some instances have nothing to do with interpersonal conflict, but employees at odds with one another are less likely to spend time making sure they understand each other during crucial events like a patient hand-off.
Dianne Austin, workforce diversity program manager at Massachusetts General Hospital, told Healthcare Dive, creating robust support networks is key to helping employees identify and deal with tension or potential discrimination from other employees. They also need to be able to talk freely with others who may be in similar situations. “There’s a lot that we do to really try to help employees feel that they have a voice and that they’re important,” she said.
How conflict happens
Susan Woods, a workplace consultant, says there are a few major dynamics in diversity-related conflict, including respect and disrespect, as well as recognition and identity.
1) Respect and Disrespect
Disrespect may be gross and blatant, but it is also subtle, communicated in the little
ways someone is told they don’t belong, are not good enough, are not expected to
achieve, or that they can be overlooked and don’t count.
Remarks like the ones below convey messages about respect.
“Not a bad job, for a woman.”
“You don’t have to worry about your appointment. You’re a minority.”
“That company is very traditional. I’m surprised they even hired you.”
A reasonable person could interpret disrespect in each of these messages. The
harmful message may be unintended and unrecognized by the offending party, even
as it is deeply felt by the offended party.
When disrespect is communicated in unintended and unconscious ways, bringing
this perspective to the surface creates an opening for learning and improved
relations. Regardless of how the incident in question is settled, failure to understand
the dynamics of respect and disrespect from more than one perspective perpetuates
the underlying conflict.
2) Recognition and Identity
A second dynamic often present in diversity-related conflict resolution is
recognition and identity. Recognition and identity are complicated dynamics, full of
opportunity for misunderstanding and tension. These may have a negative effect,
but may not have been communicated with consciously malicious intent.
We hear it below:
“I’m always asked to be in the photo or meet with visitors because I’m one of the few people of color
they have. It has nothing to do with my accomplishments.”
“I hope you’re not asking me to take the minutes because I’m the only woman in the group.”
“You’re not like the others. I feel I can talk with you.”
“Those people …”
The old days of the “great melting pot,” where everyone was expected to conform
to the dominate group, are gone. Hopefully, we’ve moved past assimilation to
realize that inclusion is about recognizing diverse identity. It’s about understanding
individuals as unique persons and, at the same time, as members of groups.
Either/or logic is misleading. This is a both/and phenomenon. The ambiguity can
be unsettling, especially when the challenge is so deeply personal and emotional as
with identity.
Research shows that conflict can be frequent in healthcare organizations because of the high workload volumes, pressures to move quickly and the importance of decisions being made. These conflicts can affect companies in many ways, including high staff turnover rates, reduced productivity and litigation costs.
Dealing with conflicts
The best processes start early and attempt to prevent conflict. Austin said Massachusetts General has an orientation where new employees attend a program on diversity and inclusion and learn about various resources available to employees, such as a citizenship program, careers days and school admissions officers. There are also multiple staff committees focused on improving diversity and inclusion.
Healthcare managers can help ease conflict by listening carefully to employees, quickly addressing the source of the problem, instituting strict and clear policies and educating staff about those policies, she wrote.
Massachusetts General has multiple ways for an employee to bring any concerns to light, including an anonymous hotline, Austin said. The HR department will review whatever is submitted and the relevant department head is told the details. “We really try to pull managers and the appropriate people in so we can get to the bottom of it based on the information provided,” she said.
Sometimes, the problem starts with a patient who refuses to be cared for by a certain nurse or doctor, and may use racial slurs or other inappropriate language. The nurse manager will respond and tell the patient all providers are equally trained and capable. The patient is then told they can go to another hospital if they will not be respectful to all employees. The affected employee can decide whether or not to continue working with the patient.
Diversity is needed at higher ranks
Diversity and inclusion efforts should reach all the way up the ranks to the executives, making sure their C-suites and boardrooms are also diverse and reflective of the surrounding community.
The American Hospital Association's Institute for Diversity in Health Management released a comprehensive report titled Diversity and Disparities: A Benchmarking Study of U.S. Hospitals in 2015. The results of the survey were not exactly positive. In fact, the survey found that minority representation on healthcare boards across this nation stood at just 14%—precisely the same percentage reported in a similar survey two years earlier and a similar study conducted in 2011.
Deborah Bowen, president of the American College of Healthcare Executives said the best ways to remedy poor diversity in C-suites is to start cultivating a diverse group of people who have an interest in leadership early on in their careers. Post-graduate fellowship programs and scholarship for mid-level executives can be helpful. Hospitals should provide leadership development and training as well as other career resources, she said.
“It’s a matter of finding mentors, for example,” she said. “Have a mentorship network to find somebody who has gone through something similar.”
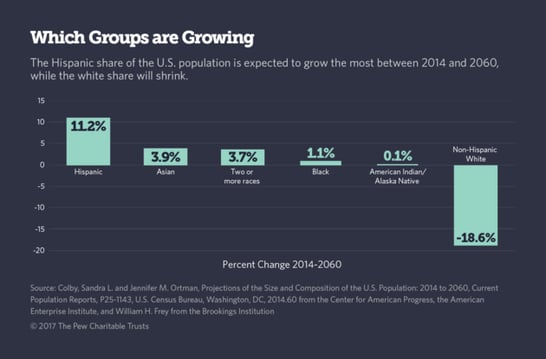
The diversity of people in the US has changed considerably. As stated at the beginning of this article, our hospital and healthcare system employees need to reflect their patient population at all levels within their organization(s). Sensitivity to language, cultural, sexual, and physical differences in both your staff and patients is critical for a harmonious and productive environment.


 The eighth annual Diversity Impact 2018 Student Conference will be held June 7-10, 2018, on FNU’s historic campus in Kentucky. This event is hosted by the Diversity PRIDE student organization and is open to all attendees who want to become part of FNU’s legacy of providing care to rural and underserved communities.
The eighth annual Diversity Impact 2018 Student Conference will be held June 7-10, 2018, on FNU’s historic campus in Kentucky. This event is hosted by the Diversity PRIDE student organization and is open to all attendees who want to become part of FNU’s legacy of providing care to rural and underserved communities. Meet FNU's New Chief Diversity and Inclusion Officer Dr. Maria Valentin-Welch, DNP, MPH, CDP, CNM, FACNM.
Meet FNU's New Chief Diversity and Inclusion Officer Dr. Maria Valentin-Welch, DNP, MPH, CDP, CNM, FACNM. Hyden, KY --
Hyden, KY -- FNU’s chief diversity and inclusion officer (CDIO) will lead the development of a vision and strategy that champions the importance of a diverse and inclusive environment that values and supports all members of the University community. The addition of the CDIO position is the most recent of a number of diversity initiatives implemented as part of FNU’s strategic plan to heighten the focus on diversity and inclusion for all faculty, staff and students. The CDIO will serve on the executive team along with the president, dean, chief operations officer and the executive vice president for finance and facilities.
FNU’s chief diversity and inclusion officer (CDIO) will lead the development of a vision and strategy that champions the importance of a diverse and inclusive environment that values and supports all members of the University community. The addition of the CDIO position is the most recent of a number of diversity initiatives implemented as part of FNU’s strategic plan to heighten the focus on diversity and inclusion for all faculty, staff and students. The CDIO will serve on the executive team along with the president, dean, chief operations officer and the executive vice president for finance and facilities. Hyden, KY --
Hyden, KY -- 

 Frontier Nursing University conference discusses healthcare diversity
Frontier Nursing University conference discusses healthcare diversity Unique challenges encompass the delivery of quality healthcare in the entire world as a whole. People of all ages are terminally ill -- with approximately half the American population fighting hypertension, diabetes, cardiovascular diseases, arthritis and mental related illness.
Unique challenges encompass the delivery of quality healthcare in the entire world as a whole. People of all ages are terminally ill -- with approximately half the American population fighting hypertension, diabetes, cardiovascular diseases, arthritis and mental related illness. How can you properly care for a patient if you don’t understand their personal needs? Communication is key. Making a patient comfortable goes far beyond providing warm blankets. It is about the patient trusting you and knowing you have things in common that show them you understand how they feel and what they need.
How can you properly care for a patient if you don’t understand their personal needs? Communication is key. Making a patient comfortable goes far beyond providing warm blankets. It is about the patient trusting you and knowing you have things in common that show them you understand how they feel and what they need. 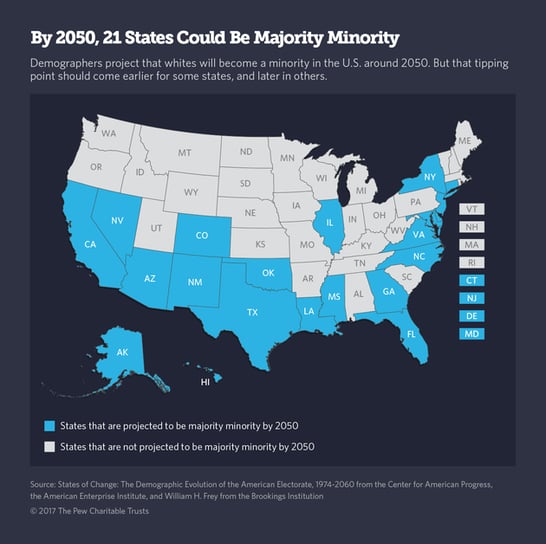

 Recruiting these days is getting more and more difficult, particularly when hiring Nurses. We’re featuring this article because of its creative approach to thinking outside the box. Perhaps it’s time to change your message, how and where you target that message, and maybe even the position requirements.
Recruiting these days is getting more and more difficult, particularly when hiring Nurses. We’re featuring this article because of its creative approach to thinking outside the box. Perhaps it’s time to change your message, how and where you target that message, and maybe even the position requirements.
 DiversityNursing.com would like to share this article with you. It features an interview with
DiversityNursing.com would like to share this article with you. It features an interview with