The headline and subheader tells us what you're offering, and the form header closes the deal. Over here you can explain why your offer is so great it's worth filling out a form for.
Millions of people could be trying to measure their blood pressure with untested, inaccurate and potentially dangerous smartphone applications, or apps, a new study finds.
Researchers analyzed the top 107 apps for "hypertension" and "high blood pressure" that are available for download on the Google Play store and Apple iTunes and found that nearly three-quarters offered useful tools for tracking medical data.
But they also found seven Android apps that claimed users needed only to press their fingers onto phone screens or cameras to get blood-pressure readings - claims that scientists say are bogus.
"This technology is really in its nascent stages, and it's not quite ready for prime time," lead author Dr. Nilay Kumar told Reuters Health.
Kumar, an attending physician at the Cambridge Health Alliance in Cambridge, Massachusetts and a Harvard Medical School instructor, was surprised to learn that apps marketed as turning smartphones into blood pressure measuring devices had been downloaded at least 900,000 times and as many as 2.4 million times.
"That's concerning that such a small number of apps have been downloaded so many times," he said. "We were surprised by the popularity."
He wasn't sure how the technology supposedly works but said the phone camera appears to read a finger pulse.
"It's really in a research-and-development stage. It's not ready for clinical use. For now, we need to be careful that we are not using things that are inaccurate and could be potentially dangerous," he said.
Apps that inaccurately measure blood pressure could lead to false alarms and possibly fatal false assurances, Kumar said.
About one in three American adults has high blood pressure, according to the U.S. Centers for Disease Control and Prevention. Also known as hypertension, the condition has been called the silent killer because it often shows no warning symptoms but increases the risk of heart disease and stroke, two leading causes of death.
A growing number of hypertension patients use mobile-health technologies to track and manage their conditions, the authors write in the Journal of the American Society of Hypertension.
The study, conducted earlier this year, in general found good news about blood pressure apps. The majority, or 72 percent, of the most popular apps allowed consumers to keep track of their medical data. About a quarter could directly export recorded information to physicians' offices. And nearly a quarter included tools to enhance medication adherence.
But healthcare agencies, such as universities, helped develop only a tiny fraction of the apps, 2.8 percent, the study found.
The U.S. Food and Drug Administration (FDA), which regulates medical devices, has not approved any of the blood pressure apps, the authors write.
The study's findings raise "serious concerns about patient safety" and reveal an "urgent need for greater regulation and oversight in medical app development," the authors say.
Dr. Karen Margolis, an internist and director of clinical research at HealthPartners Institute for Education and Research in Minneapolis, would also like to see more oversight.
"The idea that you're going to be able to stick your finger on the camera of your smartphone and get an accurate blood pressure reading is pretty farfetched right now," she told Reuters Health.
Margolis has studied devices to measure blood pressure but was not involved in the current study.
"There is virtually no information at all about how accurate these apps are," she said. "It doesn't sound to me like it's ready for routine use in any way that medical decisions could be based on."
Regulatory authority over smartphone apps that can be turned into medical devices remains unclear, Kumar said.
Writing earlier this year in The New England Journal of Medicine, a group of three lawyers, led by Nathan G. Cortez of the Southern Methodist University Dedman School of Law in Dallas, Texas, warned that mobile health, or mHealth, poses a challenge for the FDA.
"Many members of Congress and industry believe that regulation will stifle mHealth innovation," the lawyers wrote. "The true challenge, however, is creating a regulatory framework that encourages high-value innovation while also preventing the market from being overcome with products that are ineffective or unsafe."
Adopting a stray dog while in the midst of battling a disease that was deemed incurable hardly seems like the best timing, yet that’s exactly what Bill Hogencamp and his wife Kathy decided to do.
They believe that decision helped save his life.
Hogencamp, an 84-year-old semi-retired architect from Phenix, Alabama, was diagnosed with incurable cancer of the gall bladder, liver, colon and the lining of his abdomen back in May. Doctors told him he wouldn’t live to see Christmas.
“I have seven children and I’ve traveled all around the world,” Hogencamp said. “I thought if this is it, then this is it.”
Hogencamp chose to undergo treatment even though his doctor told him there was no hope, he recalled. In October, he had an operation to remove three large tumors.
Eleven days after his surgery, his wife was on her way to pick him up from a rehabilitation facility when she spotted a small white dog wandering down the middle of the road, in danger of being hit by a car. Although she was in a rush, she said something compelled her to stop and rescue the pup.
“He walked past six other cars right up to the side of my car and put his paws up on the door,” she recalled.
While his wife was hooked on the cute little dog right away, Hogencamp needed some convincing.
“I hadn’t had a dog in twenty years and I had no desire to have a dog,” he said. “I kept saying we need to find his owner.”
Despite an extensive search and nearly a dozen false leads, the Hogencamps were never able to track down the dog’s owner. They learned from a vet they visited during their search that he was a Maltese, probably around 6 years old, fixed but not chipped.
Besides, the dog very quickly won Hogencamp over. They soon became inseparable.
Whenever Hogencamp sat down, the dog -- who they named Mahjong after Kathy’s favorite card game -- would jump in his lap. Whenever Hogencamp napped, Mahjong would curl up next to him. When Hogencamp returned home after being out, Mahjong would hop onto his hind legs and dance with joy.
As he and his wife settled into life with a dog, Hogencamp underwent chemotherapy. Just before the holiday he received some miraculous news: Tests showed that he was now cancer free.
The doctors are at a loss to explain this amazing turn of events, Hogencamp’s wife said. But she said the family believes that Mahjong has played a huge part in her husband’s recovery.
“The dog seemed to know right away that Bill was sick and it was his job to take care of him -- and Bill knew it was his job to take care of the dog,” she said.
Hogencamp agreed. He said their relationship gave both him and the dog a sense of purpose. Although he knows he owes much of his cure to great medical care and a lot of luck, he said that he is convinced the little white dog was sent to him to help him get better.
As they celebrate Christmas, Hogencamp said he has two final chemotherapy treatments. He said he’s spending the day with friends, family and of course, Mahjong.
“My life has been a miracle,” Hogencamp said. “And now Mahjong is part of that miracle.”
Even before she had a groom in mind, Katie Breland Hughes knew she wanted to walk down the aisle at her wedding on her own two feet.
It became one of her initial goals after a horrific car accident left her paralyzed from the waist down. But first, she needed to survive her injuries.
“Honestly, I had so many skin graft surgeries and so many burns, my first goal was just to sit up in the bed," said Hughes, now 27. "I was literally at rock bottom."
In October 2011, the Louisiana personal trainer and physical therapy assistant missed a stop sign while driving home from an appointment with a client. A truck hit her vehicle broadside, and Hughes went flying through her windshield. She landed in a ditch and, seconds later, her burning car landed on top of her, searing her back.
Conscious throughout the ordeal, Hughes knew she was either paralyzed or that her legs were amputated because she couldn’t feel either one.
“Immediately, I started asking myself all the physical therapy questions. Is my spinal cord severed? What kind of injury is this? How far up? How low down?” she recalled for TODAY.com.
At the hospital, doctors told Hughes that she would never walk again. But during a nine-hour surgery to insert rods and plates along her spine to stabilize it, they learned that Hughes' spinal cord wasn’t severed as they originally thought.
“That was all I needed to hear to keep pushing forward,” she said. “That was kind of my prayer.”
After her 100-day hospital stay, Hughes went home and immediately started training. An athlete all her life —she was supposed to run a marathon the week after her crash — exercise had always given Hughes an emotional outlet. After the accident, her love of exercise proved critical to her recovery, and to attaining the new goal she had created for herself.
“I told my sister from the beginning, I will not get married — whoever it be to, or whenever it happens — I will not do it until I can walk down the aisle. I just won’t be in a wheelchair,” she said. “So that was always a goal. I didn’t know the next year it would actually happen.”
Hughes heard about a Michigan trainer who had worked with other paraplegics. She reached out to him and flew to Michigan to begin training.
“The first time I talked to her on the telephone, she was like, ‘Look, I don’t want to be in this chair forever. I understand what happened to me, but I want to work hard and see where I can get,’” said Mike Barwis, a strength and conditioning coach who frequently works with Olympic and professional athletes.
It was during a session with Barwis that Hughes moved her legs for the first time since the accident.
Meanwhile, Hughes had reconnected with a former acquaintance, Odie Hughes. She initially worried about meeting him again now that she was in a wheelchair.
“I didn’t know how he would accept that, or how he would feel about that,” she recalled. “But it was like he never even saw the chair, he just saw me. He believed everything with me. If I told him, ‘I think I can do this. I want to try this,’ then he would be my biggest cheerleader.”
Within three months, they were engaged. Hughes started the clock: She had nine months to get on her feet. Barwis said he had no doubts they could make it happen.
“Katie is a vibrant person. She has an amazing personality and she’s very driven,” he said. “Her mentality has been one of absolute determination.”
But while working to build up the strength in her legs, Hughes also had to plan a wedding. She also opened a gym she started in her community of Bogalusa, about 70 miles north of New Orleans.
There was also the issue of finding a wedding gown.
“I actually bought three dresses. I didn’t like any of them,” she said. After getting ready to settle on one of them, she received a call from the cable network TLC, asking if she wanted to be featured on the show, “Say Yes to the Dress.” Hughes flew to the Atlanta bridal store featured on show (the episode airs Jan. 2) and finally found a gown she was happy with.
“Everything about it was perfect,” she said.
Except she never practiced walking in it until the day of her wedding. "I didn’t want anybody to see the real one," she explained. So instead, she practiced using one of the other gowns. She started in a full-body brace, then with a walker before moving on to two canes. Finally, she used two leg braces that went up from her feet to just above the knees, all while holding on to a person on each side of her.
On her wedding day, Sept. 20, Hughes walked down the aisle, on her own two feet, holding the hands of the two men giving her away: Her dad, who stood to her right, and Barwis, on her left.
As excited as she was, Hughes said she never anticipated the nerves she experienced as she stared down the aisle at her guests.
“I felt like this was everybody’s fairytale ending. This was the story they had been following for so long and this was the ending they were waiting to see,” she said. “So I felt like there was a lot of pressure but there was no greater reward than getting to the end of that aisle, for sure.”
Waiting for her there with a huge smile was her fiance.
"When her foot caught that slip my heart stopped. But she just held it together like a champ," said Odie Hughes. "I had complete faith in her."
He said he never for a second doubted the woman he considers "the most stubborn person I know"
"When she said she was gonna do it, it was a done deal," he said. "Never one doubt in my mind she'd not only make it down the aisle but she'd do it in dramatic fashion. That's my Katie."
Months later, Katie is back at work, keeping busy with her physical therapy patients and running her gym, Katie's Shed, where she teaches various cardio and full-body workout classes.
She enjoys newlywed life and said it helps to have a partner who is familiar with life-altering injuries: Her husband once broke his neck during a car accident that left him with metal rods in his legs.
“Me and him both just really understand how quick this life is and how short it can be made,” she said. “We really value each other and the time we have together and with our family. We know first hand how quickly it can be taken from you, so we try to make the best of that.”
Hughes still uses her braces, alternating between them and her wheelchair, depending on the circumstances.
She speaks at local and regional events about her accident and hopes her story will inspire others to reach beyond traditional expectations.
“A lot of people would say, ‘Okay, I did it and now I’m going to be content with my progress right now.’ But I think contentment is our worst enemy a lot of times, just being content with where you are,” she said. “You should always try to excel forward and move forward and continue to reach goals and set new ones.”
A steady diet of fast food might hurt your child in the classroom, a new study finds.
Kids who frequently ate fast food in fifth grade lagged behind by eighth grade, said researchers who reviewed questionnaires and test scores of more than 8,500 U.S. students.
"The largest effects were found for the kids who reported daily consumption of fast food," said study leader Kelly Purtell, assistant professor of human sciences at Ohio State University. "On average they were scoring three or four points lower than the kids who did not report eating fast food at all in the past week."
The researchers compared academic test scores in reading, math and science for fifth and eighth grade and looked at the students' responses to food questions on a national survey.
On average, test scores increased 16 to 19 points, depending on the subject, Purtell said.
But kids who ate fast food the most had test-score gains of up to 20 percent less than those who never ate fast food, she found.
The study was published online this month in Clinical Pediatrics.
More than two-thirds of the students surveyed reported some fast-food intake. And one in five had eaten at least four fast-food meals in the previous week, the survey found.
The amount of fast food consumed corresponded with eighth-grade scores, even after researchers took into account for physical activity, TV watching, income levels and school characteristics, Purtell said.
The proliferation of fast food is already a concern because of America's obesity epidemic.
However, the study can't prove the fast food caused the lower scores, only that the two were linked, Purtell noted. Still, other research has linked high-sugar and high-fat diets with an adverse effect on learning processes requiring attention, she said.
Although researchers can't explain the tie-in for sure, it's also possible that those with a fast-food habit may not get the nutrients needed for good learning, she suggested.
Experts aren't recommending you ban all fast foods on the basis of this one report, but they do advise moderation.
"It is premature to presume that frequent fast-food consumption will compromise one's later academic functioning," said Dr. Andrew Adesman, chief of developmental and behavioral pediatrics at the Steven & Alexandra Cohen Children's Medical Center of New York, who wasn't involved in the study.
"Although this study found an association between frequently eating fast food and weaker academic performance a year later, we cannot be certain that the observed differences were due to nutritional factors and not other variables," he said.
Still, it's advisable to "encourage kids to go slow when it comes to fast food" to preserve health and good nutrition, Adesman added.
More research is needed, he said, to determine what impact fast food has on students' learning potential.
In the meantime, Purtell said, "I don't think the occasional fast meal is anything to worry about." Once a week or less might be a good goal, she suggested.
Gay men who've abstained from sex for one year would be able to donate blood in 2015, ending a lifetime ban for the gay community, under a proposed FDA policy change unveiled Tuesday.
The current lifetime ban by U.S. Food and Drug Administration states dates back to 1983 and forbids men who have had sex with men from becoming blood donors because the group is "at increased risk for HIV, hepatitis B and certain other infections that can be transmitted by transfusion," the FDA has ruled.
But the FDA is now seeking a change in that policy and would allow such blood donations based on an independent expert advisory panel's recommendation, the agency said.
The proposed change would align the one-year deferral period "with that of other men and women at increased risk for HIV infection," the FDA said.
The agency will be gathering public comments on the proposed change.
"We encourage all stakeholders to take this opportunity to provide any information the agency should consider, and look forward to receiving and reviewing these comments," FDA Commissioner Margaret A. Hamburg said in a statement.
The National Heart Lung and Blood Institute and the FDA would monitor a national blood surveillance system to see any effects of the proposed policy change and to ensure the continued safety of the blood supply, Hamburg said.
"A history of male-to-male sex is associated with an increased risk for exposure to and transmission of certain infectious diseases, including HIV, the virus that causes AIDS," the FDA said. Men who have had sex with other men represent approximately 2% of the U.S. population, yet are the population most severely affected by HIV, according to the FDA.
In 2010, male-to-male sex accounted for at least 61% of all new HIV infections in the United States, and "an estimated 77% of diagnosed HIV infections among males were attributed to male-to-male sexual contact," the FDA said.
In 2014, Americans say nurses have the highest honesty and ethical standards. Members of Congress and car salespeople were given the worst ratings among the 11 professions included in this year's poll. Eighty percent of Americans say nurses have "very high" or "high" standards of honesty and ethics, compared with a 7% rating for members of Congress and 8% for car salespeople.
Americans have been asked to rate the honesty and ethics of various professions annually since 1990, and periodically since 1976. Nurses have topped the list each year since they were first included in 1999, with the exception of 2001 when firefighters were included in response to their work during and after the 9/11 attacks. Since 2005, at least 80% of Americans have said nurses have high ethics and honesty. Two other medical professions -- medical doctors and pharmacists -- tie this year for second place at 65%, with police officers and clergy approaching 50%.
Historically, honesty and ethics ratings for members of Congress have generally not been positive, with the highest rating reaching 25% in 2001. Since 2009, Congress has ranked at or near the bottom of the list, usually tied with other poorly viewed professions like car salespeople and -- when they have been included -- lobbyists, telemarketers, HMO managers, stockbrokers and advertising practitioners.
Although members of Congress and car salespeople have similar percentages rating their honesty and ethics as "very high" or "high," members of Congress are much more likely to receive "low" or "very low" ratings (61%), compared with 45% for car salespeople. Last year, 66% of Americans rated Congress' honesty and ethics "low" or "very low," the worst Gallup has measured for any profession historically.
Other relatively poorly rated professions, including advertising practitioners, lawyers, business executives and bankers are more likely to receive "average" than "low" honesty and ethical ratings. So while several of these professions rank about as low as members of Congress in terms of having high ethics, they are less likely than members of Congress to be viewed as having low ethics.
No Professions Improved in Ratings of High Honesty, Ethics Since 2013
Since 2013, all professions either dropped or stayed the same in the percentage of Americans who said they have high honesty and ethics. The only profession to show a small increase was lawyers, and this rise was small (one percentage point) and within the margin of error. The largest drops were among police officers, pharmacists and business executives. But medical doctors, bankers and advertising practitioners also saw drops.
Honesty and ethics ratings of police dropped six percentage points since last year, driven down by many fewer nonwhite Americans saying the police have high honesty and ethical standards. The clergy's 47% rating last year marked the first year that less than 50% of Americans said the clergy had high ethical and honesty standards -- and the current 46% rating is, by one percentage point, the lowest Gallup has measured for that profession to date.
Bottom Line
Americans continue to rate those in medical professions as having higher honesty and ethical standards than those in most other professions. Nurses have consistently been the top-rated profession -- although doctors and pharmacists also receive high ratings, despite the drops since 2013 in the percentage of Americans who say they have high ethics. The high ratings of medical professions this year is significant after the Ebola outbreak which infected a number of medical professionals both in the U.S. and in West Africa.
At the other end of the spectrum, in recent years, members of Congress have sunk to the same depths as car salespeople and advertising practitioners. However, in one respect, Congress is even worse, given the historically high percentages rating its members' honesty and ethics as being "low" or "very low." And although November's midterm elections did produce a significant change in membership for the new Congress that begins in January, there were also major shakeups in the 2006 and 2010 midterm elections with little improvement in the way Americans viewed the members who serve in that institution.
Previously in 2014, Gallup found that Americans continue to have low confidence in banks, and while Americans continue to have confidence in small businesses, big businesses do not earn a lot of confidence. This may be the result of Americans' views that bankers and business executives do not have high honesty and ethical standards, and the fact that their ratings dropped since last year.
Survey Methods
Results for this Gallup poll are based on telephone interviews conducted Dec. 8-11, 2014, with a random sample of 805 adults, aged 18 and older, living in all 50 U.S. states and the District of Columbia. For results based on the total sample of national adults, the margin of sampling error is ±4 percentage points at the 95% confidence level.
Each sample of national adults includes a minimum quota of 50% cellphone respondents and 50% landline respondents, with additional minimum quotas by time zone within region. Landline and cellular telephone numbers are selected using random-digit-dial methods.
I'm a proud nurse from a proud family of nurses, yet I would never claim that a layperson would enjoy watching mainstream medical dramas with us. We end up yelling at the screen: "There is nothing about that sexy get-up that remotely resembles a nursing uniform," and "Doctors don't fire nurses, nurse managers fire nurses," and "No emergency room nurse would ever have to be told by a doctor to start CPR!"
So when the Baymax, the nurse/robot in the hit Disney movie Big Hero Six turned out to be reasonable, competent and not dressed in fishnet stockings, I was thrilled.
You know your profession has an image problem when you point to a balloonish animated robot doll and say, "Yes, that's good. That accurately reflects what I do on a daily basis. More representations like that, please."
Baymax might not look like any nurses you know, but unlike most nurse characters in the media he actually provides nursing care. He assesses the health condition of his charge, the boy-genius Hiro, makes recommendations related to his health and teaches him about his neurochemical processes.
Once Hiro reprograms Baymax with fighting capabilities, Baymax becomes Hiro's terrifying defender. If you've ever heard a nurse on the phone with an insurance company insisting that a patient get needed care paid for, you know this is not a misplaced metaphor.
Contrast this with the Nurse Dawn character in the HBO comedy Getting On. She has sex with a new nurse manager within hours of meeting him; doesn't seem to notice when a patient dies; cowers submissively in front of even the most incompetent doctors and never seems to provide any actual nursing care because she is too busy with self-created drama and paperwork.
Or the Nurse Beverly character in Fox's comedy The Mindy Project. She is fired from an office medical practice for incompetence, breaks a doctor's nose in angry response, and when she is rehired in a clerical position expresses relief that she finally has a job where she doesn't have to wash her hands.
Or the nurses in the Fox medical drama House. Rather than being sexually inappropriate or incompetent, these nurses all seem to be on a series-long coffee break. It is the doctors who are shown providing nursing care: starting IVs, doing patient teaching, negotiating complicated family dynamics at the bedside.
Even when nurses are shown to be competent, compassionate patient-focused experts like Jackie Peyton, the main character in Showtime's Nurse Jackie, the creators aren't satisfied with the life-and-death drama of a high-level trauma center in a huge city. The nurse character has to be an unethical, lying, stealing, not quite-in-recovery drug addict as well.
The argument could be made that it's the job of Hollywood to create fiction of all the professions, and that popular culture gets everything about health care wrong.
Certainly examples of this exist: the new Fox teen drama Red Band Society is populated by exceedingly healthy looking, extremely attractive gravely ill teenagers who live for months in hospital rooms the size of two-bedroom apartments for no other apparent reason than to make it more convenient for them to kiss each other.
Any scenes in which the dying but randy teens are portrayed interacting with medical care (one patient is shown receiving dialysis for liver failure) are so ludicrous that it makes you wonder if the procedure for the show's writers is to ask their medical adviser how something might accurately be conveyed and then write the exact opposite.
But even though this is just entertainment, the stakes for the future of nursing are high. Research has repeatedly demonstrated that Americans believe what TV shows say about medical care and health policy.
For 13 years the non-profit advocacy organization Truth About Nursing has been researching and documenting nurse representations in popular culture and has come to the conclusion that "the vast gap between what skilled nurses really do and what the public thinks they do is a fundamental factor underlying most of the more immediate apparent causes of the [nursing] shortage [including], understaffing, poor work conditions, [and] inadequate resources for nursing research and education."
This is bad news for nurses, but worse news for patients. Nurses make the difference in good health care; increased RN staffing decreases the overall patient death rate as well as the rate of hospital acquired pneumonia, falls, pressure ulcers and blood clots after surgery. When nurses show more signs of burnout related to understaffing, postsurgical infections increase.
And there's the hard-to-quantify but essential benefit of being cared for. When I was in the hospital this past January after a life-threatening complication of knee-replacement surgery, I woke up one night in pain and unable to figure out how to move within the many drains, tubes and wires attached to, or inserted in, my body. I muttered an expletive and from around the corner a nurse appeared.
"I'm right here," she said. Even before she started to untangle my IV and troubleshoot better pain management, my panic was instantly calmed.
Baymax's programming won't allow him to disengage until the patient has answered, "Are you satisfied with your care?" in the affirmative. This is inconvenient for the characters in an action adventure movie, but it's a good question to ask in a hospital. If you're satisfied with your care, you may well have a nurse to thank.
What do all nurses want for this holiday season? We asked the nursing community on Facebook and reddit and we discovered that yes, it’s not necessarily a pair of scrubs. Here are their answers:
Better staffing and better nursing jobs
Top of the list are these answers that we think go hand-in-hand:
“A job. Going 2 months strong being unemployed (currently living the dream of being a stay at home wife). When I was working: Adequate staffing.” – mogris, from reddit
“I second the ‘adequate staffing’. I'm a little worried that my Christmas night will be crushingly busy.” – CrossP, from reddit
“I'm in the same unemployment boat as you. It is not a fun ride. I just want to be someone's nurse again.” – OkieDokieArtichokee, from reddit
“Better nurse to patient ratio!” – Lisa B., from Facebook
“Low census and adequate staffing” – nocturnalnurse, from reddit
When hospitals and other healthcare facilities don’t want to hire more nurses, then obviously there are fewer nursing jobs created. Meanwhile, the existing staff will have to bear a heavier workload.
The right to die with dignity
“Legalized euthanasia.” – Vilalintine, from reddit
After all, death shouldn’t be something to be afraid of. Controversial as this may sound, sometimes it is the better option for the patient.
The company of family and friends, at home or even at work
All nurses want for Christmas is “to spend it with their families.” – Leslie C., from Facebook
“To not be pulled to another unit. I'm already away from my home family, don't take me away from my work family too!” – FunkeeBananas, from reddit
“Word. Worst Christmas ever involved me and another nurse getting pulled to another unit, that nurse crying, my pod mate being a total bitch, and my two being patients sad, sad trainwrecks. Ugh.” – abermanlebt, from reddit
Who doesn’t want to feel at home this Christmas, even at work?
The ability to not get tired
“Feet that don't hurt after 12hrs.” –Hottiemcgee, from reddit
A break during their shift or sometimes a break from nursing itself.
“A break…” – Nancy G., from Facebook
“Nonnursey gifts. ;) seriously, get me a new game or help with the gaming PC I'm building and I will love you forever. Or blankets. My husband keeps this apartment freezing! Same there's only do many layers and blankets I can cover up in before it impedes my gaming.” – thackworth, from reddit
“Steam gift cards and a matched pair of GeForce GTX 980s. ...or is that just me?” – auraseer, from reddit
Everyone does need a break from nursing once in a while—and that break takes different forms. For some of our nurses, it’s a day of playing their favorite video games. So before you go shopping to get some gifts for nurses, you may want to consider this fact. (Hint: if your nurse friends aren’t gamers, a day of pampering is always nice.)
And of course, all nurses want the best for their patient.
“For the NICU babies to go home with their family.” – kitty-cat-meow, from reddit
“An empty waiting room.” – A_guy_in_scrubs, from reddit
No patients means no one’s sick, and hence, no problem!
We’ll end this post with a Christmas carol from rninnj, posted on reddit:
Between 1990 and 2013, global life expectancy increased by nearly 5.8 years in men and 6.6 years in women, according to a new analysis of the Global Burden of Disease Study 2013 published in The Lancet.
"The progress we are seeing against a variety of illnesses and injuries is good, even remarkable, but we can and must do even better," says lead author Dr. Christopher Murray, professor of Global Health at the University of Washington.
"The huge increase in collective action and funding given to the major infectious diseases such as diarrhea, measles, tuberculosis, HIV/AIDS and malaria has had a real impact," he says.
"However, this study shows that some major chronic diseases have been largely neglected but are rising in importance, particularly drug disorders, liver cirrhosis, diabetes and chronic kidney disease."
The analysis suggests that life expectancies in high-income regions have been increased due to falling death rates from most cancers - which are down by 15% - and cardiovascular diseases - which are down by 22%.
In low-income countries, rapidly declining death rates for diarrhea, lower respiratory tract infections and neonatal disorders have boosted life expectancy.
Despite the increases in global life expectancy by nearly 5.8 years in men and 6.6 years in women, some causes of death have seen increased rates of death since 1990.
These increased causes of death include:
Liver cancer caused by hepatitis C (up by 125%)
Atrial fibrillation and flutter (serious disorders of heart rhythm; up by 100%)
Drug use disorders (up by 63%)
Chronic kidney disease (up by 37%)
Sickle cell disorders (up by 29%)
Diabetes (up by 9%)
Pancreatic cancer (up by 7%).
HIV/AIDS has 'erased years of life expectancy' in sub-Saharan Africa
The report also points to one notable global region where life expectancy is not increasing. Deaths from HIV/AIDS have erased more than 5 years of life expectancy in sub-Saharan Africa, say the authors. HIV/AIDS remains the greatest cause of premature death in 20 of the 48 sub-Saharan countries.
Since 1990, years of life worldwide lost due to HIV/AIDS is reported as having increased by 334%.
In Syria, war is the leading cause of premature death - the conflict caused an estimated 29,947 deaths in 2013, and up to 54,903 and 21,422 deaths in each of the preceding 2 years.
Countries that the authors consider to have made "exceptional gains in life expectancy" over the past 23 years include Nepal, Rwanda, Ethiopia, Niger, Maldives, Timor-Leste and Iran - where, for both sexes, life expectancy has increased by more than 12 years.
Life expectancy at birth in India increased from 57.3 years for men and 58.2 years for women in 1990 to 64.2 years and 68.5 years, respectively, in 2013. The authors say that India has made "remarkable progress" in reducing deaths, with the death rates for children dropping 1.3% per year for adults and 3.7% per year for children.
The report also welcomes dramatic drops in child deaths worldwide over the study period. In 1990, 7.6 million children aged 1-59 months died, but this death rate was down to 3.7 million by 2013.
Igor Rudan and Kit Yee Chan, from the Centre for Population Health Sciences and Global Health Academy at the University of Edinburgh Medical School in the UK, write in a linked comment:
"Estimates of the causes of the global burden of disease, disability, and death are important because they guide investment decisions that, in turn, save lives across the world.
Although WHO's team of experts have been doing fine technical work for many years, its monopoly in this field had removed incentives to invest more time and resources in continuous improvement [...] the competition between WHO and the GBD [Global Burden of Disease Study] has benefited the entire global health community, leading to converging estimates of the global causes of death that everyone can trust."
NAHN is pleased to present the NAHN National Certification for Bilingual Healthcare Providers Medical Spanish Course & Exam in partnership with Canopy Apps, a health tech company that is improving access to information across language barriers to improve healthcare.
In line with NAHN’s dedication to the professionalism and advancement of Hispanic nurses, the NAHN Medical Spanish Certification offers access to improved provider competencies in Hispanic culture and language. Healthcare providers- both on the individual and organizational level - benefit from increased proficiency in medical Spanish, resulting in the ability to reach individuals who are unable or afraid to get assistance because of linguistic barriers. The acceptance of this credentialing in the provider community on a wide-spread basis has broad-reaching potential, including reduced risk of medication and treatment non-adherence in a growing Hispanic American population with increasing medical needs.
The NAHN Medical Spanish Course is a comprehensive, self-paced online course covering the essentials of patient-provider communication in Spanish. The medical Spanish knowledge provided in the three-level program results in a provider who can communicate with and provide appropriate care to Hispanic patients. Following the program, the NAHN Medical Spanish Certification exam assesses the ability for an individual to communicate directly with Hispanic patients in a clinical setting without the use of an interpreter. The program offers 18 Continuing Nurse Education (CNE) hours for completion of the course.
NAHN members receive a discount on both the course and the exam. When registering for the course and/or the exam, please login using the email address from which you received this email to receive your discount.
Chickenpox befell Angelina Jolie this week, preventing the actress-turned-director from attending the premiere of her new film.
Meanwhile, an outbreak of mumps has hit the National Hockey League, sidelining more than a dozen players and two referees.
These are considered kids' diseases. Most adults have vivid, fretful childhood memories of standing in line to get vaccinations that they expected to provide lifetime protection.
Why, then, are these prominent adults -- and scores of others -- coming down with these infections?
Mainly, it comes down to two factors, experts say.
Vaccination rates have declined among children in some parts of the United States, increasing everyone's risk of exposure to virulent diseases like chickenpox, measles, mumps and whooping cough, said Dr. Aaron Glatt, a spokesman for the Infectious Diseases Society of America.
"These vaccines are not perfect," said Glatt, who's also executive vice president of Mercy Medical Center in Rockville Centre, N.Y. "If you don't have a perfect vaccine and you couple that with a less-than-ideal number of people getting it, then if one person gets it then it's more likely to spread to others."
On top of that, even adults who got their shots as kids are at risk of contracting these diseases once exposed to them, because the protection provided by childhood vaccinations can fade over time.
"You can be vaccinated for something and have antibodies that wane over time or disappear entirely," said Dr. Len Horovitz, an internist and lung specialist at Lenox Hill Hospital in New York City. "You can have intermittent immunity, or no immunity."
America's public health defense against infectious diseases is built on a concept called "herd immunity," Glatt explained. If enough people are vaccinated against diseases like chickenpox, influenza, mumps and whooping cough, then even those who aren't vaccinated benefit because those who are immune can't spread the disease.
Skepticism over the effectiveness and safety of vaccines has caused vaccine rates to decline in some parts of the country, Horovitz and Glatt said. In those locations, adults with waning or imperfect immunity could fall prey to childhood infectious diseases, particularly if there's an outbreak.
"There is less vaccination going on than there was previously," Glatt said. "These childhood diseases have not gone away, and there is a strong anti-vaccine lobby that plays a role in people's decision to have their children vaccinated."
Since the early 1980s, there has been an overall increasing trend of whooping cough in the United States, said Angela Jiles, a spokeswoman for the federal Centers for Disease Control and Prevention.
Between Jan. 1 and Aug. 16 of this year, the CDC received reports of 17,325 cases of whooping cough, a 30 percent increase from the same time period in 2013 and the most cases seen in six decades, Jiles said.
California is experiencing its worst outbreak of whooping cough in seven decades.
There also have been more reported mumps cases in the United States this year, due to some larger outbreaks, according to the CDC. A reported 1,078 people have contracted mumps in 2014, compared with 438 the year before. In 2006 -- the worst year in recent history -- there were 6,584 cases of mumps, largely due to outbreaks on college campuses, according to the CDC.
No one has said how Jolie might have contracted chickenpox, but many of the NHL players appear to have gotten mumps from each other, despite efforts by the hockey league to get players vaccinated.
A single dose of mumps vaccine is about 80 percent effective, and two doses is about 90 percent effective, Amy Parker Fiebelkorn, an epidemiologist with the CDC's measles, mumps, rubella and polio team, told The New York Times.
"There is no vaccine that's 100 percent effective," Fiebelkorn said. "There is some margin for fully vaccinated individuals to still be infected with mumps if they're exposed to the virus."
Unfortunately, adults who contract these diseases are in for a rougher ride than children. They are more likely to develop serious complications, and are at higher risk of death, Glatt and Horovitz said.
These viruses also can increase a person's risk of future illness. For example, chickenpox patients like Jolie have a lifetime risk of shingles, a disease that can cause terrible rashes and intense nerve pain. The chickenpox virus hides in deep reservoirs inside the human body, and then emerges later in life to cause shingles.
Concerned adults can ask their doctor for a blood test that will check their antibodies and see if they remain immune to these infectious diseases, Horovitz said.
"It's something that could be done in the course of your annual exam. It takes no more than an extra tube or two of blood," the same as regular checks for blood sugar and cholesterol, he said. "It would be particularly important for people with chronic medical conditions or who do a lot of foreign travel where these diseases are running rampant."
People also can talk with their doctor about vaccinations that are recommended for adults. For example, the CDC recommends that adults get a booster shot every 10 years for tetanus, diphtheria and whooping cough, as well as an annual flu shot.
A paralysed woman who controlled a robotic arm using just her thoughts has taken another step towards restoring her natural movements by controlling the arm with a range of complex hand movements.
Thanks to researchers at the University of Pittsburgh, Jan Scheuermann, who has longstanding quadriplegia and has been taking part in the study for over two years, has gone from giving "high fives" to the "thumbs-up" after increasing the manoeuvrability of the robotic arm from seven dimensions (7D) to 10 dimensions (10D).
The extra dimensions come from four hand movements--finger abduction, a scoop, thumb extension and a pinch--and have enabled Jan to pick up, grasp and move a range of objects much more precisely than with the previous 7D control.
It is hoped that these latest results, which have been published today, 17 December, in IOP Publishing's Journal of Neural Engineering, can build on previous demonstrations and eventually allow robotic arms to restore natural arm and hand movements in people with upper limb paralysis.
Jan Scheuermann, 55, from Pittsburgh, PA had been paralysed from the neck down since 2003 due to a neurodegenerative condition. After her eligibility for a research study was confirmed in 2012, Jan underwent surgery to be fitted with two quarter-inch electrode grids, each fitted with 96 tiny contact points, in the regions of Jan's brain that were responsible for right arm and hand movements.
After the electrode grids in Jan's brain were connected to a computer, creating a brain-machine interface (BMI), the 96 individual contact points picked up pulses of electricity that were fired between the neurons in Jan's brain.
Computer algorithms were used to decode these firing signals and identify the patterns associated with a particular arm movement, such as raising the arm or turning the wrist.
By simply thinking of controlling her arm movements, Jan was then able to make the robotic arm reach out to objects, as well as move it in a number of directions and flex and rotate the wrist. It also enabled Jan to "high five" the researchers and feed herself dark chocolate.
Two years on from the initial results, the researchers at the University of Pittsburgh have now shown that Jan can successfully manoeuvre the robotic arm in a further four dimensions through a number of hand movements, allowing for more detailed interaction with objects.
The researchers used a virtual reality computer program to calibrate Jan's control over the robotic arm, and discovered that it is crucial to include virtual objects in this training period in order to allow reliable, real-time interaction with objects.
Co-author of the study Dr Jennifer Collinger said: "10D control allowed Jan to interact with objects in different ways, just as people use their hands to pick up objects depending on their shapes and what they intend to do with them. We hope to repeat this level of control with additional participants and to make the system more robust, so that people who might benefit from it will one day be able to use brain-machine interfaces in daily life.
"We also plan to study whether the incorporation of sensory feedback, such as the touch and feel of an object, can improve neuroprosthetic control."
Commenting on the latest results, Jan Scheuermann said: ""This has been a fantastic, thrilling, wild ride, and I am so glad I've done this."
"This study has enriched my life, given me new friends and co-workers, helped me contribute to research and taken my breath away. For the rest of my life, I will thank God every day for getting to be part of this team."
At birth, a newborn baby is still attached to its mother through the umbilical cord, which is either cut very early - within the first 60 seconds - or later, with some women opting to wait until after the cord has stopped pulsating. Though the right timing for cutting the cord - also referred to as clamping - is widely debated, a new study suggests delaying cord clamping by 2 minutes results in better development for the newborn during the first days of life.
The research, carried out by scientists from the University of Granada and the San Cecilio Clinical Hospital in Spain, is published in the journal Pediatrics, the official journal of the American Academy of Pediatrics (AAP).
According to the American Congress of Obstetricians and Gynecologists (ACOG), the reason that cord clamping timing is so controversial is that a previous series of studies into blood volume changes after birth concluded that in healthy term infants, more than 90% of blood volume was attained within the first few breaths he or she took after birth.
As a result of these findings, as well as a lack of other recommendations regarding optimal timing, the amount of time between birth and umbilical cord clamping was widely shortened; in most cases, cord clamping occurs within 15-20 seconds after birth.
However, before these studies, in the mid-1950s, cord clamping within 1 minute of birth was defined as "early clamping," and "late clamping" was defined as more than 5 minutes after birth. And the ACOG have stated that "the ideal timing for umbilical cord clamping has yet to be established."
Meanwhile, the World Health Organization (WHO) advocate for late cord clamping (between 1-3 minutes after birth), as it "allows blood flow between the placenta and neonate to continue, which may improve iron status in the infant for up to 6 months after birth."
Waiting 2 minutes increased antioxidant capacity
To provide further evidence in the debate of early versus late cord clamping, the researchers from this latest study, led by Prof. Julio José Ochoa Herrera of the University of Granada, assessed newborn outcomes for infants born to 64 healthy pregnant women to determine the impact of clamping timing on oxidative stress and the inflammatory signal produced during delivery.
All of these women had a normal pregnancy and spontaneous vaginal delivery. However, half of the women's newborns had their umbilical cord cut 10 seconds after delivery and half had it cut after 2 minutes.
Results revealed beneficial effects of late cord clamping; there was an increase in antioxidant capacity and moderation of inflammatory effects in the newborns.
Commenting further, Prof. Ochoa says:
"Our study demonstrates that late clamping of the umbilical cord has a beneficial effect upon the antioxidant capacity and reduces the inflammatory signal induced during labor, which could improve the development of the newborn during his or her first days of life."
He adds that umbilical cord clamping is one of the most frequent surgical interventions practiced in humans, with proof of the practice dating back centuries.
Early clamping 'not advised unless newborn needs resuscitation'
With evidence of benefits for delayed cord clamping, however, why are most newborns separated from the placenta within 15-20 seconds after birth? According to the ACOG, there are concerns over universally adopting delayed clamping because it could "jeopardize timely resuscitation efforts, if needed, especially in preterm infants."
"However," the organization states, "because the placenta continues to perform gas exchange after delivery, sick and preterm infants are likely to benefit most from additional blood volume derived from a delay in umbilical cord clamping."
There are also other concerns regarding delayed cord clamping, including an increased potential for "excessive placental transfusion, which can lead to neonatal polycythemia" - an abnormally high level of red blood cells. This is especially of concern in the presence of risk factors including maternal diabetes, intrauterine grown restriction and high altitude.
Another concern stated by the ACOG is that delayed umbilical cord clamping "may be technically difficult in some circumstances."
Still, the WHO say late cord clamping is recommended for all births, and the improved iron status associated with it "may be particularly relevant for infants living in low-resource settings with reduced access to iron-rich foods."
The organization clearly states that early cord clamping - less than 1 minute after birth - is not advised unless the newborn is asphyxiated and needs to be moved for resuscitation.
What does a 9-year-old want after being struck by lightning and forced to spend three months in the hospital? He wants to cuddle his dog and set up his family's Christmas tree.
"He made me do it the first day I was home on Friday," the boy's father, Roger Hermann, told ABC News. "He can't move his legs, but he was directing some of the ornament placement."
Alex Hermann was on a soccer field in Austin, Texas, on Aug. 26, when a bolt of lightning struck him and stopped his heart. He suffered burn wounds and hypoxia, which is when the brain can't get enough oxygen.
Over the next three months, Alex underwent skin-grafting and wound-closure surgeries, as well as cardiac ablation, which corrects heart arrhythmias, at Dell Children's Medical Center of Central Texas. He still has a "number of issues" to address over time, but he's improving.
Although the hospital staff was great, Hermann said, Alex became homesick. Hermann added that he and Alex's mother promised that if he worked hard in therapy, they would try to get him home for Christmas.
Alex was also reunited with his beloved dog, a Catahoula Australian shepherd named Spice, who seemed pleased to have her buddy back.
"She sleeps on the bed with him," Hermann said. "She’s been guarding him."
Its name means "bending over in pain." It has no treatment or vaccine. Its symptoms resemble Dengue fever. And it has infected more than 1 million people -- 155 of them fatally -- since spreading to the Americas one year ago.
The mosquito-borne Chikungunya virus has long been diagnosed in travelers returning from countries in Asia and Africa, where the disease is widespread. But in December 2013, the first people infected by mosquitoes local to the region were reported on the Caribbean island of Saint Martin.
This was the first outbreak of the debilitating disease in the Western hemisphere, health officials said.
All countries in Central America have now reported local transmission of Chikungunya [pronounced chik-un-GOON-ya], and the United States had 11 confirmed cases of local infection this year as of December 12, all in the state of Florida. There also have been 1,900 imported cases across the U.S. in returning travelers.
"It wasn't until 2013 that unfortunately a traveler resulted in local transmission of Chikungunya," said Erin Staples of the U.S. Centers for Disease Control (CDC), referring to the people infected in Saint Martin.
Those infected carry the virus in their bloodstream; it can then be picked up by mosquitoes as they bite, making them carriers. The virus has since spread rapidly and shows no signs of leaving, as ecological conditions are perfect for the disease to flourish.
"We knew it would spread," said Staples, a medical epidemiologist.
The big question perplexing officials: Why now?
Two mosquito species primed to the temperatures of Central and South America carry Chikungunya. The species -- Aedes aegypti and Aedes albopictus -- also carry the virus behind Dengue fever.
"Given the level of Dengue in the region, we knew there could be the same levels of Chikungunya," Staples said. Both diseases can cause joint pain and inflammation, headaches, rashes and fever, and can lead to death in rare cases.
But this tropical disease with an exotic name (which originates from the African Makonde dialect) causes more intense joint pain and inflammation. For some people the pain can last for months or years, resulting in additional psychological strain.
The lack of immunity among people living in the Americas provided a blank canvas for Chikungunya to spread throughout the population this year. As of December 12, more than 1.03 million people have been infected, in addition to the 155 who died, according to the Pan-American Health Organisation (PAHO). Almost all of the fatalities occurred in the Caribbean island countries of Guadaloupe and Martinique.
"Where we saw the biggest jump was after it reached the Spanish-speaking countries in the region," said Staples, referring to the weakened infrastructures and health systems of countries such as the Dominican Republic, which has reported more than 520,000 cases -- more than half of the overall outbreak and 5% of the island country's population.
As South American countries approach their summer, numbers are expected to rise there as the mosquitoes flourish in the heat.
"Brazil, Peru, Paraguay are coming into their summer months and reporting their first local transmission," Staples said. Already, more than 2,000 people have been infected in Brazil.
Is there cause for concern?
Because infection with Chikungunya is rarely fatal, the issue of most concern to officials is the burden on health services and the impact of the debilitating symptoms on the economy.
"The high number of cases can overload health services," says Dr. Pilar Ramon-Pardo, regional adviser for PAHO, the regional office of the World Health Organization. Until recently, monitoring for Chikungunya was not part of routine surveillance in the region.
"Clinicians have to be ready to diagnose," she said
About 20% to 30% of cases are expected to become chronic, with symptoms such as arthritis and other rheumatic manifestations leading to physical disabilities, Ramon-Pardo said. Further long-term effects are psychological as people become more depressed and tired.
All of this can result in missed work and lower school attendance, she said, hurting local economies.
Is it here to stay?
The warm climate of the region offers potential for Chikungunya levels to be maintained for years to come, just like Dengue fever. But areas of most concern are the tropics.
"The areas which have year-round favorable climate for the mosquito are at the greatest risk," says Dr. Laith Yakob of the London School of Hygiene and Tropical Medicine, which is monitoring the spread of the outbreak.
While the climate and mosquitos have long been present, Ramon-Pardo said, "we don't know why this is happening now." She said globalization is likely to blame, with increased population movement from one country to another. This offers more opportunities for local mosquitos to bite infected humans.
The CDC's Staples said she is temporarily at ease regarding numbers in the U.S. "We're moving into fall and winter periods, which should see activity decrease," she said. Cold temperatures reduce mosquito survival rates.
The rapid spread of Chikungunya this year also could help minimize future infections. "Chikungunya will go through a region quite rapidly and create a level of population immunity which helps mitigate large outbreaks of the disease," Staples said. Unlike Dengue, infection with Chikungunya results in lifelong immunity.
Like many other infections, Chikungunya could, however, remain in the background through animals capable of carrying the virus in their bloodstream and acting as so-called reservoirs of the disease.
"In Asia and Africa there is a transmission cycle in small mammals and monkeys," Ramon-Pardo said, meaning these animals keep the virus present within the population. "In the Americas ... we don't know yet."
Those words -- "we don't know" -- resonate throughout the community of scientists and government officials trying to control the outbreak.
The future risk of spread, levels of future immunity, risk from animal reservoirs, why this is only happening now, and the total economic impact are all unknown.
"Mathematical models are under construction by numerous research groups around the world to improve confidence over projections of future spread," said Yakob, whose team is modeling the disease. As they work, control efforts continue.
Getting it under control
When it comes to controlling Chikungunya, there are two main strategies -- reduce the likelihood of bites and remove the ever-biting mosquito. Prevention is the priority.
Unlike the mosquitoes behind malaria, which bite at night, the species behind Chikungunya bite any time, day or night. Those living in affected areas are asked to use repellent, sleep under bed nets and wear long clothing to avoid getting bitten. The air conditioned and indoor environments of people living in the U.S. mean numbers are likely to stay low there.
But mosquito control is at the heart of it all. Mass spraying of insecticides and removal of any sources of shallow water in which mosquitoes can breed are taking place across the continents. According to the CDC's Staples, Florida has been highly aggressive with its approach to control. "We're only at 11 (cases) due to such proactive measures," Staples said. For now, prevention is all they have as officials wait and see how the outbreak pans out.
"There is no vaccine currently and no good antivirals, so we are trying to control the spread of the disease," Staples said. "There are a lot of questions and only time will tell what we'll see for Chikungunya in the future."
When 2-year-old Ryan Aprea had cochlear implant surgery in November, his mom, Jennifer, says she wasn’t sure what to expect when the device was activated a month later.
Aprea shared the moment last week in a video that has now gone viral. In the clip, the Huntington Beach, California, mom says, “Hi, Buddy,” to her son, and is rewarded with a reaction she calls “amazing” — a fit of giggles from her little boy.
Born as a micro preemie at only 25 weeks gestation, Aprea says Ryan began his life with a seven-month stay in the neonatal intensive care unit, where she and her husband learned that he was deaf shortly before his discharge.
But a cochlear implant offered hope.
“We went into the appointment not knowing if he would respond at all. Throughout this process, they had informed us that while sound would enter his brain, every child has a different response. We weren’t sure if his brain would process the sound, but we wanted to give him a chance to hear us and communicate because he is also visually impaired,” said Aprea.
Aprea, who has posted frequently about the cochlear implant process on the Facebook page of her cloth diaper supply company, tells TODAY Parents that since the activation, Ryan has been doing great — exploring toys that make sounds for the first time and taking in his surroundings with his newfound ability to hear.
“He’s been interacting with us and giving us more intentional eye contact just in the few days since he’s had it turned on. My heart melts every single time he looks at me,” said Aprea.
As for future plans for Ryan’s treatment, Aprea says she and her family are taking things one day at a time. The mother of two says she’s looking forward to taking her son for a drive to look at holiday lights while listening to Christmas music — a tradition her family shares every year, but one that will have new meaning this season.
Aprea says she is shocked that her video has gone viral, adding that she looks forward to seeing more people learn about cochlear implants as videos and articles about stories like Ryan’s become more prevalent.
She’s heard a lot of strong opinions about cochlear implants from online commenters — including some negative ones — and offers some advice to parents dealing with big decisions about their child’s health care.
“You know your child better than anyone — I learned that one in the NICU. You need to do what’s best for him or her and give them every opportunity available to succeed in life. I would say, do a lot of research, talk to people who have been through it with their own kids, and then go with your heart,” she said.
This little girl received a boost of confidence from a Disney princess that made her feel like she was in a fairy tale.
Isabella Harvey, 5, of Staten Island, New York, was first diagnosed with leukemia in January 2013, and while she went into remission for over a year, she relapsed this September and needed aggressive chemotherapy. The 5-year-old's hair began falling out, making her upset at her appearance.
"She was embarrassed," Isabella's mother, Pina told The Huffington Post in an email. "When her hair fell out the first time she was 3 so she really didn't understand. But now she is 5 and was having a hard time dealing with it."
In an effort to get Isabella to see herself in a more positive light, Pina reached out to Gianna Nicole’s Heart of Hope, an organization which helps families whose children are battling cancer. The charity teamed up with Bella Princess LLC, a princess party company to set up a photo shoot late last month for Isabella -- complete with special guest, Cinderella. The model who dressed as the Disney princess donned a bald cap, and showed the young cancer patient that she had nothing to be insecure about.
"After all she went through ... it was such an amazing feeling seeing her so happy," Pina told HuffPost.
Before finding out that Cinderella would be attending her special day, Isabella, who was accompanied by her siblings, was hesitant to participate in the photo shoot, uncomfortable with showing her head.
"At first she didn't want to go. Then, she said she would go with a hat on, and when we got there she still refused to take off her hat," Pina said about of her daughter's uneasiness.
It all changed, however, when Cinderella walked in, confident even without hair.
"She said, "she looks just like me!'" Alana Hubbard, the photographer behind Mother Hubbard Photography who shot the images, told HuffPost.
Pina added, "Her face lit up and seemed to relax a little. Isabella took off her hat. She was so happy and seemed more at ease taking pictures."
The photo shoot ended up having quite an effect on the 5-year-old, who recently saw the pictures for the first time.
"It re-enforces what I tell her every day -- that she is beautiful. That photo shoot just made her realize everyone feels the same way as [I do]," Pina told HuffPost.
Hubbard says she's ecstatic to hear about Isabella's newfound confidence, and hopes that the pictures will provide others going through the same thing with some comfort.
"We're really hoping that it shows other little girls who may be going through cancer too, that you can be a perfect princess with or without hair," Hubbard said.
It started with a sore throat on Thanksgiving and an antibiotic from a friend who wanted to help.
Now 19-year-old Yaasmeen Castanada is fighting for her life inside a California hospital's burn unit, suffering from an allergic reaction that's so severe she has large open wounds all over her body.
"It is heartbreaking, every day is a different look. Every day, she's like, shedding away. ... Overnight, it's a whole different person that you're looking at," Martha Hughes, Castanada's aunt, told CNN affiliate KABC.
Doctors diagnosed Castanada with Stevens-Johnson Syndrome, a rare disease that can be triggered by antibiotics or other medications.
"When she took the medication, she started having a hard time breathing, and she told her mom that her lips were burning, her throat, her eyes, they got so red that she couldn't talk. So she rushed her to the ER, and that's when they diagnosed her with the disease. And from there it has just spiraled to a nightmare," Hughes said.
Now Castanada, the mother of a 4-month-old, is in critical condition at the University of California, Irvine, burn center.
Her prognosis is good, even though the disease has a high mortality rate, according to Dr. Victor Joe, the center's director.
But the situation, Castanada's family says, has been devastating.
"Just unreal, just watching your daughter burn in front of you, literally, burn in front of you," her mother, Laura Corona, told KABC. "Every day, a new blister, a new burn, a new scar. And she's just, 'Mommy, I want to go home.' And I can't take her home. I can't put water on her lips."
Mom: 'Don't share medication'
On a website created to raise funds for Castanada's care, her mother said the harrowing ordeal began soon after her daughter took the medicine.
"A friend offered her an antibiotic pill that she had from a previous illness," Corona wrote. "She was thinking that it would help her. This would be the biggest mistake of her life."
Now, Corona says she's hoping to spread the word so others don't make the same mistake.
"Don't share medication. Don't give someone else your medication. Don't offer medication," she said.
She also advises parents to find out what their children are allergic to -- before it's too late.
Doctor: Reaction causing skin to separate
At first, doctors diagnosed Castanada with Stevens-Johnson Syndrome, which refers to a condition where between 10% and 30% of the skin on the body is affected, Joe said. Now she's experiencing Toxic Epidermal Necrolysis, the diagnosis when more than 30% of the body is affected. Joe estimates that 65% of Castaneda's skin and mucus membranes have been affected.
The allergic reaction is causing layers of Castaneda's skin to separate, Joe said, creating lesions that grow into large open wounds.
"Patients can experience problems with taste, swallowing, eyesight and sexual functions can be affected. In Yaasmeen's case, we are particularly concerned because her eyes have been affected. This can cause scarring of the corneas, which could lead to permanent blindness," he said. "We are trying to prevent that from happening."
Photos on the fundraising website show Castanada lying in a hospital bed, with openings for her eyes cut from the bandages that cover her.
As part of her treatment for the disease, doctors have wrapped her body in a special dressing, Joe said.
"We have chosen to place a dressing that adheres to the open wound, which allows her skin to heal without having to remove the bandages to wash the wounds," he said.
Mortality for those suffering from Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis can be as high as 25% in adults, but tends to be lower with early treatment, according to the Merck Manual.
Though it's uncommon, Joe said his hospital has treated around six cases in the past year, because the burn center has experience treating open wounds.
"This is very sobering. The fact that you can get a life-threatening situation from taking a medication. It can happen, and most people don't think twice about taking pills for things," Joe said. "In fact, most of the time you do have some sort of side reaction to medication, just not this severe."
After recovering from Stevens-Johnson Syndrome, patients usually only have minor issues with their skin, such as dryness, Joe said.
"Hopefully new skin will come in," Corona told KABC. "I'm just there watching. All I can tell her is, "Hang on, hang on. It's almost over.'"
A young Liberian woman who saved three of her relatives by nursing them back to health after they contracted the Ebola virus is coming to the United States to finish her nursing degree.
The news comes as Time magazine announced Wednesday that its "Person of the Year" honors go to the Ebola fighters, the "unprecedented numbers" of doctors and nurses who responded when Ebola overtook an already-weak public health infrastructure this year in West Africa.
Fatu Kekula is not named in the article, but she definitely holds a place among those being honored.
The 22-year-old, who was in her final year of nursing school earlier this year, single-handedly took care of her father, mother, sister and cousin when they became ill with Ebola beginning in July.
And she did so with remarkable success. Three out of her four patients survived. That's a 25% death rate -- considerably better than the estimated Ebola death rate of 70%.
Kekula stayed healthy, which is noteworthy considering that hundreds of health care workers have become infected with Ebola, and she didn't even have personal protection equipment -- those white space suits and goggles used in Ebola treatment units.
Instead, Kekula invented her own equipment. International aid workers heard about her "trash bag method" and taught it to other West Africans who can't get into hospitals and don't have protective gear of their own.
Every day, several times a day for about two weeks, Kekula put trash bags over her socks and tied them in a knot over her calves. Then she put on a pair of rubber boots and then another set of trash bags over the boots.
She wrapped her hair in a pair of stockings and over that a trash bag. Next she donned a raincoat and four pairs of gloves on each hand, followed by a mask.
It was an arduous and time-consuming process, but she was religious about it, never cutting corners.
UNICEF Spokeswoman Sarah Crowe said Kekula is amazing.
"Essentially this is a tale of how communities are doing things for themselves," Crowe said. "Our approach is to listen and work with communities and help them do the best they can with what they have."
She emphasized, of course, that it would be better for patients to be in real hospitals with doctors and nurses in protective gear -- it's just that those things aren't available to many West Africans.
No one knows that better than Kekula.
Her Ebola nightmare started July 27, when her father, Moses, had a spike in blood pressure. She took him to a hospital in their home city of Kakata.
A bed was free because a patient had just passed away. What no one realized at the time was that the patient had died of Ebola.
Moses, 52, developed a fever, vomiting and diarrhea. Then the hospital closed down because nurses started dying of Ebola.
Kekula took her father to Monrovia, the capital city, about a 90-minute drive via difficult roads. Three hospitals turned him away because they were full.
She took him back to another hospital in Kakata. They said he had typhoid fever and did little for him, so Kekula took him home, where he infected three other family members: Kekula's mother, Victoria, 57; Kekula's sister, Vivian, 28, and their 14-year-old cousin who was living with them, Alfred Winnie.
While operating her one-woman Ebola hospital for two weeks, Kekula consulted with their family doctor, who would talk to her on the phone, but wouldn't come to the house. She gave them medicines she obtained from the local clinic and fluids through intravenous lines that she started.
At times, her patients' blood pressure plummeted so low she feared they would die.
"I cried many times," she said. "I said 'God, you want to tell me I'm going to lose my entire family?' "
But her father, mother, and sister rallied and were well on their way to recovery when space became available at JFK Medical Center on August 17. Alfred never recovered, though, and passed away at the hospital the next day.
"I'm very, very proud," Kekula's father said. "She saved my life through the almighty God."
Her father immediately began working to find a scholarship for Kekula, so she could finish her final year of nursing school. But the Ebola epidemic shut down many of Liberia's schools, including hers.
After a story about Kekula ran on CNN in September, many people wanted to help her.
A non-profit group called iamprojects.org also got involved.
With some help, Kekula applied to Emory University in Atlanta, the campus with the hospital that has successfully cared for American Ebola patients. Emory accepted the young woman so that she could complete her nursing degree starting this winter semester.
In order to attend, iamprojects will have to raise $40,000 to pay for her reduced tuition rate, living expenses, books and her travel and visa so that she can travel between Africa and the United States.
Kekula's father has no doubt that his daughter will go on to save many more people during her lifetime.
"I'm sure she'll be a great giant of Liberia," he said.
Not all children with severe brain injuries need to be monitored for subclinical seizures, researchers said here, which means that resources can be focused on those at the highest risk.
Victims of abuse, those younger than 2, and those with bleeding within the brain rather than only in the epidural compartment are the pediatric ICU patients most likely to show significant seizure activity that should be detected and treated, said Rajsekar Rajaraman, MD, of the University of California Los Angeles (UCLA).
A separate study by many of the same investigators also found that, in a broader range of pediatric brain injury cases, risk of seizures could be predicted with "fair-to-good" accuracy on the basis of clinical characteristics that would be recorded routinely at admission.
Both studies were reported at the American Epilepsy Society's annual meeting here.
A senior author on both studies, Nicholas Abend, MD, of Children's Hospital of Philadelphia, said at an AES press briefing that identifying and treating seizures is important in the pediatric ICU. When seizures are extremely frequent or long-lasting -- and these can easily go without detection in hospitalized children who are unconscious or lethargic -- they significantly increase the likelihood of poor short- and long-term outcomes.
Such seizures can only be detected via continuous EEG monitoring, Abend explained, which also requires interpretation from trained electroneurologists.
Another investigator in the studies, UCLA's Jason Lerner, MD, noted that children may appear to be napping peacefully while actually undergoing continuous seizures.
Although it would be desirable to perform intense monitoring on all pediatric cases involving head trauma, that is not feasible at most centers, Abend said. He said the field could benefit from risk-stratification models that would allow the care team to track only those patients at the highest risk for damaging subclinical seizures.
Such models, he added, could be tailored to meet the needs of individual centers on the basis of their patient mix, staffing, and other factors.
In a platform session at AES, Rajaraman described one approach to developing such a model. He and colleagues collected data on 135 consecutive pediatric patients (ranging in age from infant to late adolescent) with traumatic brain injury who were treated in ICUs at UCLA and at Children's Hospital of Colorado in Denver. These children had continuous EEG monitoring for detecting subclinical seizures.
They found that all such seizures occurred in children younger than 2 and in those with intradural bleeding, and that the vast majority also involved abusive head trauma. Rajaraman and colleagues then sought to validate these associations in a separate cohort of 44 pediatric ICU patients with head injuries treated at Children's Hospital of Philadelphia. The same patterns were seen.
Across both cohorts, 81% of those with subclinical seizures were determined to have been victims of abusive head trauma, whereas the prevalence of such trauma in all the patients was 25%. Abend said it was uncertain why abusive trauma should be such a strong predictor of these seizures, but speculated that "shaken baby syndrome" -- the most common form of abuse of infants and toddlers -- may produce fundamentally different injuries in the brain compared with falls and car accidents.
Also, such abuse is often chronic, such that the episode that brings a child to the hospital is only the latest in a series of abusive incidents.
The other study, led by Abend, was aimed at producing a predictive model yielding a risk index score that pediatric centers could use to identify critically ill children who could benefit the most from continuous EEG monitoring. It was based on clinical information to which the attending neurologist would have ready access: age, seizure etiology, presence of clinical seizures prior to beginning continuous EEG, initial EEG background category, and interictal discharge category.
Data to design the model were drawn from a database of 336 patients from 11 centers, and then tested against a separate validation dataset of 222 patients treated at Children's Hospital of Philadelphia.
Normalized scores in the model could range from 0 to 1.0, and Abend and colleagues examined the sensitivity and specificity of various cutoffs. When set at 0.10 in the validation cohort, sensitivity was 86% but sensitivity was only 58% -- the high sensitivity meant that 43% of patients would be identified as candidates for continuous monitoring. At the other end, a cutoff of 0.45 reversed the sensitivity and specificity percentages to 19% and 97%, respectively, such that only 5% of patients would be assigned to monitoring.
Abend said the beauty of this approach is that an individual center could choose its own optimal cutoff depending on the resources it has available to monitor multiple patients at one time. A well-equipped and staffed ICU could thus opt for high sensitivity whereas one with more limited resources could be more restrictive.
Jessica Zegre-Hemsey, a cardiac monitoring expert at the University of North Carolina at Chapel Hill, and her colleagues at the University of California San Francisco, revealed more than 2.5 million alarms were triggered on bedside monitors in a single month - the first figure ever reported from a real-world hospital setting.
Alarm fatigue occurs when nurses and other clinicians are exposed to a high number of physiological alarms generated by modern monitoring systems. In turn, alarms are ignored and critical alarms are missed because many alarms are false or non-actionable.
The work, the first of its kind to investigate the frequency and accuracy of alarms, addresses a growing patient safety issue that has gained national attention in recent years when a patient died despite multiple alarms that indicated low heart rate. The issue also addresses hidden downsides to modern monitoring technologies.
"Current technologies have been instrumental in saving lives but they can be improved," said Zègre-Hemsey, who is an assistant professor at the UNC-Chapel Hill School of Nursing. "For example, current monitoring systems do not take into account differences among patients. If alarm settings were tailored more specifically to individuals that could go a long way in reducing the number of alarms health care providers respond to."
Zègre-Hemsey and her colleagues collected alarm data on 461 adults in five intensive care units at the UCSF Medical Center for a period of 31 days. Zègre-Hemsey was one of four scientists who analyzed the alarms and helped to determine if they were true or false.
Investigators analyzed a subset of 12,671 arrhythmia alarms, which are designed to alert providers to abnormal cardiac conditions, and found 88.8 percent were false positives. Most of the false alarms were caused by deficiencies in the computer's algorithms, inappropriate user settings, technical malfunctions, and non-actionable events, such as brief spikes in heart rate, that don't require treatment.
A potential solution the researchers suggested would be to design monitors that could be configured to individual patients. No two bodies are exactly the same, and if the monitors could be adjusted to a patient's unique vital signs, the machines would not mistake a normal condition for an abnormal one. A "gold standard" database of annotated alarms could also help developers create computer algorithms that are less sensitive to artifacts.
According to Zègre-Hemsey, reducing alarm fatigue will ultimately require strong collaborations between clinicians, engineers, and hospital administrators as well as additional research.
"Alarm fatigue is a large and complex problem," she said. "Yet the implications are far-reaching since sentinel events like patient death have been reported. This is a current patient safety crisis."
The study was led by primary investigator Barbara J. Drew at UCSF. Co-authors on the paper include UCSF researchers Patricia Harris, Daniel Schindler, Rebeca Salas-Boni, Yong Bai, Adelita Tinoco, Quan Ding, and Xiao Hu from the UCSF department of physiological nursing and Tina Mammone from the UCSF department of nursing.
Brittany Wenger is one seriously smart cookie. In 2012, the then-17-year-old submitted her "artificial brain" technology -- which assesses tissue samples for breast cancer -- to the Google Science Fair and walked away with the grand prize. It was no wonder: Her invention, which uses a type of computer program called neural networks, can identify complex data patterns and make breast cancer detection calls with 99 percent accuracy. But she's not stopping there: Brittany hopes to help wipe out cancer completely.
Since she took home the gold two years ago, she's been named one of Time's 30 Under 30, given a truly inspiring TED Talk, and launched her app, Cloud4Cancer, which allows doctors to enter their own data and fuel continued cancer research. And did we mention she's also holding down a full course load at Duke University? Um, yeah.
We recently chatted with Brittany about how she got started, her challenges along the way, and how she balances being a college student with breaking the barriers of cancer diagnostics.
How did you get into computer programming?
When I was in 7th grade I took an elective class on futuristic thinking. When we were assigned our final paper, I decided to write mine on technology of the future. The moment I started researching artificial intelligence and its transcendence into human knowledge, I was inspired. I went out and bought a coding textbook, and taught myself how to code. I remember one of the first projects that I ever worked on was an artificial neural network that taught people how to play soccer.
You're a self-taught coder who went on to create a potentially game-changing cancer detection tool. How did that happen?
Well, it definitely didn't happen overnight. I spent over five years working with neural networks, starting with an entire year of research to try and recognize patterns and connect breast cancer to artificial intelligence. I faced a lot of roadblocks along the way, as this was a very complicated program with no predefined solution. I went through thousands of pages of coding and data that was available through public domains, and performed over 7.6 million test trials. I two failed projects before finally succeeding on my third attempt, taking what didn't work the first few times to optimize the code that helped build the Cloud4Cancer app.
Why did you decide on developing breast cancer detection technology?
When I was 15, my cousin was diagnosed with breast cancer. I have a very close-knit family, so seeing the impact that the disease can have on a woman and her family, firsthand, was so real to me. When I learned that one in eight women will be diagnosed with breast cancer in their lifetime, I knew that I wanted to get involved in making the process better for patients. Now, the coding that I first used to help detect breast cancer has been extended into diagnosing other types of cancers, including blood-based diseases like leukemia.
What's been the most rewarding part of the process?
The people. I've already had the opportunity to work with real patients and breast cancer survivors, as well as talk with kids who are interested in doing research or coding in the future. Knowing that my cloud application has the potential to save lives and expedite the process of discovery is so rewarding. I still get chills thinking about how, a couple of years down the line, my research can actually contribute to finding the cure for cancer.
You've got a lot on your plate these days, between Cloud4Cancer and school. How do you balance everything?
The great thing about where I am with school right now is that my schedule is entirely what I make it. I can attend classes during the week and then travel over some weekends. School is not something that I will ever bend on, as I'm actually going for my MD, PhD in pediatric oncology. At the same time, my initiative is so important to me, I don't want either one to ever outweigh the other. Luckily, I think they complement each other well and what I'm learning in my classes helps me improve Cloud4Cancer.
What's one thing you want other young women to know if they're thinking about going the tech route?
If you're interested, go for it! There have never been so many available resources or opportunities -- for women, and for society as a whole -- to pursue a career in the field. I love how technology allows you to make new things by putting together the little pieces and working towards something bigger that can really benefit the world. There's no greater feeling than solving a problem and seeing your code come to life.
A Colorado family welcomed a larger-than-expected bundle of joy when their newborn daughter was born weighing almost 14 pounds.
Mia Yasmin Hernandez tipped the scales at 13 pounds, 13 ounces after her delivery Monday at San Luis Valley Hospital in Alamosa, Colorado. The newborn’s father, Francisco Garcia, said doctors had estimated the baby would weigh 8 pounds at birth.
Mia didn't seem especially large when she was born, Gracia said.
“She was swollen and everything” after delivery, he said. “I thought she was going to [weigh] 10 or 11 pounds.”
But after weighing Mia, the nurse told Garcia the infant’s weight.
“I was like, ‘Whoa, she’s the biggest baby I’ve ever seen,’” Garcia told ABC News.
Even hospital personnel agreed. Garcia said the nurse told hi she’d never seen “a baby that big.”
Dr. Robert Barbieri, chief of obstetrics and gynecology at Brigham and Women’s Hospital in Boston, said in a previous interview about one out of 1,000 babies could weigh 11 pounds, and one out of every 100,000 could weigh 14 pounds. A 14-pound baby, he said, is extremely rare, because usually a doctor will induce labor if a baby appears oversize.
While Mia’s delivery via Caesarean section went smoothly, the infant developed breathing problems and was eventually moved to Children’s Hospital of Colorado in Aurora, Colorado, according to Garcia.
Garcia said Mia is on oxygen and doing well, although they’re not sure when she will get home.
Garcia said the couple has another four daughters at home, which might come in handy for new baby clothes.
“We bought her a lot of stuff like a newborn cap and pampers,” Garcia said. “They don't fit her. She’s too big.”
Already-strong public support for right-to-die legislation has grown even stronger in the days since the planned death of 29-year-old brain cancer patient Brittany Maynard, a new HealthDay/Harris Poll has found.
An overwhelming 74 percent of American adults now believe that terminally ill patients who are in great pain should have the right to end their lives, the poll found. Only 14 percent were opposed.
Broad majorities also favor physician-assisted suicide and physician-administered euthanasia.
Only three states -- Oregon, Washington and Vermont -- currently have right-to-die laws that allow physician-assisted suicide.
"Public opinion on these issues seems to be far ahead of political leadership and legislative actions," said Humphrey Taylor, chairman of The Harris Poll. "Only a few states have legalized physician-assisted suicide and none have legalized physician-administered euthanasia."
People responded to the poll in the weeks after Maynard took medication to end her life in early November.
Maynard moved from California to Oregon following her diagnosis with late-stage brain cancer so she could take advantage of the state's "Death With Dignity Act." Her story went viral online, with a video explaining her choice garnering nearly 11.5 million views on YouTube.
A "poster child for the movement," Maynard helped spark conversations that allowed people to put themselves in her shoes, said Frank Kavanaugh, a board member of the Final Exit Network, a right-to-die advocacy group.
"I think it is just a natural evolution over a period of time," Kavanaugh said of the HealthDay/Harris Poll results. "There was a time when people didn't talk about suicide. These days, each time conversations occur, people think it through for themselves, and more and more are saying, 'That's a reasonable thing to me.'"
The poll also found that:
Support for a person's right to die has increased to 74 percent, up from 70 percent in 2011. Those opposed decreased to 14 percent from 17 percent during the same period.
Physician-assisted suicide also received increased support, with 72 percent now in favor, compared with 67 percent in 2011. Opposition declined from 19 percent to 15 percent.
Sixty-six percent of respondents said doctors should be allowed to comply with the wishes of dying patients in severe distress who ask to have their lives ended, up from 58 percent in 2011. Opposition decreased from 20 percent in 2011 to 15 percent now.
"The very large -- more than 4-to-1 and increasing -- majorities in favor of physician-assisted suicide, and the right of terminally ill patients to end their lives are consistent with other liberal social policy trends, such as support for same-sex marriage, gay rights and the decriminalization of marijuana, seen in the results of referendums and initiatives in the recent mid-term elections," Taylor said.
Support for the right-to-die movement cut across all generations and educational groups, both genders, and even political affiliation, the poll found.
Democrats tended to be more supportive of right-to-die legislation, but 56 percent of Republicans said they favor voluntary euthanasia and 63 percent favor physician-assisted suicide.
Kavanaugh was not surprised. "People think of this as a liberal issue. But I find that as I talk to [conservatives], you can appeal to them on the basis of 'get the government the hell out of my life,'" he said.
But the public is split over how such policies should be enacted, with 35 percent saying that the states should decide on their own while 33 percent believe the decision should be made by the federal government, the poll found.
"Most of the people I know in the field whose opinion I put stock in don't feel there's ever going to be federal movement on it," Kavanaugh said. "You're just going to have to suffer through a state-by-state process."
Kavanaugh does believe this overwhelming public support will result in steady adoption of right-to-die laws.
"I think this will become the ultimate human right of the 21st century, the right to die with dignity," he said. "There are good deaths and bad deaths, and it is possible to have a good death."
Despite increasing public support for assisted suicide, stiff opposition remains in some quarters.
"Assisted suicide sows confusion about the purpose of life and death. It suggests that a life can lose its purpose and that death has no meaning," Rev. Alexander Sample, archbishop of the Archdiocese of Portland in Oregon, said in a pastoral statement issued during Maynard's final days.
"Cutting life short is not the answer to death," he said. "Instead of hastening death, we encourage all to embrace the sometimes difficult but precious moments at the end of life, for it is often in these moments that we come to understand what is most important about life. Our final days help us to prepare for our eternal destiny."
Todd Cooper, a spokesman for the Portland archdiocese, said the debate over assisted suicide touches him on a very deep level because of his wife, Kathie.
About 10 years ago, she also was diagnosed with terminal brain cancer. She endured two brain surgeries, two years of chemotherapy and six weeks of radiation therapy, and remains alive to this day.
"If she'd given up the fight for life, she wouldn't be here," Cooper said. "That doesn't necessarily happen in every case, but it gives hope for those who struggle to the very end."
Nursing students with previous caring experience are less likely to perform better academically and clinically than those who have none, research shows.
A study assessing the criteria for selecting nursing students found that high emotional intelligence did not mean students performed better on their courses.
Researchers also found that of the students who have withdrawn from their studies, nearly 60 per cent had previous caring experience.
The ongoing study, led by the University of Edinburgh, is tracking performance and emotional intelligence - the ability to recognise your own and other people's feelings and act accordingly - of nearly 900 nursing and midwifery students from the University of the West of Scotland and Edinburgh Napier University.
Researchers found, however, that performance improved with age and that female trainees scored significantly better than male counterparts.
The findings come after the 2013 Frances Report - which highlighted care failings at the Mid Staffordhire NHS Foundation Trust - recommended an emphasis on creating a more compassionate end empathetic culture in nursing.
As a result, aspiring nurses in England could potentially be required to spend a placement year as a carer before undertaking their training.
Lead researcher Rosie Stenhouse, lecturer in Nursing Studies at the University of Edinburgh, said: "The research should sound a note of caution to such pilot schemes. They are potentially expensive, politically motivated and not backed up by evidence."
This young girl is truly benevolent beyond her years.
Three-year-old Ariana Smith from Winterport, Maine watched a video from Extra Life, a charity that raises money for Children’s Miracle Network Hospitals through video gaming, that featured a girl who didn't have any hair. The curious kid then decided to ask her parents about what she saw, Josh Smith, Ariana's father, told the Huffington Post in an e-mail.
"She asked why the little girl had no hair. We explained that she was sick and that the medicine they were using made her hair fall out," Smith said.
The chat left a strong impression on Ariana.
“Without a second thought, Ariana said ‘Oh, well she can have some of my hair,’” Smith told ABC News.
So, on November 21st, the toddler received her first cut, and with the help of her parents, donated her hair to Locks Of Love. The pictures from the milestone, which were posted on Imgur, have since gone viral with over 500,000 views -- an ode to the 3-year-old's generosity.
"She could be so selfless like that," Smith told ABC News. "Her first reaction is ‘How about I give up something that I have so a little girl can feel pretty'."
While Ariana's act of kindness is a noble one, her father says that he wasn't surprised when she expressed her desire to donate her hair. He told HuffPost that she loves helping others -- even when she's playing.
"I think she’s just a caring person," he wrote. "She has a little play set of medical devices which she uses often. I’ve had my blood pressure and heart rate 'checked' hundreds of times this year."
As for Ariana's new hairstyle, the toddler seems to be adjusting quite nicely to her fashion statement.
"She loves it," Smith says of her daughter's new hairdo. "She can eat her breakfast without worrying about her hair drooping into it."
Researchers have developed a new device that may result in more comfortable mammography for women. According to a study being presented next week at the annual meeting of the Radiological Society of North America (RSNA), standardizing the pressure applied in mammography would reduce pain associated with breast compression without sacrificing image quality.
Compression of the breast is necessary in mammography to optimize image quality and minimize absorbed radiation dose. However, mechanical compression of the breast in mammography often causes discomfort and pain and deters some women from mammography screening.
An additional problem associated with compression is the variation that occurs when the technologist adjusts compression force to breast size, composition, skin tautness and pain tolerance. Over-compression, or unnecessarily high pressures during compression, is common in certain European countries, especially for women with small breasts. Over-compression occurs less frequently in the United States, where under-compression, or extremely low applied pressure, is more common.
"This means that the breast may be almost not compressed at all, which increases the risks of image quality degradation and extra radiation dose," said Woutjan Branderhorst, Ph.D., researcher in the Department of Biomedical Engineering and Physics at the Academic Medical Center in Amsterdam.
Overall, adjustments in force can lead to substantial variation in the amount of pressure applied to the breast, ranging from less than 3 kilopascals (kPa) to greater than 30 kPa.
Dr. Branderhorst and colleagues theorized that a compression protocol based on pressure rather than force would reduce the pain and variability associated with the current force-based compression protocol. Force is the total impact of one object on another, whereas pressure is the ratio of force to the area over which it is applied.
The researchers developed a device that displays the average pressure during compression and studied its effects in a double-blinded, randomized control trial on 433 asymptomatic women scheduled for screening mammography.
Three of the four compressions for each participant were standardized to a target force of 14 dekanewtons (daN). One randomly assigned compression was standardized to a target pressure of 10 kPa.
Participants scored pain on a numerical rating scale, and three experienced breast screening radiologists indicated which images required a retake. The 10 kPa pressure did not compromise radiation dose or image quality, and, on average, the women reported it to be less painful than the 14 daN force.
The study's implications are potentially significant, Dr. Branderhorst said. There are an estimated 39 million mammography exams performed every year in the U.S. alone, which translates into more than 156 million compressions. Pressure standardization could help avoid a large amount of unnecessary pain and optimize radiation dose without adversely affecting image quality or the proportion of required retakes.
"Standardizing the applied pressure would reduce both over- and under-compression and lead to a more reproducible imaging procedure with less pain," Dr. Branderhorst said.
The device that displays average pressure is easily added to existing mammography systems, according to Dr. Branderhorst.
"Essentially, what is needed is the measurement of the contact area with the breast, which then is combined with the measured applied force to determine the average pressure in the breast," he said. "A relatively small upgrade of the compression paddle is sufficient."
Further research will be needed to determine if the 10 kPa pressure is the optimal target.
The researchers are also working on new methods to help mammography technologists improve compression through better positioning of the breast.
U.S. health officials are poised to endorse circumcision as a means of preventing HIV and other sexually transmitted diseases.
The U.S. Centers for Disease Control and Prevention on Tuesday released its first-ever draft guidelines on circumcision that recommend that doctors counsel parents and uncircumcised males on the health benefits of the procedure.
The guidelines do not outright call for circumcision of all male newborns, since that is a personal decision that may involve religious or cultural preferences, Dr. Jonathan Mermin, director of the CDC's National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention, told the Associated Press.
But "the scientific evidence is clear that the benefits outweigh the risks," Mermin said.
Circumcision involves the surgical removal of the foreskin covering the tip of the penis. Germs can collect and multiply under the foreskin, creating issues of hygiene.
Clinical trials, many done in sub-Saharan Africa, have demonstrated that circumcision reduces HIV infection risk by 50 percent to 60 percent, the CDC guidelines note. The procedure also reduces by 30 percent the risk of contracting herpes and human papilloma virus (HPV), two pathogens believed to cause cancer of the penis.
The guidelines do point out that circumcision has only been proven to prevent HIV and sexually transmitted diseases in men during vaginal sex. The procedure has not been proven to reduce the risk of infection through oral or anal sex, or to reduce the risk of HIV transmission to female partners.
The scientific evidence is mixed regarding homosexual sex, the guidelines say, with some studies having shown that circumcision provides partial protection while other studies have not.
Circumcision does reduce the risk of urinary tract infections in infants, according to the CDC guidelines.
The most common risks associated with the procedure include bleeding and infection.
Male circumcision rates in the United States declined between 1979 and 2010, dropping from almost 65 percent to slightly more than 58 percent, according to a CDC report issued last year.
The new draft guidelines mirror an updated policy on circumcision released by the American Academy of Pediatrics in 2012.
"The American public should take confidence that these are pretty much converging guidelines. There is no doubt that it [circumcision] does confer health benefits and there is no doubt it can be performed safely, with a less than 1 percent risk of complications," Dr. Susan Blank, chair of the task force that authored the AAP policy statement, said Tuesday. "This is one thing a parent can do to protect the future health of their children."
In its policy statement, the AAP declared that the health benefits are great enough that infant male circumcision should be covered by insurance, which would increase access to the procedure for families who choose it, said Blank, who is also assistant commissioner of STD Control and Prevention at the New York City Department of Health and Mental Hygiene.
"The push from the academy's point of view is to really have providers lay out for parents what are the risks, what are the benefits, and give the parents the information they need to make a decision," Blank said. "And the academy feels strongly that since there are proven health benefits, the procedure should be covered by insurance."
The guidelines are expected to spur a response from anti-circumcision groups.
"There are certainly groups that are troubled by circumcision of an individual who is not in a position to provide their own consent," Blank said.
The public can comment on the draft guidelines through Jan. 16, according to the CDC.
Cancer is one of the leading causes of morbidity and mortality worldwide. In 2012, there were around 14 million new cases of cancer and around 8.2 million deaths from the disease. But despite such alarming numbers, a new study by researchers from the UK finds that most people ignore cancer warning signs, attributing them instead to symptoms of less serious illnesses.
Lead study author Dr. Katriina Whitaker, senior research fellow at University College London in the UK, analyzed the responses of 1,724 people aged 50 and over to a health questionnaire that was sent to them in April 2012.
The questionnaire asked participants whether they had experienced any of 17 symptoms, 10 of which are defined as cancer "alarm" symptoms by Cancer Research UK. These symptoms include unexplained cough, changes in mole appearance, unexplained bleeding, persistent change in bowel habits, unexplained weight loss, difficulty swallowing and unexplained lumps.
Participants were not told which symptoms are cancer warning signs.
The respondents were also asked what they thought was the cause of any symptoms they experienced, whether they deemed the symptoms to be serious and whether they visited their doctor as a result of their symptoms.
Only 2% of respondents considered warning symptoms to be cancer-related
Results of study - published in the journal PLOS ONE - revealed that 53% of participants reported that they had experienced at least one cancer warning sign over the past 3 months.
The most common cancer warning symptoms reported were persistent cough and persistent change in bowel habits, while unexplained weight loss and problems swallowing were the least common.
However, the researchers were surprised to find that of the respondents who reported cancer warning symptoms, only 2% considered cancer to be a potential cause.
What is more, Dr. Whitaker says that of participants who reported the most obvious signs of cancer - such as unexplained lumps or changes in mole appearance - most did not consider them to be cancer-related.
"Even when people thought warning symptoms might be serious, cancer didn't tend to spring to mind," adds Dr. Whitaker. "This might be because people were frightened and reluctant to mention cancer, thought cancer wouldn't happen to them or believed other causes were more likely."
On a positive note, respondents did deem the cancer warning signs to be more serious than symptoms not linked to cancer - such as shortness of breath, fatigue and sore throat- and 59% of those who experienced cancer warning signs visited their doctor.
But the researchers say their findings show that the majority of people are dismissing potential warning signs of cancer, which could be putting their health at serious risk. Dr. Whitaker says:
"Most people with potential warning symptoms don't have cancer, but some will and others may have other diseases that would benefit from early attention. That's why it's important that these symptoms are checked out, especially if they don't go away. But people could delay seeing a doctor if they don't acknowledge cancer as a possible cause."
"Most cancers are picked up through people going to their general practitioner (GP) about symptoms, and this study indicates that opportunities for early diagnosis are being missed," adds Sara Hiom, director of early diagnosis at Cancer Research UK. "Its results could help us find new ways of encouraging people with worrying symptoms to consider cancer as a possible cause and to get them checked out straight away with a GP."
Paul Alexander's most impressive accomplishment is something most people never think about.
He taught himself how to breathe.
Alexander, 67, is a victim of the worst that polio had to offer children in the late 1940s and early 1950s. At the age of 6, he was completely paralyzed by the disease, his lungs stopped working, and he was literally thrown into an iron lung.
Alexander has been in that iron lung for 61 years because he remains almost totally paralyzed, able to move only his head, neck and mouth. He is one of an estimated seven people in the United States who are still living in an iron lung, and yet he has had a long and successful career as a lawyer.
"Over the years, I've been able to escape this machine for a few hours at a time by teaching myself voluntary breathing," Alexander said recently as he lay in the iron lung at his home in Dallas, Texas. "I have to consciously push air into my lungs, something that's done involuntarily by just about everyone else. It's hard work, but it allows me to escape this infernal device, if only for a little while."
Alexander "escapes" the machine most often when he is litigating a case -- his specialty is family law -- or gives a speech.
While he sometimes condemns the contraption that keeps him alive, Alexander is most grateful for his iron lung, whose machinery is essentially unchanged from the first ones that were put in use in the late 1930s. His machine, in fact, is the same one he entered 61 years ago.
"It is my cage, but it's also my cocoon," he said, as the iron lung issued a noticeable whishing sound, an almost uncanny replication of normal breathing.
But we're getting ahead of the story.
This year marks the 60th anniversary of the nation's first mass polio vaccine inoculations, a time when hundreds of thousands of grade school students -- many of them throughout the South -- lined up in school gymnasiums, stuck out their arm and gritted their teeth as a nurse gave them Dr. Jonas Salk's experimental vaccine.
The shot was literally a game-changer. Most of these children had seen at least one or two classmates come to school on crutches, paralyzed by the ravages of polio. More than a few knew other students and friends who had died from the disease.
So 1954 signified their liberation during the summer -- they could return to public swimming pools and play in the rain and eat in restaurants and not be afraid that they would wake up the next day with a fever and terrible leg pains, which could rapidly lead to paralysis.
That's what happened to 6-year-old Paul Alexander in 1952, two years too early for the Salk vaccine.
"I remember it was really hot and raining, something that is sort of rare for Dallas in August," he recalled, "and my brother and I had been outside playing, running around and getting wet when the rain started.
"Our mother called for us to come in for dinner, and I remember her taking one look at me -- hot and wet and feverish -- and she cried out, 'Oh my God!' She ripped my clothes off and threw me onto her and my dad's bed and called the doctor.
"She knew right away that I had polio. I don't know how she knew, but she knew. I remember feeling hot and feverish, and for the next few days, I stayed in the bed and didn't move. I remember I had this coloring book, and I felt this compulsion to color as much as I could, sort of like maybe I wouldn't be able to do it in the future."
Why didn't Alexander's parents take him to the hospital? "Our family doctor said that all the kids with polio were at Parkland (Dallas' big municipal hospital), and he didn't want me there with the other kids because maybe I had a better chance to recover at home," Alexander said.
But all of that became moot about six days later when he could no longer move and found it difficult to breathe: "I remember having terrible pains in my legs, and breathing became really laborious. So they finally took me to Parkland."
And that's when the most horrifying event occurred before Alexander's long battle with polio could even begin: "I had become immobile; I don't think I could even talk, so the hospital staff put me on a gurney in a long hallway with all the other hopeless polio kids. Most of them were dead."
That would have been Alexander's fate, too, if not for Dr. Milton Davis, a well-known pediatric cardiologist who was examining all of the children in the hallway. "He took one look at me, gathered me up in his arms, and I think he performed a tracheotomy on me almost immediately so I could breathe," Alexander said. "And the next thing I remember, I was inside an iron lung."
And then he blacked out.
Alexander woke up weeks later still in the iron lung: "The pain was still there, although it seemed much less to me, and the iron lung pumped hot steam through a thick plastic water pump into my chest. This kept the mucuous loose enough so I could breathe."
He couldn't see through the steam at first, and he couldn't talk. But Alexander said he found some sort of determination within himself as strong as the iron in the device that was keeping him alive. "I decided I was going to fight this," he said. "I was going to have a life."
Eighteen months later, his parents brought him home. They stayed with him in shifts, fed him, helped him with school work (he was still enrolled in elementary school) and encouraged him to keep up his curiosity and enthusiasm for learning.
"My mother lobbied the school district for home-school learning, something very rare in the 1950s," he said. His dad fashioned a writing implement for him, similar to a T-square, which Alexander would put in his mouth and move around with his neck muscles in order to write.
Through their efforts and his own fierce determination, Alexander graduated high school as the class salutatorian. "I would have been valedictorian but the biology teacher gave me a B because I couldn't take lab," he joked.
Scholarships to Southern Methodist University in Dallas and the University of Texas in Austin allowed Alexander, with the help of a paid health aide, to get an undergraduate degree and then a law degree. He returned to the Dallas area and became associated with an Arlington law firm for a while, but eventually established a private practice that still handles everything from family law to financial cases.
"With help from a medical aide or one of my friends, I can get out of the lung and attend functions in a wheelchair or argue a case for a few hours," he said. "But I always have to remember to tell myself to inhale, exhale, inhale."
Alexander came to the attention this year of the leaders of the Dallas area's Rotary clubs through one of his doctors, Alexander Peralta, Jr., who is a Rotarian from Duncanville, Texas.
Rotary International has been working with the Bill and Melinda Gates Foundation to eliminate polio worldwide, just as smallpox has been eradicated.
"One of our clubs, which is well-versed in modern technology (the Dallas e-Club) went to Paul's house and made a four-minute video with him," said Bill Dendy, District Governor of District 5810, which has 65 local Rotary clubs in the north Texas area.
"What none of us realized at first is what a compelling story this is, not only Paul's triumphs under difficult circumstances, but also what a terrifying experience it can be, just sitting in the presence of that machine that keeps him alive. The iron lung personalizes the horror all those thousands of kids went through a little more than half a century ago," Dendy said. The video they made has been submitted to the local PBS station in Dallas.
Since making contact with Alexander, various district Rotary clubs have volunteered to make improvements to his house -- an old ramp leading to the front door was replaced -- and to be available to take him to his appointments. Throughout his life, Alexander has had a combination of help from health aides provided through the government and friends who pitch in.
Alexander said his iron lung is no longer supported by any company on an ongoing basis. The last company to service his machine, Philips Respironics, no longer does so. "So now, we have to strip spare parts from other discarded iron lungs to keep us going," he said. So far, it hasn't been a problem, he added: "There are only seven iron lung users left, so I don't think this is going to be a big problem of supply and demand."
How did he accomplish so much -- and keep his sense of humor -- while being virtually immobile for more than 60 years?
"It all starts with love," Alexander said. "My parents raised me in love. They taught me never to give up. They taught me the importance of relationships. They were always there for me.
"So, naturally, I had to reciprocate. And you know what? They were right. Anything is possible."
Researchers are using computed tomography (CT) and 3-D printing technology to recreate life-size models of patients' heads to assist in face transplantation surgery, according to a study presented today at the annual meeting of the Radiological Society of North America (RSNA).
Physicians at Brigham and Women's Hospital in Boston performed the country's first full-face transplantation in 2011 and have subsequently completed four additional face transplants. The procedure is performed on patients who have lost some or all of their face as a result of injury or disease.
In the study, a research team led by Frank J. Rybicki, M.D., radiologist and director of the hospital's Applied Imaging Science Laboratory, Bohdan Pomahac, M.D., lead face transplantation surgeon, and Amir Imanzadeh, M.D., research fellow, assessed the clinical impact of using 3-D printed models of the recipient's head in the planning of face transplantation surgery.
"This is a complex surgery and its success is dependent on surgical planning," Dr. Rybicki said. "Our study demonstrated that if you use this model and hold the skull in your hand, there is no better way to plan the procedure."
Each of the transplant recipients underwent preoperative CT with 3-D visualization. To build each life-size skull model, the CT images of the transplant recipient's head were segmented and processed using customized software, creating specialized data files that were input into a 3-D printer.
"In some patients, we need to modify the recipient's facial bones prior to transplantation," Dr. Imanzadeh said. "The 3-D printed model helps us to prepare the facial structures so when the actual transplantation occurs, the surgery goes more smoothly."
Although the entire transplant procedure lasts as long as 25 hours, the actual vascular connections from the donor face to the recipient typically takes approximately one hour, during which time the patient's blood flow must be stopped.
"If there are absent or missing bony structures needed for reconstruction, we can make modifications based on the 3-D printed model prior to the actual transplantation, instead of taking the time to do alterations during ischemia time," Dr. Rybicki said. "The 3-D model is important for making the transplant cosmetically appealing."
The researchers said they also used the models in the operating room to increase the surgeons' understanding of the anatomy of the recipient's face during the procedure.
"You can spin, rotate and scroll through as many CT images as you want but there's no substitute for having the real thing in your hand," Dr. Rybicki said. "The ability to work with the model gives you an unprecedented level of reassurance and confidence in the procedure."
Senior surgeons and radiologists involved in the five face transplantations agreed that the 3-D printed models provided superior pre-operative data and allowed complex anatomy and bony defects to be better appreciated, reducing total procedure time.
"Less time spent in the operating room is better for overall patient outcomes," Dr. Pomahac added.
Based on the results of this study, 3-D printing is now routinely used for surgical planning for face transplantation procedures at Brigham and Women's Hospital, and 3-D printed models may be implemented in other complex surgeries.
"It only takes one virus to get through for a person to be infected," explained Dr. John Mascola. This is true of any viral infection, but in this instance, Mascola is referring to HIV and his ongoing efforts to develop a vaccine against the virus. "It's been so difficult to make an HIV/AIDS vaccine."
Those were the words of many working in HIV vaccine development until the results of a 2009 trial in Thailand surprised everyone. "The field is energized," said Mascola, director of the Vaccine Research Center at the U.S. National Institute of Allergy and Infectious Diseases, describing the change in atmosphere in the vaccine community.
The trial included over 16,000 volunteers and was the largest clinical trial ever conducted for a vaccine against HIV. It was also the first to show any protection at all against infection.
Two previously developed vaccines, known as ALVAC-HIV and AIDSVAX, were used in combination, with the first priming an immune response against HIV and the second used as a booster once the immunity waned. The duo reduced the risk of contracting HIV by 31.2% -- a modest reduction, but it was a start.
To date, only four vaccines have made it as far as testing for efficacy to identify their levels of protection against HIV. Only this one showed any protection.
"That trial was pivotal," Mascola said. "Prior to that, it wasn't known whether a vaccine could be possible."
In recent years, there have been parallel findings of an equally pivotal nature in the field of HIV prevention, including the discovery that people regularly taking their antiretroviral treatment reduce their chances of spreading HIV by 96% and that men who are circumcised reduce their risk of becoming infected heterosexually by approximately 60%.
Both improved access to antiretrovirals and campaigns to increase male circumcision in high-risk populations have taken place since the discoveries, and although numbers of new infections are falling, they're not falling fast enough.
In 2013, there were 35 million people estimated to be living with HIV globally. There were still 2.1 million new infections in 2013, and for every person who began treatment for HIV last year, 1.3 people were newly infected with the lifelong virus, according to UNAIDS. A vaccine remains essential to control the epidemic.
A complex beast
Scientists like Mascola have dedicated their careers to finding a vaccine, and their road has been tough due to the inherently complicated nature of the virus, its aptitude for mutating and changing constantly to evade immune attack, and its ability attack the very immune cells that should block it.
There are nine subtypes of HIV circulating in different populations around the world, according to the World Health Organization, and once inside the body, the virus can change continuously.
"Within an individual, you have millions of variants," explained Dr. Wayne Koff, chief scientific officer for the International AIDS Vaccine Alliance.
HIV invades the body by attaching to, and killing, CD4 cells in the immune system. These cells are needed to send signals for other cells to generate antibodies against viruses such as HIV, and destroying those enables HIV to cause chronic lifelong infections in those affected.
Measles, polio, tetanus, whooping cough -- to name a few -- all have vaccines readily available to protect from their potentially fatal infections. But their biology is seemingly simple in comparison with HIV.
"For the older ones, you identify the virus, either inactivate it or weaken it, and inject it," Koff said. "You trick the body into thinking it is infected with the actual virus, and when you're exposed, you mount a robust immune response."
This is the premise of all vaccines, but the changeability of HIV means the target is constantly changing. A new route is needed, and the true biology of the virus needs to be understood. "In the case of HIV, the old empirical approach isn't going to work," Koff said.
Scientists have identified conserved regions of the virus that don't change as readily, making them prime targets for attack by antibodies. When the success of the Thai trial was studied deep down at the molecular level, the protection seemed to come down to attacking some of these conserved regions. Now it's time to step it up.
In January, the mild success in Thailand will be applied in South Africa, where over 19% of the adult population is living with HIV. The country is second only to bordering Swaziland for having the highest rates of HIV in the world.
"The Thai vaccine was made for strains (of HIV) circulating in Thailand," said Dr. Larry Corey, principal investigator for the HIV Vaccine Trials Network, which is leading the next trial in South Africa. The strain, or subtype, in this case was subtype B. "For South Africa, we've formed a strain with common features to (that) circulating in the population." This region of the world has subtype C.
An additional component, known as an adjuvant, is being added to the mix to stimulate a stronger and hopefully longer-lasting level of immunity. "We know durability in the Thai trial waned," Corey said. If safety trials go well in 2015, larger trials for the protective effect will take place the following year. An ideal vaccine would provide lifelong protection, or at least for a decade, as with the yellow fever vaccine.
A broad attack
The excitement now reinvigorating researchers stems not only from a modestly successful trial but from recent successes in the lab and even from HIV patients themselves.
Some people with HIV naturally produce antibodies that are effective in attacking the HIV virus in many of its forms. Given the great variability of HIV, any means of attacking these conserved parts of the virus will be treasured and the new found gold comes in the form of these antibodies -- known as "broadly neutralizing antibodies." Scientists including Koff set out to identify these antibodies and discover whether they bind to the outer coat of the virus.
The outer envelope, or protein coat, of HIV is what the virus uses to attach to, and enter, cells inside the body. These same coat proteins are what vaccine developers would like our antibodies to attack, in order to prevent the virus from entering our cells. "Broadly neutralizing antibodies" could hold the key because, as their name suggests, they have a broad remit and can attack many subtypes of HIV. "We will have found the Achilles heel of HIV," Koff said.
Out of 1,800 people infected with HIV, Koff and his team found that 10% formed any of these antibodies and just 1% had extremely broad and potent antibodies against HIV. "We called them the elite neutralizers," he said of the latter group. The problem, however, is that these antibodies form too late, when people are already infected. In fact, they usually only form a while after infection. The goal for vaccine teams is to get the body making these ahead of infection.
"We want the antibodies in advance of exposure to HIV," explained Koff. The way to do this goes back to basics: tricking the body into thinking it is infected.
"We can start to make vaccines that are very close mimics of the virus itself," Mascola said.
Teams at his research center have gained detailed insight into the structure of HIV in recent years, particularly the outer coat, where all the action takes place. Synthesizing just the outer coat of a virus in the lab and injecting this into humans as a vaccine could "cause enough of an immune response against a range of types of HIV," Mascola said.
The vaccine would not contain the virus itself, or any of its genetic material, meaning those receiving it have no risk of contracting HIV. But for now, this new area remains just that: new. "We need results in humans," Mascola said.
Rounds of development, safety testing and then formal testing in high-risk populations are needed, but if it goes well, "in 10 years, there could be a first-generation vaccine." If improved protection is seen in South Africa, a first-generation vaccine could be with us sooner.
Making an Impact
When creating vaccines, the desired level of protection is usually 80% to 90%. But the high burden of HIV and potentially beneficial impact of lower levels of protection warrant licensing at a lower percentage.
"Over 50% is worth licensing from a public health perspective," Koff said, meaning that despite less shielding from any contact with the HIV virus, even a partially effective vaccine would save many lives over time.
The next generations will incorporate further advancements, such as inducing neutralizing antibodies, to try to increase protection up to the 80% or 90% desired.
"That's the history of vaccine research; you develop it over time," Corey said. He has worked in the field for over 25 years and has felt the struggle. "I didn't think it would be this long or this hard ... but it's been interesting," he ponders.
But there is light at the end of tunnel. Just.
"There has been no virus controlled without a vaccine," he concluded when explaining why, despite antiretrovirals, circumcision and increased awareness, the need for a one-off intervention like a vaccine remains strong.
"Most people that transmit it don't even know they have it," he said. "To get that epidemic, to say you've controlled it, requires vaccination."
Amyotrophic lateral sclerosis - also known as Lou Gehrig's disease - is a condition that gradually attacks nerve cells that control our voluntary movement, leading to paralysis and death. In the US, a reported 30,000 individuals are living with the disease, but now, scientists have identified a fault in protein formation, which could be the origin of this condition.
The researchers, from the University of Wisconsin-Madison, have published their study on amyotrophic lateral sclerosis (ALS) in the journal Cell Stem Cell.
According to the Centers for Disease Control and Prevention (CDC), nobody knows for sure why ALS occurs, and there is currently no cure.
The researchers of this latest study, led by Su-Chun Zhang, senior author and neuroscientist at UW-Madison, say previously, a genetic mutation was discovered in a small group of patients with ALS, prompting scientists to transfer that gene to animals for drug treatment testing.
However, this approach has not yet worked. As such, Zhang and his team decided to study diseased human cells - called motor neurons - in lab dishes. These motor neurons are what direct muscles to contract, and Zhang explains this is where failures occur in ALS.
Discovery centers on faulty proteins inside motor neurons
Zhang was the first scientist to ever grow motor neurons from human embryonic stem cells around 10 years ago, and he has recently been transforming skin cells into induced pluripotent stem (iPS) cells, which are then transformed into motor neurons.
He explains that the iPS cells can be used as models for disease since they have many of the same characteristics as their donor cells.
"With iPS, you can take a cell from any patient, and grow up motor neurons that have ALS," Zhang explains. "That offers a new way to look at the basic disease pathology."
For their latest study, the researchers have focused on proteins that erect a transport structure - called a neurofilament - inside the motor neurons.
They say the neurofilament moves chemicals and cellular parts - including neurotransmitters - to far sides of the nerve cell.
Zhang explains that the motor neurons, for example, that control foot muscles are around 3 ft long, so they need to be moved a whole yard from the cell body to the spot where they can signal the muscles.
As such, one of the first signs of ALS in a patient who lacks this connection is paralysis of the feet and legs.
'Findings have implications for other neurodegenerative disorders'
Before now, scientists have understood that with ALS, so-called tangles - misshapen protein - along the nerve's paths block the route along the nerve fibers, which eventually results in the nerve fiber malfunctioning and dying.
The team's recent discovery, however, has to do with the source of these tangles, which lies in a shortage of one of three proteins in the neurofilament.
Zhang explains that the neurofilament plays both a structural and a functional role:
"Like the studs, joists and rafters of a house, the neurofilament is the backbone of the cell, but it's constantly changing. These proteins need to be shipped from the cell body, where they are produced, to the most distant part, and then be shipped back for recycling.
If the proteins cannot form correctly and be transported easily, they form tangles that cause a cascade of problems."
He says their discovery is that the origin of ALS is "misregulation of one step in the production of the neurofilament."
Additionally, he notes that similar tangles crop up with Alzheimer's and Parkinson's diseases: "We got really excited at the idea that when you study ALS, you may be looking at the root of many neurodegenerative disorders."
Zhang and his team also observed that this misregulation happens very early, which is why it is highly likely that what they found is the origin ALS.
"Nobody knew this before, but we think if you can target this early step in pathology, you can potentially rescue the nerve cell," he says.
And as if this discovery is not exciting enough, the team also found a way to rescue the neural cells in the lab dishes, and when they "edited" the gene that orchestrates formation of the blundered protein, they found that the cells suddenly looked normal.
They report that they are currently testing a wide range of potential drugs, which brings hope to the domain of ALS research.
The CDC have a National ALS Registry, where patients with the condition can complete brief risk-factor surveys to help scientists defeat ALS.
A brain abnormality may be responsible for more than 40 percent of deaths from sudden infant death syndrome (SIDS), a new study suggests.
The abnormality is in the hippocampus, a part of the brain that influences breathing, heart rate and body temperature. This abnormality may disrupt the brain's control of breathing and heart rate during sleep or during brief waking that happens during the night, the researchers report.
"This abnormality could put infants at risk for SIDS," said lead researcher Dr. Hannah Kinney, a professor of pathology at Harvard Medical School in Boston.
Kinney can't say for sure that this abnormality is a cause of SIDS. "We don't know at this stage. This is the first observation of this abnormality," she said. "It's just an observation at this point."
Before this brain abnormality can be called a cause of SIDS, Kinney said, they have to find out what causes this abnormality and determine if it alone can cause SIDS.
For the study, Kinney's team examined sections of the hippocampus from 153 infants who died suddenly and unexpectedly between 1991 and 2012. The deaths were classified as unexplained -- which includes SIDS -- or from a known cause, such as infection, accident, murder or lack of oxygen.
Kinney's group found that 41.2 percent of infants who died for an unexplained reason compared with 7.7 percent of those whose death was explainable had an abnormality in the part of the hippocampus known as the dentate gyrus.
Among the 86 infants whose death was classified as SIDS, 43 percent had this abnormality, the researchers added.
This change in the dentate gyrus suggests there was a problem in development at some point late in the life of the fetus or in the months after birth, Kinney said.
Kinney added that this abnormality has only been seen under the microscope after death, so a child cannot be tested for the abnormality.
"There are no signs or symptoms that predict SIDS or warn families that this problem is there or that SIDS is going to occur," she said.
The report was published online Nov. 24 in the journal Acta Neuropathologica.
"Until we understand more about this abnormality, parents should follow the safe sleep recommendations of the American Academy of Pediatrics," Kinney said.
The recommendation is to place an infant alone in a crib on the back without toys or pillows as bolsters. "The same messages we have always had are still applicable," she said.
SIDS is the leading cause of death of infants younger than 1 year of age in the United States, the researchers said.
Dr. Sayed Naqvi, a pediatric neurologist at Miami Children's Hospital, noted that this brain abnormality has been found in epilepsy, but this is the first time it has been linked to SIDS.
"This needs to be confirmed and more research done to say this is a cause of SIDS," he said.
Marian Willinger, a special assistant for SIDS at U.S. National Institute of Health's Eunice Kennedy Shriver National Institute of Child Health and Human Development, said in a statement, "The new finding adds to a growing body of evidence that brain abnormalities may underlie many cases of SIDS."
"The hope is that research efforts in this area eventually will provide the means to identify vulnerable infants so that we'll be able to reduce their risk for SIDS," she added.
The number of emergency department visits in the United States rose from about 130 million in 2010 to a record 136 million in 2011, according to the U.S. Centers for Disease Control and Prevention.
The findings also showed that fewer people were going to ERs with non-urgent medical needs: 96 percent of patients were identified as needing medical care within two hours of arriving at the ER. In 2010, that number was 92 percent, according to the research.
Sixty percent of patients arrived at the ER after normal business hours (after 5 p.m. on weekdays). One-third of visits were for patients on either end of the age spectrum -- younger than 15 or older than 65, the researchers found.
Almost 30 percent of visits were for injuries. The highest injury rates were among patients 75 and older, the study noted.
"The report also finds that there are large numbers of admitted patients who wait long times for inpatient beds," Dr. Michael Gerardi, president of the American College of Emergency Physicians (ACEP), said in an ACEP news release.
"Nearly two-thirds of patients waited two or more hours for beds in 2011, and nearly three-quarters of hospitals continued to board patients, even when the emergency department was critically overloaded. Hospitals must move admitted patients out of the emergency department faster to make room for the increasing number of people coming," he said.
It's believed that there will be about 140 million ER visits in 2014, according to the ACEP.
"The growth in patient demand aligns with what emergency physicians have been seeing and predicting: demand is going to increase," Gerardi said.
"Given that our nation's population is aging, and emergency departments have a critical role as the front line of responding to disasters and infectious disease outbreaks in America, such as what we saw with Ebola, we need to prepare for increased numbers of patients," he added.
Despite increasing use of ERs, most hospitals had not expanded their ERs as of 2011 and had no plans to expand them in the following two years, according to Gerardi.
"Emergency departments are essential to every community and must have adequate resources," he said. "They continue to be under severe stress and face soaring demands, despite the efficiency of caring for more than 136 million of the sickest patients each year using only 4 percent of the nation's health care dollar. This report is more evidence that we are going to need more resources, not less, in the future."
The current measles vaccine - administered by an injection - is effective and safe, but experts say coverage could be made better by a vaccine that is easier to administer and transport. Now, a measles vaccine consisting of dry powder that is delivered with a puff of air has proven safe in early human trials and effective in previous animal trials.
Though many people living in the US consider measlesto be a thing of the past - thanks, in large part, to widespread vaccination efforts - the disease has made a comeback in recent years.
In fact, 2014 has so far seen a record number of measles cases in the US, with 603 confirmed cases reported to the Centers for Disease Control and Prevention's (CDC) National Center for Immunization and Respiratory Diseases (NCIRD) between January 1st and October 31st.
The organization says this is the highest number of cases since measles elimination was confirmed in the US in 2000.
Measles is spread by droplets or direct contact with the nose or throat secretions of people who are infected, but it can also be spread through the air or by objects containing nose and throat secretions.
According to the World Health Organization (WHO), measles is "one of the most readily transmitted communicable diseases and probably the best known and most deadly of all childhood rash/fever illnesses."
In 2013, the disease killed 145,700 people worldwide - most of whom were children - despite an already existing effective injectable vaccine.
"Delivering vaccines in the conventional way, with needle injections, poses some serious challenges, especially in resource-poor parts of the world," says Prof. Robert Sievers, author of the latest study from the University of Colorado Boulder's Department of Chemistry and Biochemistry.
New vaccine safe, with evidence of positive immune response
To improve the delivery of the vaccine, Prof. Sievers and his colleagues created a dry delivery technique - that involves an inhalable, dry powder - in order to circumvent the need for injections and liquid storage, and to avoid risk of vaccine contamination.
In previous work, he and his team showed that their vaccine protected rhesus macaques and cotton rats from measles infection, and they also demonstrated that their dry vaccines can be safely stored for 6 months to 4 years at room temperature or in refrigerators kept at 36-46° F (2-8°C).
But their latest study heralds the success of the first phase 1 clinical trial for their vaccine in humans. "Out of an abundance of caution," says Prof. Sievers, "we test first in people who have already had the disease, or been injected earlier by needles with liquid vaccines."
As such, they enrolled 60 adult males aged 18-45 years who were already seropositive for the measles antibody. In the clinical trial, the researchers tested delivery of the powder using two devices and compared those two groups with a group that received the typical injection.
Results showed that the men from all three groups responded similarly and displayed no clinically relevant side effects. What is more, there was also evidence of a positive immune response to vaccination from the powder.
Any adverse events were recorded with diary cards for 28 days after the vaccination, and researchers followed the participants for 180 days post-vaccination to watch for any long-term adverse events. Additionally, the team measured measles antibodies 7 days before vaccination and 21 and 77 days after vaccination.
Commenting on their new dry vaccine, Prof. Sievers says:
"You don't need to worry about needles; you don't need to worry about reconstituting vaccines with clean water; you don't need to worry about disposal of sharps waste or other vaccine wastage issues; and dry delivery is cheaper."
Vaccine trials in humans are ongoing
Though their trial demonstrated that their powder vaccine is safe, because the men were already immune to measles, it could not compare effectiveness of the vaccines.
"It is very good news that we encountered no problems," says Prof. Sievers, "and now we can move on."
He and his team plan to continue their research through phase 2 and 3 trials in people who are not yet immune to measles, including women and children.
The research was funded by a $20 million grant from the Foundation for the National Institutes of Health, with support from the Bill and Melinda Gates Foundation. It should be noted that the authors of the paper include researchers from the Serum Institute of India, Ltd. - the largest manufacturer of childhood vaccines used in developing countries.
Additionally, Prof. Sievers is president and CEO of Aktiv-Dry, LLC, a Colorado-based company that provides dry powder solutions for the vaccine, pharmaceutical and biotechnology industries.
That’s right—there are men in nursing, too! It’s time to rid ourselves of outdated stereotypes. We don’t live in a society where boys only like blue and girls only like pink. Where boys can only play with legos and girls can only play with dolls. There’s too much variety in this world to limit ourselves to what we think is expected of us. There are women in engineering and mathematics, and there are men in nursing and healthcare.
Population Growing for Men in Nursing
Nursing is a fantastic career. In fact, the number of men in nursing is growing, with the percentage of male nurses increasing almost every year. In addition, there are more men in nursing schools, making up 13% of nursing school students. Find out more facts about male nurses by reading the men in nursing infographic below.
In the Future of Nursing report published by the Institute of Medicine, it is recommended that health care facilities throughout the United States increase the proportion of nurses with a BSN to 80 percent and double the number of nurses with a DNP by the year 2020. Research shows that nurses who are prepared at baccalaureate and graduate degree levels are linked to lower readmission rates, shorter lengths of patient stay, and lower mortality rates in health care facilities.
What does the job market look like for RNs who are looking to advance their careers?
We tackle this question in our latest infographic, “Career Paths for RNs,” where we look in-depth at the three higher education paths RNs can choose from to advance their careers — Bachelor of Science in Nursing, Master of Science in Nursing, and Doctor of Nursing Practice.
For each career path, we outline the various in-demand specialties, salaries, and job outlook.
In the wake of media focus on the trials and bravery of nurses in the context of the Ebola crisis, leaders in the fields of nursing and clinical ethics have released an unprecedented report on the ethical issues facing the profession, as the American Nursing Association prepares to release a revised Code of Ethics in 2015.
The report captures the discussion at the first National Nursing Ethics Summit, held at Johns Hopkins University in August. Fifty leaders in nursing and ethics gathered to discuss a broad range of timely issues and develop guidance. The report, A Blueprint for 21st Century Nursing Ethics: Report of the National Nursing Summit, is available in full online at www.bioethicsinstitute.org/nursing-ethics-summit-report. It covers issues including weighing personal risk with professional responsibilities and moral courage to expose deficiencies in care, among other topics.
An executive summary of the report is available at: http://www.bioethicsinstitute.org/wp-content/uploads/2014/09/Executive_summary.pdf
"This blueprint was in development before the Ebola epidemic really hit the media and certainly before the first U.S. infections, which have since reinforced the critical need for our nation's healthcare culture to more strongly support ethical principles that enable effective ethical nursing practice," says Cynda Hylton Rushton, PhD, RN, FAAN, the Bunting Professor of Clinical Ethics at the Johns Hopkins School of Nursing and Berman Institute of Bioethics, and lead organizer of the summit.
The report makes both overarching and specific recommendations in four key areas: Clinical Practice, Nursing Education, Nursing Research, and Nursing Policy. Among the specific recommendations are:
Clinical Practice: Create tools and guidelines for achieving ethical work environments, evaluate their use in practice, and make the results easily accessible.
Education: Develop recommendations for preparing faculty to teach ethics effectively
Nursing Research: Develop metrics that enable ethics research projects to identify common outcomes, including improvements in the quality of care, clinical outcomes, costs, and impacts on staff and the work environment
Policy: Develop measurement criteria and an evaluation component that could be used to assess workplace culture and moral distress
What does this blueprint mean for nurses on the front line?
"It's our hope this will serve as a blueprint for cultural change that will more fully support nurses in their daily practice and ultimately improve how healthcare is administered -- for patients, their families and nurses," says Rushton. "We want to start a movement within nursing and our healthcare system to address the ethical challenges embedded in all settings where nurses work."
On the report's website, nurses and the public can learn more about ethical challenges and proposed solutions, share personal stories, and endorse the vision of the report by signing a pledge.
"This is only a beginning," says Marion Broom, PhD, RN, FAAN, Dean and Vice Chancellor for Nursing Affairs at Duke University and Associate Vice President for Academic Affairs for Nursing at Duke University Health System. "The next phase is to have these national nursing organizations and partners move the conversation and recommendations forward to their respective constituencies and garner feedback and buy-in. Transformative change will come through innovative clinical practice, education, advocacy and policy."
At the time of publication, the vision statement of the report has been endorsed by the nation's largest nursing organizations, representing more than 700,000 nurses:
American Academy of Nursing
American Association of Critical-Care Nurses
American Nurses Association
American Association of Colleges of Nursing
American Organization of Nurse Executives
Association of Women's Health, Obstetric and Neonatal Nurses
Use of "antibiograms" in skilled nursing facilities could improve antibiotic effectiveness and help address problems with antibiotic resistance that are becoming a national crisis, researchers conclude in a new study.
Antibiograms are tools that aid health care practitioners in prescribing antibiotics in local populations, such as a hospital, nursing home or the community. They are based on information from microbiology laboratory tests and provide information on how likely a certain antibiotic is to effectively treat a particular infection.
The recent research, published by researchers from Oregon State University in Infection Control and Hospital Epidemiology, pointed out that 85 percent of antibiotic prescriptions in the skilled nursing facility residents who were studied were made "empirically," or without culture data to help determine what drug, if any, would be effective.
Of those prescriptions, 65 percent were found to be inappropriate, in that they were unlikely to effectively treat the target infection.
By contrast, use of antibiograms in one facility improved appropriate prescribing by 40 percent, although due to small sample sizes the improvement was not statistically significant.
"When we're only prescribing an appropriate antibiotic 35 percent of the time, that's clearly a problem," said Jon Furuno, lead author on the study and an associate professor in the Oregon State University/Oregon Health & Science University College of Pharmacy.
"Wider use of antibiograms won't solve this problem, but in combination with other approaches, such as better dose and therapy monitoring, and limiting use of certain drugs, we should be able to be more effective," Furuno said.
"And it's essential we do more to address the issues of antibiotic resistance," he said. "We're not keeping up with this problem. Pretty soon, there won't be anything left in the medical cabinet that works for certain infections."
In September, President Obama called antibiotic resistant infections "a serious threat to public health and the economy," and outlined a new national initiative to address the issue. The Centers for Disease Control and Prevention has concluded that the problem is associated with an additional 23,000 deaths and 2 million illnesses each year in the U.S., as well as up to $55 billion in direct health care costs and lost productivity.
Antibiograms may literally be pocket-sized documents that outline which antibiotics in a local setting are most likely to be effective. They are often used in hospitals but less so in other health care settings, researchers say. There are opportunities to increase their use in nursing homes but also in large medical clinics and other local health care facilities for outpatient treatment. The recent study was based on analysis of 839 resident and patient records from skilled nursing and acute care facilities.
"Antibiograms help support appropriate and prudent antibiotic use," said Jessina McGregor, also an associate professor in the OSU/OHSU College of Pharmacy, and lead author on another recent publication on evaluating antimicrobial programs.
"Improved antimicrobial prescriptions can help save lives, but they also benefit more than just an individual patient," McGregor said. "The judicious use of antibiotics helps everyone in a community by slowing the spread of drug-resistant genes. It's an issue that each person should be aware of and consider."
Multi-drug resistant organisms, such as methicillin-resistant Staphylococcus aureus, or MRSA, and other bacterial attacks that are being called "superinfections" have become a major issue.
Improved antibiotic treatment using a range of tactics, researchers say, could ultimately reduce morbidity, save money and lives, and improve patients' quality of life.
Each year, about one million babies throughout the world die of complications due to premature birth. Many of them could have been saved if given access to an incubator. But this expensive device is sorely lacking in developing countries. A young British researcher says he has found a solution -- a low-cost inflatable incubator.
Doctors say many expectant mothers in developing countries give birth prematurely, especially in refugee camps, largely because of poor diet and unhealthy living conditions.
Premature birth is the biggest killer of children worldwide. Because these tiny babies are born before their lungs are fully developed, they are more susceptible to often deadly infections. But they could survive if placed in an incubator, where they would continue to develop in the closed chamber and warm, controlled environment.
However with a price tag of around $50,000, incubators are out of reach even for some hospitals.
Design engineering student James Roberts, 23, of Britain says his $400 inflatable incubator may help solve this problem.
“It's basically an insulated piece of air, so it's like the difference between double and single glazing, so it's easier to keep the inside at a stable heat environment, heat temperature," he said.
The inflated incubator is collapsible and when folded resembles an ordinary travel bag.
It is powered through a regular electrical line, but Roberts said he has found a solution in case there is a power outage, which often happens in refugee camps.
“I thought 'why not car batteries?' There's loads of cars out there, they're pretty readily available. So you can plug this into a car battery. It will run for 24 hours and then when the mains [regular electrical line] comes back on, the mains can then charge this battery, and then that can run the incubator," he said.
Roberts' won the $47,000 James Dyson Award earlier this year for his incubator design. He said the project is still in the development phase, but the prize money will help him start a company for the mass manufacturing of inflatable incubators.
“HIT has been shown to help some patients, but it has also been shown to perhaps provide some complications in care, or less than adequate care, when messages are not received, when messages are interrupted or when messages are routed to the inappropriate person,” explained Milisa Manojlovich, PhD, RN, CCRN, associate professor at the University of Michigan School of Nursing (UMSN) and member of U-M’s Institute for Healthcare Policy and Innovation.
Manojlovich will serve as the primary investigator on a new $1.6 million grant from the federal Agency for Healthcare Research and Quality (AHRQ) that will focus on health IT’s effects on nurse–physician communication. Manojlovich and her co-investigators will look at how communication technologies make it easier or harder for doctors and nurses to communicate with each other. They hope their research will identify the optimal way to support effective communication while fostering improved and positive interdisciplinary team-based care.
Until the research is completed, Manojlovich offers some simple procedures clinicians can begin to adopt right now to help alleviate common problems with digital communication:
1. Use multiple forms of technology
Just like there is more than one way to treat a cold, there is more than one way to communicate electronically. Utilizing multiple forms of technology to communicate important information, or sometimes even reverting back to the “old-fashioned” ways of making a phone call or talking in person, can help ensure the receipt of a message in an environment that is often inundated.
“One of the things we are going to investigate is this idea of matching the message to the medium,” Manojlovich said. “So depending on the message that you want to send, you will identify what is the best medium to send that message.”
Using the current Ebola situation in Texas as an example, Manojlovich explained that using multiple forms of technology as a back-up to solely documenting the information in the EHR system could have mitigated the breakdown in communication that occurred. “Although the clinician did her job by entering the information into the EHR, she maybe should have texted or emailed the physician with the information or found someone to talk to in person about the situation. What we are trying to do with this study is see if there is another way that messages like this could have been transmitted better.”
2. Include the whole message
Reducing fragmented messages and increasing the aggregation of key data and information in communications may be one of the most critical pieces to improving communication between nurses and physicians. Manojlovich has been passionate about nurse–physician communication throughout her career and has conducted several previous studies on communication technologies.
“What we’ve noticed, for example, is that nurses will sometimes use the same form of communication over and over again. In one of the studies we actually watched a nurse page the same physician three times with the same question within an hour period.”
The physician did not answer any of the messages, and Manojlovich concluded it was because the pages were missing critical components of information related to the patient’s care plan. Increasing the frequency of communications can be beneficial, but only if the entire message and all important facets of information are relayed.
“If you do what you’ve always done, you’re going to get what you’ve always gotten. If you don’t alter or change the communication technology you are using, you are going to get the same results,” she added.
3. Incorporate a team-based approach
“At a really high level the problem is that a lot of these computer and electronic health record technologies are built with individuals in mind,” Manojlovich said. “When you talk about care process and team processes, that requires more interaction than the technologies are currently able to give us. The computer technologies are designed for individual use, but health care is based on the interaction of many different disciplines.”
Infusing this collaborative mindset into the “siloed” technology realm will undoubtedly help to improve the communication problems between providers and clinicians at all levels and all practice settings--which is especially important in today’s environment of co-morbidities and coordinating care.
Nurses play a critical role in improving communication as frontline care providers. “Nurses are the 24-hour surveillance system for hospitalized patients. It is our job to do that monitoring and surveillance and to let physicians know when something comes up.”
“I believe that for quality patient care, a patient needs input from all disciplines; from doctors, nurses, pharmacists, nutritionists--everyone,” Manojlovich said. “We are being trained separately and each discipline has a different knowledge base, and these differences make it difficult for us to understand each other. Developing mutual understanding is really important because when we have that mutual understanding I think outcomes are better and it can be argued that the quality of care is better when you have everyone providing input.”
More and more people are seeking care in emergency departments, leading to crowding and extended wait times that can adversely affect patient satisfaction and outcomes. Many nurses, including ER nurses, have come up with ideas to improve throughput and enhance care.
“Wait times are a very prevalent problem,” said Paula Roe, BSN, MBA/HCM, FACHE, senior consultant with Simpler Consulting, based in Pittsburgh, Penn. “There are many things that can be done.”
Roe helps clients discover waste through Lean principles and thereby reduce ER wait times.
At the end of 2013, ProPublica launched an interactive news application called ER Wait Watcher, using government information to educate people about average wait times at emergency departments (EDs). ER Wait Watcher reports a national average waiting time of 28 minutes before the patient sees a physician.
The American College of Emergency Physicians reported in April 2014 that 46 percent of surveyed members reported an increase in emergency department patients since January 1, 2014. Most respondents, 94 percent, did not believe wait times were the biggest issue facing emergency patients and their ability to access care, however. Interestingly, their top concern was the limited supply of primary care physicians, followed by too many non-urgent patients that might instead be treated in a primary care setting.
Deena Brecher, MSN, RN, APN, ACNS-BC, CEN, CPEN, president of the Emergency Nurses Association, agreed that a lack of primary care contributes to ED crowding and waiting.
In a recent interview, she pointed out that patients boarded in the ED also stop the flow and lead to crowding. Other people have to wait longer because the ED stretcher is occupied. To solve the problem, Brecher said hospitals must involve the entire hospital in getting patients ready for discharge out, the beds cleaned and the transfers made.
“You have to think of crowding as a hospital problem and not an emergency department problem,” Brecher explained. “It involves an organizational effort.”
Jodi Pahl, chief nursing executive at St. Rita’s Medical Center in Ohio, and the team at St. Rita’s launched a comprehensive communications program to keep all hospital clinicians informed of when patient wait times in the ED increase beyond acceptable levels. Those communications may prompt physicians to discharge patients ready to go home more quickly. As a result of this program, St. Rita’s was able to decrease patient wait times, as well as walk-out rates. Patients wait to see the doctor an average of 34 minutes at St. Rita’s, according to ER Wait Watcher.
Several hospitals have opened fast-track systems to reduce wait time, by getting the “walking well” in and out, Brecher said. She also reported an increase in the use of provider-nurse teams at the initial point of entry. Tests can be ordered so results are available more quickly once the patient enters the ED. Patients with minor ailments can be treated and released.
Charge nurse Steven Kunz, RN, CEN, of Aria Health’s Torresdale campus emergency department in Northeast Philadelphia, reported that reducing ER wait times and improving care are the key focus areas of the hospital’s new emergency department.
“Our strategic group of stakeholders including nurses, physicians and administration, worked together to implement an updated registration system that includes a pivot nurse to help transform triage,” Kunz said.
The pivot nurse greets patients upon their arrival, obtains patient identifiers and vital signs, and performs a rapid assessment to determine the level of need for immediate care. The pivot nurse concept, combined with an expanded treatment area and more rapid evaluation and disposition by the physician, have worked to reduce wait times and improve patient satisfaction, he added.
Penne Marino, RN, and colleagues at Lancaster General Hospital in Pennsylvania described in the Journal of Emergency Nursing in 2014 how a multidisciplinary team established a Bypass Rapid Assessment Triage process. Patients are met by a greeter nurse, who conducts a quick assessment to determine acuity and then places the patient in an appropriate bed. This new system reduced the time it took patients to see the physician and enhanced patient satisfaction. According to ER Wait Watcher, patients are seen by a doctor within 17 minutes.
The University of Kansas Medical Center (KUMC) in Kansas City, Kan., hired a bachelor’s-prepared emergency registered nurse as a flow coordinator in hopes of reducing its wait times. Seamus Murphy, BSN, RN, CEN, CPEN, CTRN, CPHQ, NREMT-P, at KUMC, and colleagues reported in the Journal of Emergency Nursing in 2014 how the flow coordinator decreased length of stay by 87.6 minutes, reduced the number of patients who left without being seen and decreased the number of time the hospital was on diversion. ER Wait Watcher reports an average wait time to see a physician is 34 minutes and more than eight hours for admitted patients to be roomed.
Nurses remain on the forefront of trying to improve throughput and reduce ER waiting times. Roe explained that nurses can assess improvements in three areas: triage, evaluation by medical staff and associated diagnosis and treatment, and then disposition.
“Each phase has its unique opportunities to eliminate barriers, reduce waste and improve wait times,” Roe said. “Nursing and how nurses deliver care is key in process improvement efforts. It’s important they are involved as frontline staff and part of studying the current state, helping to identify barriers to patient flow and understanding the solutions to deploy to make the situation better.”
Talking bystanders through CPR methods for a cardiac emergency during a 911 call can significantly boost survival rates, a new study suggests.
State researchers in Arizona examined the aggressive use of so-called pre-arrival telephone CPR guidelines -- step-by-step dispatcher instructions on administering cardiopulmonary resuscitation before trained rescuers arrive -- and found that it bumped survival of cardiac arrest patients from about 8 percent to more than 11 percent.
Cardiac arrest occurs when the heart's normal rhythm abruptly stops, and the organ can no longer pump blood and oxygen to the body. It can be triggered by a heart attack, but the two conditions are different.
Lead researcher Dr. Ben Bobrow said the type of focused intervention studied in his home state -- not only training telephone dispatchers but measuring bystander CPR outcomes and circling back to 911 centers with feedback -- is not done uniformly on a national basis, despite American Heart Association (AHA) guidelines.
But he hopes the results of his study, scheduled to be presented Saturday at the AHA meeting in Chicago, will promote that ideal.
"We believe strongly that this may be the best, and most efficient, way to improve survival rates across the country," said Bobrow, the medical director of the Bureau of EMS and Trauma System for the Arizona Department of Health Services. "Cardiac arrest is one of the leading causes of death, and as a country, despite tons of efforts ... this has not improved."
About 359,000 people in the United States suffered sudden cardiac arrest outside of a hospital setting in 2013, and more than 90 percent of them died, according to the AHA.
The heart association also has reported that 70 percent of Americans feel helpless to act during a cardiac arrest emergency because they don't know CPR or their training had lapsed.
Bobrow and his colleagues analyzed more than 4,000 audio recordings from 911 calls over three years from eight Arizona dispatch centers. That information, paired with emergency medical services (EMS) and hospital outcome data, showed that providing telephone CPR instructions prompted a jump in the number of bystanders implementing CPR, from 44 percent to 62 percent.
With the guidelines in place, the average amount of time elapsing between a bystander's call to 911 and the first chest compression in CPR dropped by 23 seconds, to 155 seconds.
"This research shows . . . that even the simplest of interventions, like having someone on the other end of a phone guide you [in CPR], can result in a remarkable difference of outcome," said Dr. Vinay Nadkarni, a spokesperson for the AHA, who wasn't involved in the study.
"That change is possible with a cellphone and our own two hands," added Nadkarni, an associate professor of anesthesiology and critical care at the University of Pennsylvania School of Medicine. "It's within our grasp."
Nadkarni said that Bobrow and his team had done an "excellent job" in helping 911 dispatchers in Arizona use certain phrases to prompt quick action among bystanders who witness a cardiac arrest.
For example, before the intervention, dispatchers typically asked 911 callers if anyone was available to perform CPR, or if they would be willing to. After the Web-based and live training, the revised script emphasized the importance of dispatchers directing callers to start CPR, saying something like, "You need to do chest compressions and I'm going to help you. Let's start."
With the apparent success of this approach, Bobrow said he and his team have asked the U.S. Centers for Disease Control and Prevention to consider implementing it on a national scale. Funding for such a program is needed, he said.
"It would be an incredibly inexpensive intervention for how many lives it would save," he said. "We estimate conservatively that it would save several thousand lives per year. It's not complicated stuff . . . and the beauty of the 911 system is that it already exists."
Research presented at scientific conferences typically has not been peer-reviewed or published and results are considered preliminary.
Using the Internet to access health information may be out of reach for many older Americans, according to a study by researchers at the University of Michigan. According to the study, less than one-third of Americans age 65 and older use the Web. Within that age group less than 10 percent of those with low health literacy, or who lack the ability to navigate the healthcare system, go online for health-related matters.
The results of the study have been published in the Journal of Internal Medicine. Data was analyzed from the 2009 and 2010 Health and Retirement Study, a nationally representative survey of older adults; about 1,400 of the participants were asked about how often they use the Internet for any purpose, and, in particular, how often they search for health and medical information.
Health literacy was found to be a significant predictor or what people do once they are online. Elderly Americans with low health literacy are less likely to use the Internet at all, according to the researcher; and if members of this group do surf the Web, it is not generally to search for medical or health information.
“In recent years, we have invested many resources in Web-based interventions to help improve people’s health, including electronic health records designed to help patients become more active participants in their care,” according to lead author of the study Helen Levy, Ph.D., research associate professor at the University of Michigan Institute for Social Research, in a prepared statement. “But many older Americans, especially those with low health literacy, may not be prepared for these tools.”
Senior author Kenneth Langa, M.D., a professor of Internal Medicine at the University of Michigan Medical School, cautions that as the Internet becomes more central to health literacy, older Americans face barriers that may sideline them. He recommends that “Programs need to consider interventions that target health literacy among older adults to help narrow the gap and reduce the risk of deepening disparities in health access and outcomes.”
A number of eye conditions can be treated by administering drugs directly into the eye. Yet, conventional needles have a bunch of drawbacks, including the patients’ fear of needles entering such fragile parts of the body and the difficulty of accurately administering medication into a targeted region of the eye. For glaucoma, for example, eye drops are prescribed which have a shorter active lifetime and are often skipped by the patients. An easy injection that works for months at a time would help control the disease considerably better.
Researchers at Georgia Tech and Emory University have been working on microneedles and formulations to safely and effectively deliver drugs into the eye. The microneedles are designed to only penetrate to the correct depth and the formulations need to be viscous enough to stay in place and release their therapeutic compounds in a controlled fashion. The researchers have already tested the microneedles on laboratory animals and showed that they can place drugs within the targeted sections of the eye.
More from Georgia Tech:
The microneedle therapy would inject drugs into space between two layers of the eye near the ciliary body, which produces the aqueous humor. The drug is retained near the injection side because it is formulated for increased viscosity. In studies with an animal model, the researchers were able to reduce intraocular pressure through the injections, showing that their drug got to the proper location in the eye.
Because the injection narrowly targets delivery of the drug, researchers were able to bring about a pressure reduction by using just one percent of the amount of drug required to produce a similar decline with eye drops.
To treat corneal neovascularization, the researchers took a different approach, coating solid microneedles with an antibody-based drug that prevents the growth of blood vessels. They inserted the coated needles near the point of an injury, keeping them in place for approximately one minute until the drug dissolved into the cornea.
In an animal model, placement of the drug halted the growth of unwanted blood vessels for about two weeks after a single application.
Twice a day, Michele Forth drives 45 miles to the Neonatal Intensive Care Unit to visit her 4-month-old baby she affectionately calls "Miss Madilyn." She is a 6-pound fighter in pink pajamas — but to her family and the nurses who care for her day and night, she is so much more.
"Hi, pumpkin! You just waking up?" Forth coos. Nurse Adrianna "Adri" Zimmerman, wearing purple scrubs and a warm smile, hands Madilyn to her father who is quickly surrounded by his wife and two young sons.
"She fights harder than any adult that I know, let alone a 6-pound baby," says father Shane Forth, softly stroking Madilyn's delicate left foot in his hand.
It was in that spirit that the nurses chose to see Madilyn, one of nearly 100 babies cared for in the NICU at Children’s Healthcare of Atlanta every day. "We always talk about how feisty this one is or how sweet this one is,” Zimmerman says.
That bedside chatting took on a whole new life with a photo series called "From the NICU to the Moon" that imagines what the babies dream about as they wiggle and smile in their sleep, and what they might become someday. It also aims to educate parents about safe sleep for newborns.
The nurses and hospital communications team imagined Madilyn as a physician, surrounded by stethoscopes and Band-Aids. The photo series also features Brentley, the future astronaut, Arianna, the future chef, Sofia the ballerina, and Carolina as an Olympian.
Madilyn was born two months early and has what is called vacterl association (a collection of birth defects), resulting in multiple surgeries and months in the NICU. Zimmerman remembers Madilyn's arrival in the NICU like it was her own child.
"I think she's strong and she's definitely got the will to see whatever it is through to the end, so, if that happens to be med school in a few years, I would not be surprised," says Zimmerman. "It's funny how much personality these babies have."
And Mom is happy with the depiction. "Even though Miss Madilyn does have a whole bunch of obstacles ahead of her right now," she says, "she can do amazing things and she can aspire to be anything that she wants to be."
Carolina, the tiny Olympian, is “a strong-willed patient who has a lot of heart and she is letting nothing hold her back," says Jessica Wright, a NICU Nurse with 10 years of experience. "Just because they were born early doesn't mean they cannot do whatever they want when they grow up in life."
True to her athletic depiction, Carolina is hardly ever still in her crib. Gazing up at the green alligator and orange lion of her soother, Carolina playfully kicks her feet back and forth, her bright eyes fixed on Nurse Wright. "What are you thinking about?" Wright asks, her hand on Carolina's blue and pink ensemble, "You tell 'em about it, wiggle worm."
Sofia, the ballerina in the photo series, is also on the move. Since she was photographed, Sofia was able to leave the NICU and go home with her parents, Fred and Dawnyale "Dawny" Hill.
In the pale orange light of an Atlanta sunset, Fred and Dawny cradle their daughter in their arms on the family's front porch. It's Sofia's first time outside on the porch and her longest stint outside in the evening since she went home. "What do you think? What do you think? Hill asks his daughter, holding her hand. "Interesting, huh?"
Sofia spent 157 days, 20 hours, and 6 total minutes in NICUs. Respiratory and reflux issues keep this 5 1/2-month-old on an oxygen tank and feeding tube.
"She has some accessories, as we like to refer to them as," says Mr. Hill, about the oxygen tank and tubes. "They kind of travel with her."
But in the "NICU to the Moon" photos, Sofia left all the tubes behind for the stage and curtains. "It made her seem normal. The way the pictures kind of erased all of the cords. All of the tubes," says Hill of his daughter. "I saw the innocence of Sofia as opposed to my child in the NICU."
"She's got a family full of dancers on both sides so we definitely are excited to see Miss Sofia the ballerina come about," Dawny says with a laugh. "She'll be dancing around."
But for now, the Hills cherish moments with Sofia at home, like their evening bedtime routine. Mr. Hill carries Sofia on his chest while Dawny wheels the oxygen tank and other cords towards the bedroom. "Good holding your head, Sofia. Look at you," applauds Mrs. Hill.
As they gently place her on her back in her crib, Sofia rubs her eyes.
"Hey, you had a good day. You had a good day, right? Are you sleepy?" asks her father, the machine beeping and sighing next to the crib.
"Ready? Time to pray," Mr. Hill says, kneeling over the crib next to his wife. They pray for every organ in their daughter's body and give thanks to the doctors who helped bring her home.
"We will be keeping up our bedtime routine," Mrs. Hill says, looking at her husband. "Until she can start saying her prayers," he answers.
"Any child that has to go through that much opposition from day one, there's got to be something great for them to accomplish out of life, so my hope is that she accomplishes exactly what she was sent here to do," Mr. Hill says.
And with that, the bedroom light switches off and one more former NICU baby gets to dream of her future in her own crib.
As Jill Koziol turned away from her 8-month-old daughter to check on her toddler, the unthinkable happened. In a fraction of a second little Cate pulled herself up against the laundry hamper, grabbed a detergent pod and popped it into her mouth.
Koziol heard a gagging sound, whipped around and was horrified to see the remains of the pod on the floor and Cate in obvious distress.
"The next few moments were very chaotic with a screaming child, me crying and screaming to poison control to be heard over Cate's cries," the 34-year-old New Yorker said.
Within minutes Cate was vomiting and the Koziols were in an ambulance racing to the hospital.
Cate Koziol is hardly alone in her run-in with a detergent pod. A study published on Monday in Pediatrics finds that in 2012 and 2013 17,230 children under age 6 got into trouble with detergent pods. Most — nearly 80 percent — of the children were reported to have ingested a pod. Nearly two-thirds of the children were between 1 and 2 years old.
“The severity of these exposures varies,” said study coauthor Dr. Gary Smith, director of the Center for Injury Research and Policy at Nationwide Children’s Hospital in Columbus, Ohio. “Sometimes the chemicals get into the eyes, sometimes they are swallowed. And if they are swallowed, they can cause severe burns to the esophagus and the stomach.”
It shouldn’t be surprising that most of the problems involved 1- and 2-year-old kids putting pods into their mouths, Smith said.
“This is the age group where they explore the environment with their mouths,” he explained.
A big part of the problem is that the chemicals in the pods are more dangerous than those in traditional laundry detergents.
“I’ve been treating children for over 30 years in emergency departments,” Smith said. “And for decades if a child came in with a laundry detergent exposure it was usually no big deal. But these are different. They have strong concentrated chemicals in them. And that’s why it’s so important for parents to understand the dangers associated with their use.”
Smith and his colleagues found that among children exposed to the packets, about half were managed at home and 35 percent were treated and released from a health care facility. One child died.
“The concern we have is that in about 700 of these children — that’s a child every day in this country — they had to be admitted to the hospital,” Smith said, adding that some ended up in pediatric intensive care units either in a coma or unable to breathe without the help of mechanical ventilation.
Andrea Gielen, director of the Johns Hopkins Center for Injury Research and Policy, hopes the new findings will be a wake up call for parents.
“I think it is definitely intended to alert parents to a hazardous household product that they need to make sure is tucked away from where young children can access — much like other dangerous household products, said Gielen, a professor at the Johns Hopkins Bloomberg School of Public Health.
In a statement the American Cleaning Institute said, “ACI and its member companies have directly engaged parents and caregivers, as well as poison control centers, pediatricians and other medical professionals, educators and social service providers in alerting them to the potential for childhood accidents involving these products.”
A recent survey by the institute suggests that many parents are unaware of the dangers. While 70% of those surveyed said they store household cleaners — such as dishwashing detergent and glass and toilet cleaners — safely and securely, just 34 percent reported properly storing their laundry pods in a cabinet or a cabinet with a lock, the ACI found. More worrisome, one out of six people admitted to taking no safety precautions at all when it came to storing laundry pods.
That wasn’t the case in the Koziol home. In the minutes before Cate got into trouble with one, Jill Koziol had taken a single pod down and set it on the family’s hamper to get everything ready for her husband to take to their apartment’s laundry room.
The Koziols’ experience is “a perfect example of how these things can happen in the blink of an eye,” Gielen said.
But Gielen said the onus isn’t just on parents. The new study should sound the alarm for product designers, too. “When you are designing a new product you need to be thinking about the most vulnerable part of the population and how it will interact with the product. In this case, it is kids,” she said
When the Koziols arrived at the emergency room, doctors decided to keep Cate there for observation. And it was a good thing they did. Within a couple of hours the little girl was wheezing and struggling to breathe. Her doctors decided to intubate her and Cate spent the next two days in the pediatric intensive care unit.
The whole experience was frightening, but Cate pulled through unscathed.
“Cate is back to normal, though mommy may never quite recover from the ordeal,” Koziol said.
Have you or someone you know dealt with a child who ate a laundry pod? If so, please share your experience.
Many people have been told, incorrectly, that they're allergic to penicillin, but have not had allergy testing. These people are often given alternative antibiotics prior to surgery to ward off infection. But when antibiotic choices are limited due to resistance, treatment alternatives may be more toxic, more expensive and less effective.
According to two studies presented at the American College of Allergy, Asthma and Immunology (ACAAI) Annual Scientific Meeting, people who believe they have a penicillin allergy would benefit from consultation from an allergist and penicillin allergy skin testing. Once they know if they are allergic, they can be given appropriate -- and not more resistant -- treatment prior to surgery. Of the 384 people in the first study who believed they were allergic to penicillin, 94 percent tested negative for penicillin allergy.
"A large number of people in our study who had a history of penicillin allergy were actually not allergic," said allergist and ACAAI member Thanai Pongdee, MD, lead study author. "They may have had an unfavorable response to penicillin at some point in the past, such as hives or swelling, but they did not demonstrate any evidence of penicillin allergy at the current time. With that in mind, their doctors prescribed different medications prior to surgery."
In the second study, 38 people who believed they were allergic to penicillin were given penicillin skin testing to see if it was possible to help reduce the use of high-cost antibiotics. Of the 38 people tested, all of them tested negative to an allergy for penicillin. Once it was known they weren't allergic to penicillin, the medical center was able to change the medications of 29 of the patients, thereby significantly lowering prescription costs.
"When you are told you have an allergy to something, it's important to be seen and tested by an allergist, who has the specialized training needed for accurate diagnosis and treatment," said allergist James Sublett, ACAAI president-elect. "If you're truly allergic to a medication, your allergist will counsel you on an appropriate substitute."
It is well known that exercise is good for the mind and body, but to what extent does the neighborhood or community in which we live affect our physical and mental health? New research from the University of Kansas suggests the walkability of a community has a great impact on cognition in older adults.
Previous studies have detailed the importance physical exercise has for executive function in older adults.
But how can the layout of a neighborhood encourage its residents to get out and walk? This is precisely what Amber Watts, assistant professor of clinical psychology at the University of Kansas, wanted to find out.
"Depending on which type of walking [leisure vs. walking to get somewhere] you're interested in, a neighborhood might have different characteristics," she says. "Features of a neighborhood that encourage walking for transportation require having someplace worth walking to, like neighbors' houses, stores and parks."
She adds that neighborhoods that encourage leisure walking have "pleasant things to look at," including walking trails and trees, and they should feel safe.
Her research, which she presented yesterday at the Gerontological Society of America's annual meeting in Washington, DC, suggests that neighborhoods that encourage walking can protect against cognitive decline in older adults.
To conduct her research, Watts used geographic information systems (GIS) to judge walkability. This involved maps that measure and analyze spatial data.
Better physical and mental health
Detailing how she collected her data, Watts explains:
"GIS data can tell us about roads, sidewalks, elevation, terrain, distances between locations and a variety of other pieces of information. We then use a process called space syntax to measure these features, including the number of intersections, distances between places or connections between a person's home and other possible destinations they might walk to."
She also looked at how complicated a route is from one location to another: "For example, is it a straight line from point A to point B, or does it require a lot of turns to get there?"
To conduct the study, Watts and colleagues tracked 25 people with mild Alzheimer's disease and 39 older adults without any cognitive impairment. Using the space syntax data, they created a "walkability score" for the participants' home addresses.
Then, they estimated the relationship between a person's neighborhood scores and how well they performed on cognitive tests over 2 years. The cognitive tests included three categories: attention, verbal memory and mental status. The team also factored in issues that might influence cognitive scores, including age, gender, education and wealth.
Results from the study suggest that communities that are easier to walk in are linked to better physical health outcomes - such as lower body mass and blood pressure - and cognition - including better memory.
Watts and her colleagues believe their findings could benefit older adults, health care professionals, caregivers and even architects and urban planners.
Do mentally complex neighborhoods act like a brain-training game?
Though elaborate community layouts may be expected to confuse older residents, Watts and her team found that they actually serve to keep cognition sharp.
"There seems to be a component of a person's mental representation of the spatial environment, for example, the ability to picture the streets like a mental map," Watts says.
She adds that complicated environments may demand more intricate mental processes in order to navigate them, which could keep the mind sharp. This is in line with previous studies, which have demonstrated how staying mentally active helps to preserve memory.
"Our findings suggest that people with neighborhoods that require more mental complexity actually experience less decline in their mental functioning over time," Watts adds.
She explains that a challenging environment keeps an individual's body and mind healthy:
"With regard to the complexity of neighborhood street layouts - for example, the number of turns required getting from point A to point B - our results demonstrate that more complex neighborhoods are associated with preserved cognitive performance over time.
We think this may be because mental challenges are good for us. They keep us active and working at that optimal level instead of choosing the path of least resistance."
A National Institute on Aging grant, KU Strategic Initiative Grant and Frontiers Clinical Translational Science award helped fund the study.
Beginning in 1999, blogging became a route for individuals with a devotion to writing to share their talent. Blogging gives the author the ability to channel their thoughts in a manner that can be useful and enjoyable to readers. Nurses encounter many learning situations which may be helpful to fellow nurses. Blogs give the writer a means to share these experiences and readers a chance to learn and relate to others in a virtual setting. In nursing, blogs serve multiple purposes including engaging fellow nurses in educational opportunities, networking, providing insight into unique avenues in nursing, and burnout prevention.
This list of top nursing blogs was compiled based on Facebook likes, frequency of postings, and number of followers. Many of the following blogs are top hits when conducting online searches and can also be followed on Twitter, Pinterest, and Google+. This list has been divided into sections for the reader’s convenience: general nursing, registered nurse, nurse practitioner, nursing student, nursing career, and women’s health.
GENERAL NURSING
Confident Voices – Beth Boynton is a national speaker, professional coach, facilitator, and medical improv trainer. She writes this blog founded on respectful communication for nurses, physicians, patient advocates, and support staff to encourage safe, respectful work cultures.
Disruptive Women in Healthcare – This blog targets challenging and inspirational concepts in the current healthcare field. There are over 100 individuals that actively contribute to this blog including elected officials, healthcare workers, patient advocates, researchers, and economists.
Diversity Nursing – Diversity Nursing offers a variety of articles on all topics pertinent to nursing including health and wellness and career tips. This blog also includes a job board and a forum for open discussion amongst nurses and student nurses. Highlight:Nurses Among Most Influential People in Healthcare
ER Nurses Care – Written by emergency room nurse Leslie Block, this blog uses her passion for nursing to demonstrate caring and compassion through her posts focusing on healthy living, injury prevention, and various current trending topics in healthcare.
Living Sublime Wellness – Elizabeth Scala MSN/MBA, RN is a motivational speaker who focuses her writing on encouraging nurses to make the necessary changes in healthcare by facilitating out-of-the box critical thinking.
Not Nurse Ratched – A nurse and freelance writer, Megen Duffy blogs about all things nursing while using her humor to lighten the mood as necessary. Duffy’s blog is highly followed online and on Facebook likely due to her down to earth writing style.
Nurse Barb’s Daily Dose – Barb Dehn, RN, MS, NP is committed to deciphering convoluted health information in order to assist individuals in achieving optimal health and wellness. Nurse Barb’s Daily Dose contains articles pertaining to women’s health, parenting, caregiving, healthy living, and medical conditions.
Nursetopia – Nursetopia features timely articles on all pertinent topics in healthcare. This blog inspires nurses by highlighting and displaying the positive influence nurses have on the healthcare culture.
rtConnections – Renee Thompson is a motivational speaker and the author of “Do No Harm” Applies to nurses too! Strategies to protect and bully-proof yourself at work. Thompson gears her presentations toward clinical competence and bullying within the workplace and works to enhance effective communication within a healthy organization.
The Nursing Show -The Nursing Show is not your typical blog. It is filled with hundreds of short podcasts and easy to read articles pertaining various nursing topics geared toward nurses of all skill levels. All nurses are sure to find topics of interest in this diverse, educational blog.
REGISTERED NURSES
According to Nurse Kateri – Kateri, RN, BSN, started this blog while on a personal journey to discover herself and now uses it to detail her personal experiences as they pertain to health and happiness. This blog features narratives relating to her career in pediatrics and pediatric intensive care.
JParadisi RN’s Blog – Julianna Paradisi, RN is an accomplished artist and an oncology nurse who incorporates art into patient care. This blog focuses on the same while featuring some of her personal pieces of art as they relate to her writing.
Nurse Eye Roll – Nurse Eye Roll was established by a newly seasoned nurse wishing to provide encouragement, inspiration, support, and laughter to student nurses. Nursing school is tough and Nurse Eye Roll is there to offer tips and suggestions about navigating the path toward graduation and successful board examination.
The Nerdy Nurse – Brittany Wilson, RN, BSN is a nursing informatics nurse who prides herself by incorporating technology into healthcare in order to improve and streamline patient care. This blog is found on various lists of top nursing blogs and is highly followed on social media. For more information, see what is nursing informatics?
NURSE PRACTITIONER
Barefoot Nurse – Barefoot Nurse reviews real life experiences as they occur through the eyes of an advance practice nurse. Kelly Arashin, the author behind this blog, is unique in her profession because she is a dually board certified nurse practitioner in acute and critical care and a clinical nurse specialist.
My Strong Medicine – Sean Dent is an acute care nurse practitioner by day and weightlifter and coach by night. This blog was originally designed to share his experiences as a nurse but now it contains more commentaries on his personal life, his love for CrossFit and weightlifting.
NP Business Blog – Nurse practitioners whom are in private, independent practice are breaking the mold of traditional NP employment status and are often found without the available resources to answer common questions. Barbara C. Phillips developed this blog as a means for NPs to offer support to others in all avenues of business NPs may be involved in.
NP Odyssey – In existence since 2009, this blog contains a wealth of valuable information and insight including what it takes to become a nurse practitioner and the challenges NPs frequently encounter. This blog also incorporates articles pertaining to recent headlines in healthcare and how they pertain to NP practice.
The NP Mom -Brett Badgley Snodgross is a family nurse practitioner with a passion for pain management and palliative care. She writes informative, easy to read articles related to common concerns she sees in her practice ranging from dieting to hypertension to allergies and beyond.
NURSING STUDENT
A Journey Through Nursing School and Beyond – This blog takes the reader through the entire process of climbing the ladder through nursing education. The author began this blog as a certified nurse assistant, became a LPN, then an RN, and is currently seeking a master’s degree in nursing education. Most entries are brief and include an update on coursework although others offer valuable tips and tricks of the nursing trade.
Adrienne, Student Nurse – Adrienne, RN is passionate about the way nurses and nursing students use social media in their professional lives. Adrienne, Student Nurse is written with the goal of telling the story of being a student nurse in an effort to motivate others to accept the challenge of becoming a nurse.
Becoming a RN – Follow Amy on her journey through nursing school through her blog where she recounts her trials, tribulations, and triumphs. This blog includes insight on navigating through the various challenges presented by nursing school and inspires nursing students to prevail.
NURSING CAREER
Digital Doorway – Keith Carlson, RN utilizes his blog, Digital Doorway, to coach nurses so they may feel fulfilled in their nursing careers. One of the most well known bloggers in healthcare, Carlson blogs about career opportunities, social media in healthcare, and burnout prevention.
Innovative Nurse – Kevin Ross, RN is the ‘Innovative Nurse’ behind this blog. Ross writes about numerous areas of career nursing such as time management, salary, mobile apps, networking, and workplace happiness in the healthcare arena.
International Nurse Support – International Nurse Support provides nurses with the necessary strategies to be confident in their positions while empowering them to climb the profession’s ladder as they progress in their career. This blog is owned by Joyce Fiodembo, however guest bloggers are featured frequently.
Off the Charts – Off the Charts is the online publication of the well renowned American Journal of Nursing. While this blog lacks the personal touch many other blogs convey, Off the Charts presents up to date research data provided in an easy to read format. Various bloggers are often featured on this blog including many other bloggers in this list.
The Nursing Site Blog – Kathy Quan, RN, BNS, PHN, has been a nurse for greater than 30 years and utilizes this blog as a means to share her extensive knowledge with fellow nurses. Quan is the author of five books including The Everything New Nurse Book which helps new nurses transition from nursing school to bedside nursing.
Your Career Nursing – Tina Lanciault, RN helps her readers find their niche in nursing by writing about alternative nursing careers. Your Nursing Career contains articles related to online learning, networking, lifestyles, product reviews, and entrepreneurship.
WOMEN’S HEALTH
At Your Cervix – At Your Cervix is written by a newly graduated nurse midwife and nicely portrays the trials and tribulations a new nurse midwife may encounter in practice. The blog contains educational articles that pertain to women’s health as well as commentaries based on the situations she came across over the course of the bloggers first year in practice.
Mimi Secor – Mimi Secor is an accomplished family nurse practitioner with over 30 years experience in women’s health. Outside of her private practice, Mimi Secor is a public speaker and nurse consultant who prides herself in promoting quality care in women’s health.
'Movember' is men's health awareness month. It's a global initiative that's now gaining steam and raising millions to help find cures for men's cancers and other health issues.
Originally started by two mates in Australia more than 10 years ago, it's grown from 30 growing mustaches that first year, to more than 4 million in almost two dozen countries.
The original rules still exist, right along with the concept, spelled out by the announcer in a Movember YouTube video: "It's a reality check on your health and a responsibility to take action."
The concept is easy: Men, especially those who don't normally grow facial hair, let their mustaches grow all month long. The more peach fuzz, the better!
"Honestly, it looks terrible for the first several weeks and for some individuals it always looks terrible," says Seattle's Dr. Peter Nelson. "But the point that we get across is that you want people to ask you 'why are you doing this?' "
It's a conversation starter, to get men talking about their health, specifically prostate and testicular cancer plus mental health.
Men who join the movement are called Mo Bros and work to raise money to combat these issues.
"In general, men don't discuss their health issues," Dr. Nelson said.
Dr. Nelson is part of a locally growing team of Mo Bros called MoDawgs, plus he's a prostate cancer researcher at the Fred Hutchinson Cancer Research Center.
Last year, the Movember foundation awarded his team a $1.4 million grant to develop strategies to treat advanced prostate cancer.
"Advanced prostate cancer unfortunately is really a deadly disease in which we have no cure," Nelson said. "Once prostate cancer spread out of the prostate an into bones another sites, we can often temporize it for years by cutting off the fuel supply which is testosterone but eventually these cancers all resist."
And so he explained that his team developed several interesting targets and that they're now developing drugs to block to improve treatment.
The project is moving into the second of its 3 years of funding.
And there are many such studies being funded in the United States through the Movember movement. Each country keeps all of the money it's raised. To date, the United States has raised $559 million, since 2003, and some 770 men's health projects have been funded.
So back to that Movember YouTube video, it ends with words on the screen: "Makers, Thinkers, Growers, Doers; changing the face of men's health."
A woman's odds of having a baby with kidney and urinary tract birth defects are higher if she's obese, new research suggests.
Such defects include being born with a single kidney, having kidney swelling or enlarged ureters, the urine-carrying tubes, said lead researcher Dr. Ian Macumber, a pediatric nephrology fellow at Seattle Children's Hospital.
"The more we find out about obesity, the more we find out what a public health problem it is," he said.
Prior research has linked maternal obesity with newborn heart defects, neural tube defects such as spina bifida and other health conditions.
The discovery of a link with kidney and urinary tract birth defects is newer. "We found a significant association between maternal obesity and risk of these anomalies," said Macumber.
While the study found a link between maternal obesity and certain birth defects, it did not establish a cause-and-effect relationship.
The kinds of defects Macumber and his colleagues evaluated are diagnosed in up to 1 percent of pregnancies, with some conditions more serious than others. The defects account for about 20 percent or 30 percent of all prenatal abnormalities, he said.
And risk of these defects increased along with the level of obesity, the study found.
More than half of pregnant women in the United States are overweight or obese, and 8 percent of reproductive-aged women are extremely obese, says the American College of Obstetricians and Gynecologists.
Macumber is to present the findings Nov. 14 at a meeting of the American Society of Nephrology in Philadelphia. Studies presented at medical meetings are typically viewed as preliminary until published in a peer-reviewed journal.
For the study, the researchers looked at medical charts, including birth and hospital discharge records, from 2003 to 2012. They found more than 3,200 cases of abnormal kidney or urinary tract problems and compared them with more than 13,000 "controls" -- newborns without the abnormalities.
Looking at pre-pregnancy weight records, the researchers found that mothers who delivered children with the birth defects were almost 1.3 times more likely to be obese than those whose infants didn't have the kidney and urinary tract defects.
Obesity was based on body-mass index (BMI), a calculation based on height and weight. A BMI of 30 or greater is viewed as obese. As an example, a 5-foot-4-inch-tall woman who weighs 180 pounds has a BMI of 30.9 and is considered obese.
Because the researchers went by hospital codes, they couldn't determine which defects were most common or how severe they were.
The mechanism behind the association isn't known, Macumber said.
"There is certainly some question as to whether insulin may play a role in this," he said. Pregnant women who are overweight may have insulin resistance, a condition in which the body doesn't respond well to the hormone insulin, and blood sugar is less able to get to the cells, he said.
Another expert praised the research.
"Studies like this are really quite important," said Dr. David Mendez, an attending physician at the Miami Children's Hospital and a neonatologist. However, whether obesity actually causes these birth defects is not yet known, he added.
Mendez said that chart reading, while limited in some respects, "is a vital research tool" and a good starting point.
Ideally, future research would follow mothers during pregnancy, tracking their weight and the health of their newborns, looking at the link from the start, he said.
Meanwhile, Mendez advises a good diet, exercise if approved by the woman's doctor and other good health habits. "The things that make you feel good," he tells patients, "will make the baby feel good."
Residents of the southern United States may be at risk for a parasitic infection that can lead to severe heart disease and death, three new studies suggest.
Chagas disease, which is transmitted by "kissing bugs" that feed on the faces of humans at night, was once thought limited to Mexico, Central America and South America.
That's no longer the case, the new research shows.
"We are finding new evidence that locally acquired human transmission is occurring in Texas," said Melissa Nolan Garcia, a research associate at Baylor College of Medicine in Houston and the lead author of two of the three studies.
Garcia is concerned that the number of infected people in the United States is growing and far exceeds the U.S. Centers for Disease Control and Prevention's estimate of 300,000.
In one pilot study, her team looked at 17 blood donors in Texas who tested positive for the parasite that causes Chagas disease.
"We were surprised to find that 36 percent had evidence of being a locally acquired case," she said. "Additionally, 41 percent of this presumably healthy blood donor population had heart abnormalities consistent with Chagas cardiac disease."
The CDC, however, still believes most people with the disease in the United States were infected in Mexico, Central and South America, said Dr. Susan Montgomery, of the agency's parasitic diseases branch.
"There have been a few reports of people becoming infected with these bugs here in the United States," she said. "We don't know how often that is happening because there may be cases that are undiagnosed, since many doctors would not think to test their patients for this disease. However, we believe the risk of infection is very low."
Maybe so, but kissing bugs -- blood-sucking insects called triatomine bugs -- are found across the lower half of the United States, according to the CDC. The insects feed on animals and people at night.
The feces of infected bugs contains the parasite Trypanosoma cruzi, which can enter the body through breaks in the skin. Chagas disease can also be transmitted through blood.
It's a silent killer, Garcia said. People don't feel sick, so they don't seek care, but it causes heart disease in about 30 percent of those who get infected, she said.
In another study, Garcia's team collected 40 insects in 11 Texas counties. They found that 73 percent carried the parasite and half of those had bitten humans as well as other animals, such as dogs, rabbits and raccoons.
A third study found that most people infected with Chagas aren't treated.
For that project, Dr. Jennifer Manne-Goehler, a clinical fellow at Harvard Medical School and Beth Israel Deaconess Medical Center in Boston, collected data on nearly 2,000 people whose blood tested positive for Chagas.
Her team found that only 422 doses of medication for the infection were given by the CDC from 2007 to 2013. "This highlights an enormous treatment gap," Manne-Goehler said in a news release.
The findings of all three studies, published recently in the American Journal of Tropical Medicine and Hygiene, were to be presented Tuesday in New Orleans at the annual meeting of the American Society of Tropical Medicine and Hygiene.
Symptoms of Chagas can range from none to severe with fever, fatigue, body aches and serious cardiac and intestinal complications.
"Physicians should consider Chagas when patients have swelling and enlargement of the heart not caused by high blood pressure, diabetes or other causes, even if they do not have a history of travel," Garcia said.
However, the two treatments for this disease are "only available [in the United States] via an investigative drug protocol regulated by the CDC," Garcia said. They are not yet approved by the Food and Drug Administration.
Efforts are under way to develop other treatments for Chagas disease, Montgomery said.
"Several groups have made some exciting progress in drug development," she said, "but none have reached the point where they can be used to treat patients in regular clinical practice."
One recent night I was asked to declare the death of a woman I had never met.
“Ms. L. passed,” the nurse said. “Could you pronounce her?”
The online medical record told me that she was 32 years old, one year younger than me. She had been in the hospital for months with leukemia that had progressed despite every possible chemotherapy regimen and a failed bone marrow transplant. And now someone needed to perform a death exam.
Declaring death is not technically hard but it is weird and sad and requires reams of paperwork. It is usually done by an intern, but my intern was busy so I said I would do it.
The first time I declared a patient dead was nearly six years earlier. I had been a doctor for a few months when I was summoned overnight with a page that told me that my patient’s heart had stopped. When I got to his room I was out of breath and his nurse smiled at me and told me that there really wasn’t urgency; he wasn’t going anywhere.
It was only when I walked into the room and saw my patient still and utterly silent, his tired family sitting around the bed, that I realized no one had ever told me precisely how to declare death. I wished I could come back later, but it didn’t seem right to leave him there, so I thumbed through my pocket-sized intern survival guide. The manual was alphabetized, and the discussion about declaring death came somewhere before a section on diabetes management.
The instructions were clear and began with the directive to express sympathy. I turned to the family to tell them how sorry I was. Listen for heart sounds and watch to see if the patient is breathing. I placed my stethoscope on the patient’s still chest and waited, watching for him to take a breath, and wondering what I would do if I heard something. But there was nothing. Feel for a pulse. I placed my hand on his neck and there was not even a quiver. And that was that. He was dead.
I looked at the clock and spoke the time out loud and said I was sorry again. And then I left the room.
Later I would face the inevitable pile of paperwork, which one hospital I worked at labeled the “Final Discharge Packet,” and another, in bold letters on a red binder, the “Death Binder.” That was followed by calls to admitting to report the death, minutes that felt like hours on hold with the medical examiner, death certificates returned to me because I had signed on the wrong dotted line. By the end of my intern year, one of the worst parts of having a patient die was those bureaucratic forms and phone calls.
Now, years later, I paused outside the room of Ms. L. before pulling back the curtain.
Until then, most of the patients I had been called to declare looked much as they did in life, only vacant. But this woman had been destroyed by illness. She was bald and yellow and bloated. She must have suffered. I took out my stethoscope as I had learned to do, rested it on her chest and listened to the silence that had taken the place of her heartbeat. I laid my fingers on her neck and there was no pulse. I looked up at the clock and said the time out loud.
As I turned to leave, I couldn’t help but note the wall of cards and photographs next to her hospital bed. She must have run a marathon to raise money for cancer research, for one photo captured her healthy and smiling, arms lifted victoriously as she crossed the finish line. Someone who loved her must have been there, waiting to take that photo.
“She must have been cool,” I said to her nurse. “I bet I would have liked her.”
“She was awesome.”
No one spoke. Two nurses gently pulled out the intravenous lines that had once run antibiotics and fluids into her veins and, one by one, removed the stickers on her chest that had recorded her heartbeat. One of the nurses paused and caught my eye.
“It’s so humid out,” she said. “How do you keep your hair from getting frizzy in this humidity?” I had showered just before my shift, I told her, and then I had come right to work so I hadn’t been outside much. When I caught a glimpse of myself in the mirror, my hair didn’t even look that good.
And then, because I didn’t know what else to say in front of this 32-year-old woman I would never meet, I offered only: “You know, I’ve always wanted to run a marathon.”
Invisible tattoos could replace the permanent dark ink tattoos used to ensure that breast cancer patients having radiotherapy are treated in exactly the same spot during each session, according to results from a pilot study to be presented at the National Cancer Research Institute (NCRI) Cancer Conference.
Research suggests that the permanent pin prick marks made on the skin of women having radiotherapy reminds them of their diagnosis for years to come, reducing body confidence and self-esteem.
It's also more difficult to spot these tattoos in dark-skinned women, potentially leading to inconsistencies in the area being treated.
The NIHR-funded researchers, based at The Royal Marsden hospital in London, asked 42 breast cancer patients undergoing radiotherapy to rate how they felt about their body, before the treatment and one month later.
Half the women were offered fluorescent tattoos, only visible under UV light, while the other half had conventional dark ink tattoos.
The researchers found that 56 per cent of the women who had fluorescent tattoos felt better about their bodies one month after treatment, compared to only 14 per cent among those who received black ink tattoos.
Using fluorescent tattoos also made no difference to the accuracy of treatment and took only slightly longer to carry out, compared to conventional dark ink tattoos.
Steven Landeg, a senior radiographer from the Royal Marsden, who is presenting the data, said: "These findings suggest that offering fluorescent radiotherapy tattoos as an alternative to dark ink ones could help ameliorate the negative feelings some women feel towards their bodies after treatment. It's important to remember that body image is subjective and dark ink radiotherapy tattoos will affect patients differently, but we hope that these results will go some way towards making this a viable option for radiotherapy patients in the future."
Evelyn Weatherall, 62, Surrey, had six cycles of chemotherapy, followed by radiotherapy, after being diagnosed with breast cancer following routine mammography through the UK's breast screening programme.
She said: "I'd asked if I could be part of any kind of clinical trial during my treatment because I'd read about how successful they were proving to be. My doctors told me about the invisible tattoos they were pioneering at The Royal Marsden hospital and I was more than happy to take part. I had lost my hair during chemotherapy and felt that I didn't want another visible reminder of my cancer.
"I think I was one of the first to undergo this procedure and it really worked. There wasn't a mark on my skin after the radiotherapy planning. I was going to a wedding soon afterwards and knew I'd be able to wear an outfit that didn't make me feel self-conscious.
"It's wonderful to think that I may have been a part of something that could become standard in the future."
Professor Matt Seymour, NCRI's clinical research director said: "With more than half of all cancer patients now surviving 10 years and beyond, it's imperative that we do everything we can to reduce the long term impact of treatment on patients, including cosmetic changes."
The study was funded by the NIHR Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research (ICR).
Can we predict the future of medicine? Although designer babies and a disease-free world may or may not come to pass, you can get a glimpse of the most promising and upcoming medical innovations each year, via the Cleveland Clinic.
The clinic's Top 10 Medical Innovations list, which has been an annual undertaking since 2007, contains treatments and technologies that are expected to significantly change patient care and save lives.
To be considered, each innovation must have a good chance of being available to the public in the upcoming year, says Dr. Michael Roizen, chief wellness officer at the Cleveland Clinic and chairman of the committee that decides the list. The committee must also expect it to have a significant impact on a large part of the population.
The process starts with a panel of Cleveland Clinic physicians and scientists who submit their ideas. These suggestions, which Roizen said totaled about 700 for the 2015 list, are then narrowed down and voted on by 40 physicians in a variety of health fields.
Here's what they selected for 2015:
1. Mobile stroke unit
Videoconferencing has made its way into ambulances, specifically for treating stroke victims on the go. Hospital stroke neurologists can interpret symptoms via a broadband video link and instruct an onboard paramedic, critical care nurse and CT technologist on treatment. This new technology should improve the speed of medical care, which is important as strokes quickly damage and kill brain cells.
2. Dengue fever vaccine
The World Health Organization reports that about half of the world's population is now at risk for dengue fever, which up until now was preventable only by avoiding mosquito bites. The disease is a leading cause of death and illness in children in some countries. A new vaccine has been developed and tested, and is expected to be available in 2015.
3. Painless blood testing
For those who hate large needles, a nearly painless way to sample blood will be a welcome relief. Plus, it will be cheaper and provide faster results than today's blood test. The new technology takes blood from your fingertip, and the Cleveland Clinic reports that over 100 tests can be performed on just one drop of blood.
4. New way to lower cholesterol
New self-injectable drugs called PCSK9 inhibitors have shown to be very effective in lowering cholesterol. These drugs may prove to be helpful for people with high LDL cholesterol who don't have good results with statins. The FDA is expected to approve the first PCSK9 in 2015.
5 ways to lower cholesterol
5. Cancer drug that doesn't harm healthy tissue
Although chemotherapy can save lives, it can be hard on the body and attack healthy cells as well as cancerous ones. A welcome breakthrough in the world of cancer treatment, antibody-drug conjugates can deliver targeted treatment without damaging healthy tissue.
6. Immune booster for cancer patients
Immune checkpoint inhibitors have been shown to prevent cancer cells from "hiding" from the immune system, allowing the body to more effectively fight these abnormal cells. Combined with chemotherapy and radiation treatment, the drugs have shown significant, long-term cancer remissions for patients with metastatic melanoma, one of the most deadly forms of cancer.
7. Wireless cardiac pacemaker
Until this point, wires have been a necessary component in pacemakers. A new wireless pacemaker about the size of a vitamin can now be implanted in the heart without surgery. Its lithium-ion battery is estimated to last about seven years.
8. New medications for idiopathic pulmonary fibrosis
Idiopathic pulmonary fibrosis is a life-threatening disease that causes scarring in the lungs, leading to breathing difficulties and a shortage of oxygen in the brain and other organs. Life expectancy is only three to five years after diagnosis, but those numbers may change now that the FDA has approved two experimental drugs that slow the disease: pirfenidone and nintedanib.
9. Single-dose radiation therapy for breast cancer
The National Cancer Institute estimates that 40,000 women in the United States will die from breast cancer in 2014. The Cleveland Clinic cites multiple chemotherapy appointments, sometimes requiring the patient to travel long distances, as a hindrance to successful treatment. Intraoperative radiation therapy is a new solution. It treats a breast cancer tumor during surgery in a single dose, reducing time and cost spent on treatment.
10. New drug for heart failure
About 5.1 million people in the United States suffer from heart failure, according to the National Heart, Lung and Blood Institute. It is managed with a combination of drugs, but a new drug, angiotensin-receptor neprilysin inhibitor, has been granted fast-track status by the FDA because of its ability to cut the risk of dying from heart failure more effectively than current treatments.
For more information on the annual medical innovations list, including descriptions and videos, download the "Innovations" app or visit the website. A "where is it now" feature also includes updates on innovations that made the top 10 list in prior years.
"We look in past to see what we voted on to improve the process," Roizen said. "With one exception, we've been pretty good."
Brittany Maynard, the Oregon woman who had become an outspoken advocate for patients' rights following her terminal cancer diagnosis, died on Saturday, the Oregonian reported. She was 29.
"Goodbye to all my dear friends and family that I love," she wrote in a Facebook post, according to People. "Today is the day I have chosen to pass away with dignity in the face of my terminal illness... the world is a beautiful place, travel has been my greatest teacher, my close friends and folks are the greatest givers... goodbye world. Spread good energy. Pay it forward!"
Earlier this year, Maynard learned that she was suffering from an aggressive form of brain cancer called glioblastoma and had only six months to live. After hearing what the disease would to her body in its final stages, she decided that she wanted to die on her own terms.
Maynard and her family, including her husband Dan Diaz and her mother Debbie Ziegler, moved to Oregon,whose Death With Dignity Act has allowed hundreds of terminally ill people to end their lives by taking a medication prescribed by doctors. She picked November 1st as the day she wanted to die because it was after her husband's late October birthday.
Since then, Maynard had become a champion for the law and for patients in her situation, working with the group Compassion and Choices.
"I am not suicidal," she wrote in a blog post for CNN.com. "I do not want to die. But I am dying. And I want to die on my own terms."
On Wednesday, Maynard released a new video that suggested that she might consider postponing her death.
"If November 2nd comes along and I've passed, I hope my family is still proud of me and the choices I've made. If November 2nd comes along and I'm still alive, I know that we'll still be moving forward as a family out of love for each other, and that decision will come later."
Maynard recently crossed the last item off her bucket list: a trip to the Grand Canyon. Before she became ill, Maynard was an active traveler and adventurer who lived in Southwest Asia for a year and once climbed Mount Kilimanjaro.
Detecting cancer could be as easy as popping a pill in the near future. Google’s head of life sciences, Andrew Conrad, took to the stage at the Wall Street Journal Digital conference to reveal that the tech giant’s secretive Google[x] lab has been working on a wearable device that couples with nanotechnology to detect disease within the body.
“We’re passionate about switching from reactive to proactive and we’re trying to provide the tools that make that feasible,” explained Conrad. This is a third project in a series of health initiatives for Google[x]. The team has already developed a smart contact lens that detects glucose levels for diabetics and utensils that help manage hand tremors in Parkinson’s patients.
The plan is to test whether tiny particles coated “magnetized” with antibodies can catch disease in its nascent stages. The tiny particles are essentially programmed to spread throughout the body via pill and then latch on to the abnormal cells. The wearable device then “calls” the nanoparticles back to ask them what’s going on with the body and to find out if the person who swallowed the pill has cancer or other diseases.
“Think of it as sort of like a mini self-driving car,” Conrad simplified with a clear reference to Google[x]‘s vehicular project. “We can make it park where we want it to.” Conrad went on with the car theme, saying the body is more important than a car and comparing our present healthcare system as something that basically only tries to change our oil after we’ve broken down. “We wouldn’t do that with a car,” he added.
Bikanta’s tiny diamonds luminesce cells in the body.
Similar to Y Combinator-backed Bikanta, the cells can also fluoresce with certain materials within the nanoparticles, helping cancer cells to show up on an MRI scan much earlier than has been possible before.
This has all sorts of implications in medicine. According to a separately released statement from Google today, “Maybe there could be a test for the enzymes given off by arterial plaques that are about to rupture and cause a heart attack or stroke. Perhaps someone could develop a diagnostic for post-surgery or post-chemo cancer patients – that’s a lot of anxious people right there (note: we’d leave this ‘product development’ work to companies we’d license the tech to; they’d develop specific diagnostics and test them for efficacy and safety in clinical trials.”
We essentially wouldn’t need to go into the doctor and give urine and blood samples anymore. According to Conrad, we’d simply swallow a pill and monitor for disease on a daily basis. We’d also be able to upload that data into the cloud and send it to our doctor. “So your doctor could say well for 312 days of this year everything looks good but these past couple of months we’re detecting disease,” Conrad said.
Privacy and security, particularly in health care is essential. Google came under fire in the last couple of years for handing over information to the U.S. government. Conrad was quick to mention that a partner, not Google would be handling individual data. “It’d be like saying GE is in control of your x-ray. We are the creators of the tech and they are the disseminators,” Conrad clarified.
The U.S. government has an active interest in this space, as well. It’s invested over $20 billion in nanotechnology research since 2013.
This project is in the exploratory phases but Conrad was hopeful that we’d be seeing this technology in the hands of every doctor within the next decade. He also mentioned that his team has explored ways of not just detecting abnormal cells but also delivering medicine at the same time. “That’s certainly been discussed,” he said, but cautioned that this was something that needed to be carefully developed so that the nanoparticles had a chance to show what was happening in the body before destroying the cells.
So far 100 Google employees with expertise in astrophysics, chemistry and electrical engineering have taken part in the nanoparticle project. “We’re trying to stave off death by preventing disease. Our foe is unnecessary death,” Conrad added.
When Jackson Small began having seizures at 7, his parents hoped and assumed at least one of the many epilepsy drugs on the market would be enough to get things under control. But one seizure quickly spiraled to as many as 30 a day.
"He would stop in his tracks and not be aware of what was going on for 20 or 30 seconds or so," his mother Shana Small told CBS News. Jackson was eventually diagnosed with juvenile myoclonic epilepsy, a type of epilepsy characterized by brief but often frequent muscle jerking or twitching.
But a number of medications typically prescribed to patients with this type of epilepsy were not effective. And so the quest to help Jackson gain control over his seizures led the family from their home in Orlando, Florida, to the office of a registered dietician at the NYU Langone Comprehensive Epilepsy Center in New York City.
They were there to discuss the medical benefits of heavy cream, mayonnaise, eggs, sausage, bacon and butter.
A lot of butter.
The plan was to treat Jackson with a diet that is heavy in fat, low in protein and includes almost no carbohydrates. It's known as the ketogenic diet and has long been in the arsenal of last-resort options for patients with epilepsy who are unresponsive to medication. Doctors may recommend a patient go on this special diet after unsuccessfully trying two or three prescriptions.
The diet works by putting the body in a "fasting" state, known as ketosis. "When we're fasting the body needs to find fuel so our body will break down fat storage and break down their own fat and enter a state of ketosis," Courtney Glick, the registered dietician who coordinated and fine-tuned Jackson's diet plan, told CBS News. "But with this diet, instead of breaking down the body's fat, the body breaks down dietary fat."
The ketogenic diet consists of as much as 90 percent fat. Some patients who feel they can't make such an extreme change adopt a modified Atkins diet, which is between 65 and 70 percent fat. It can be nearly as effective for controlling seizures, though every patient is different.
Though experts don't know everything about why this diet is effective for seizure control, they do know that eating mostly fat causes the body to fuel on ketones rather than glucose, which ultimately lowers insulin levels. This can have an anti-inflammatory effect on the body and may prevent seizures by calming the brain, said Glick.
One study by researchers at Dana-Farber Cancer Institute and Harvard Medical School found that a child's ability to stave off seizures is tied to a protein that affects metabolism in the brain. The protein, called BCL-2-associated Agonist of Cell Death, or BAD, also regulates metabolism of glucose. The researchers discovered that by modifying this, they switched metabolism in brain cells from glucose to ketone bodies, which are fat byproducts.
Glick said the diet plan didn't work for Jackson until he tried the most strict version, which was a 4 to 1 ratio of fat to protein and carbohydrates. Each day, he ate approximately 160 grams of fat, 8 to 10 grams of carbohydrates and 30 grams of protein, all of which amounted to about 1,700 calories a day.
Four months into the program, Jackson was seizure-free. He remained on the strict diet for two years with no return of seizures. His mother prepared foods from special recipes such as "keto" pizza made with a macadamia nut crust or chicken nuggets with coconut flour.
Over the summer -- after receiving a green light from his doctors -- Jackson, now 10 years old, began to wean himself off the diet, and his mother has slowly introduced foods such as breads and ice cream. He has maintained seizure-free and takes very little anti-seizure medication.
Research has found that for pediatric patients the anti-seizure effects of the diet often continue long after the child stops following the food plan, though the reason why remains unclear. This is typically not the case for adults, who may need to stay on the diet for life in order to control seizures.
"We've probably seen more kids go on the diets than adults, and adults are really set on their eating patterns," said Glick, adding that social obligations can make the diet difficult to fit into a grown person's lifestyle.
Jackson's mother said his doctors are hopeful that in the near future he may no longer need medication -- or a keto diet -- to stay seizure-free. "I think it's taught him a very important lesson about how food is as important as medicine, and how food affects the chemistry of your body," she said.
A new report finds that by 2100, there will be more people alive on the planet than has ever previously been predicted. We investigate what the consequences these extra bodies may have for maintaining public health.
The potentially catastrophic consequences of an exponentially growing global population is a favorite subject for writers of dystopian fiction.
The most recent example, Utopia - a forthcoming David Fincher-directed series for HBO - won critical acclaim in its original incarnation on UK television for its depiction of a conspiracy-laden modern world where the real threat to public health is not Ebola or other headline-friendly communicable viruses, but overpopulation.
Fears over the ever-expanding number of human bodies on our planet are not new and have been debated by researchers and policy makers for decades, if not centuries. However, recent research by University of Washington demographer Prof. Adrian Raftery - using modern statistical modeling and the latest data on population, fertility and mortality - has found that previous projections on population growth may have been conservative.
"Our new projections are probabilistic, and we find that there will probably be between 9.6 and 12.3 billion people in 2100," Prof. Raftery told Medical News Today. "This projection is based on a statistical model that uses all available past data on fertility and mortality from all countries in a systematic way, unlike previous projections that were based on expert assumptions."
Prof. Raftery's figure places up to an additional 5 billion people more on the Earth by 2100 than have been previously calculated.
A key finding of the study is that the fertility rate in Africa is declining much more slowly than has been previously estimated, which Prof. Raftery tells us "has major long-term implications for population."
Fertility rates declining more slowly in Africa than previously reported
A 2003 Centers for Disease Control and Prevention (CDC) report found that, in sub-Saharan Africa, both fertility and mortality rates were high, with the proportion of people aged over 65 expected to remain small, increasing from an estimated 2.9% in 2000 to 3.7% in 2030.
The CDC report notes that fertility rates declined in developing countries during the preceding 30 years, following a 20th century trend among developed countries. The pattern established by developed countries - and presumed to follow in developing countries - was that countries shift from high fertility and high mortality rates to low fertility and delayed mortality.
This transition starts with declining infant and childhood mortality as a result of improved public health measures. Improvements in infant and childhood mortality contribute to longer life expectancy and a younger population.
This trend of adults living longer, healthier lives is typically followed by a decline in fertility rates. The CDC report suggested that by 2030, there would be similar proportions of younger and older people in developing countries, by that point mirroring the age distribution in developed countries circa 1990.
Prof. Raftery's research, however, notes that in Nigeria - Africa's most populous country - each woman has an average of six children, and in the last 5 years, the child mortality rate has fallen from 136 per 1,000 live births to 117. This works out as a population increase of 20 people per square mile over the same timespan.
How will population growth affect developing countries?
But what does this mean for countries where the public health system is already stretched to breaking point - as has been demonstrated by the recent Ebola epidemic?
"Rapid population growth is likely to increase the burden on the public health service proportionally," answered Prof. Raftery.
"There are already big public health needs and challenges in high-fertility countries, and rapid population growth will make it even harder to meet them." However, if the fertility rate declines faster, Prof. Raftery suggests that high-fertility countries can reap "a demographic dividend."
He explained:
"This is a period of about a generation during which the number of dependents (children and old people) is small. This frees up resources for public health, education, infrastructure and environmental protection, and can make it easier for the economy to grow. This can happen even while the population is still increasing."
Does this suggest that an increasing population is not quite as much of a threat, but that it is more specifically the accelerations and decelerations in fertility rates that provide warning signs to future public health crises?
"Following a long run of an increasing human population growth rate, over the past half century the rate has been halved from about 2% to about 1%," Darryl Holman, professor of biological anthropology at the University of Washington, explained to MNT.
"The turnaround is quite remarkable," he said. "But as long as the growth rate remains positive, our species will eventually reach numbers and densities where technological solutions cannot ameliorate resource scarcity."
High population density leads to a much higher rate of contact between humans, which means that communicable diseases - ranging from the common cold to Dengue fever - can be much more easily transmitted.
And more people means greater efforts are needed to control waste management and provide clean water. If these needs cannot be adequately met, then diarrheal diseases become much more common, resulting in what Prof. Holman described to the University of Washington's news website The Daily UW as a "huge, huge, huge difference in mortality rates."
Taking a more general view, "the anticipated increase in the number of older persons will have dramatic consequences for public health, the health care financing and delivery systems, informal caregiving, and pension systems," wrote the authors of the CDC's 2003 report.
Overpopulation and the environment
"Can we assume that life on earth as we know it can continue no matter what the environmental conditions?," asked the authors of a 2001 Johns Hopkins School of Public Health report on the health consequences of population growth.
The Johns Hopkins report quoted figures demonstrating that unclean water and poor sanitation kill over 12 million people every year, while air pollution kills 3 million. In 64 of 105 developing countries, population has grown faster than food supplies.
By 2025, the report claimed, humankind could be using over 90% of all available freshwater, leaving just 10% for the world's plants and animals.
Prof. Holman summarizes the writings of experts Joel Cohen, E.O. Wilson, Paul Ehrlich and Ronald Lee, who have argued that the consequences of long-term environmental degradation - "specifically rising sea levels, disruption of agriculture and the increased frequency of extreme weather events resulting from anthropogenic climate change, exacerbated by resource scarcity" - create social problems that lead to social unrest.
With more people living together than ever before, it seems inevitable that this compounded social unrest would lead to increased warfare and fighting for resources.
According to the Johns Hopkins researchers, about half of the world's population currently occupies a coastal strip 200 kilometers wide - which means that 50% of us are squeezed together on just 10% of the world's land surface.
The projected flooding of these coastal regions as a result of global warming and rising sea levels could displace millions of people, result in widespread droughts and disrupt agriculture.
The Johns Hopkins team identified two main courses of action to divert these potential disasters.
Firstly - sustainable development. The report authors argued this should include:
More efficient use of energy
Managing cities better
Phasing out subsidies that encourage waste
Managing water resources and protecting freshwater sources
Harvesting forest products rather than destroying forests
Preserving arable land and increasing food production
Managing coastal zones and ocean fisheries
Protecting biodiversity hotspots.
The second vital area of action is the stabilization of population through good-quality family planning, which "would buy time to protect natural resources."
How to reduce fertility in a morally acceptable way?
Commenting on Prof. Raftery's finding that we may be welcoming an additional 5 billion individuals onto the planet by 2100 than had previously been estimated - a potential global population of 12.3 billion people - Prof. Holman admits that "it is difficult to know what the public health effects will be."
He explains:
"By then, we may see severe petroleum and fresh water resource shortages, climate changes that affect agriculture patterns that, in turn, affect food supplies. Reducing fertility in socially and morally acceptable ways seems like one public health strategy to avoid - or at least postpone - testing some of these limits."
In Utopia, a sinister governmental organization proposes to sterilize a large percentage of the population by rolling out a secretly modified vaccine in response to a manufactured flu pandemic. Obviously, that is not a socially or morally acceptable strategy for reducing fertility - but what is?
Experts consider boosting the education of girls in developing countries to be a prime solution.
As well as acquiring more control over their reproductive life, an educated female workforce should have more opportunities of employment and of earning a living wage. Studies report that the children of educated women also have better chances of survival and will become educated themselves. This pattern continuing across generations is associated with a decline in fertility rates.
A 2011 article by the Earth Policy Institute (EPI), analyzing data from the United Nations (UN), states that "countries in which more children are enrolled in school - even at the primary level - tend to have strikingly lower fertility rates."
In particular:
"Female education is especially important. Research consistently shows that women who are empowered through education tend to have fewer children and have them later. If and when they do become mothers, they tend to be healthier and raise healthier children, who then also stay in school longer. They earn more money with which to support their families, and contribute more to their communities' economic growth. Indeed, educating girls can transform whole communities."
The relationship between education, fertility and national poverty is a direct one. As the EPI authors add: "When mortality rates decline quickly but fertility rates fail to follow, countries can find it harder to reduce poverty."
The UN's 2012 Revision of the world population prospects report suggested if we make rapid reductions in family size, then it may still be possible to constrain the global population to 8 billion by 2045.
No projections are set in stone - all are contingent on what extent fertility rates will sway over the next century. And, as Prof. Holman pointed out to us, the nature of the threat posed by overpopulation has "been vigorously debated for over 200 years" with experts still not in complete accord.
For instance, in the 1980s, said Prof. Holman, the economist Julian Simon and ecologist Paul Ehrlich went on tour together, with a series of debates about the consequences of population growth.
"Ehrlich argued that continued population growth would lead to disaster for humans. Simon argued that population growth provided more people to invent new solutions to the problems confronting humans," said Prof. Holman, adding:
"Given the trends to this point, Simon has been 'more right.' One simple measure of this is mortality rates, which have decreased for most human groups. The flaw in Simon's argument may well be that we have never hit the limits of our finite earth. Positive population growth guarantees that we will, someday, hit some hard limits."
"So that," Prof. Holman concluded, "is the long term."
October's shorter, darker days can trigger a type of depression, known as seasonal affective disorder, according to an expert.
People affected by seasonal affective disorder, also called SAD, may feel overly tired, lack motivation and even have trouble getting out of bed. In extreme cases, SAD can lead to suicide, said Dr. Angelos Halaris, a professor in the department of psychiatry and behavioral neurosciences at Loyola University Chicago Stitch School of Medicine.
"Seasonal affective disorder should not be taken lightly," Halaris said in a hospital news release.
Seasonal affective disorder affects up to 5 percent of the population, Halaris said. It's linked to a reduction in light exposure from shorter days and gray skies, which is thought to cause a chemical imbalance in the brain.
SAD season starts in October and lasts until the middle of April. Until then, there are ways to reduce your risk for the condition, advised Halaris. He said the following strategies might help:
Get outside. Spend at least 30 minutes a day outside. Avoid wearing sunglasses during this period of time. If weather permits, expose the skin on your arms to the sun.
Let light inside. Keep your home well-lit. Open curtain and blinds to allow sunlight in. You can also consider buying a high-intensity light box specially designed for SAD therapy. Sit near the box for 30 to 45 minutes in the morning and at night. Be sure to talk to your doctor before attempting this type of light therapy on your own, Halaris cautioned.
Exercise. Physical activity releases endorphins and other brain chemicals that help you feel better and gain more energy, Halaris explained. Exercising for 30 minutes daily can help.
Consider medication. When all else fails, there are medications that can help ease the troubling effects of SAD. Halaris recommends visiting a mental health professional if extra sun exposure, indoor lights and exercise are not effective in treating your symptoms.
A special type of concentrated cocoa drink seems to turn back the clock on memory, changing the brain and helping middle-aged people ace memory tests, researchers reported on Sunday.
Plant compounds called flavanols seem to be what does the trick, the team at Columbia University Medical Center report in the journal Nature Neuroscience.
"If a participant had the memory of a typical 60-year-old at the beginning of the study, after three months that person on average had the memory of a typical 30- or 40-year-old," said Dr. Scott Small, who led the study.
It wasn’t hot cocoa that they drank, he cautions, but a proprietary drink made by Mars, Inc., which has also demonstrated that its flavanol-rich compounds can improve heart health.
It is not yet available on the market.
Small’s team tested 37 healthy volunteers aged 50 to 69, who either drank a high-flavanol diet (900 mg of flavanols a day) or a low-flavanol diet (10 mg of flavanols a day) for three months. Everyone got functional magnetic resonance imaging (fMRI) scans and also memory tests at the beginning and after the three months.
"When we imaged our research subjects' brains, we found noticeable improvements in the function of the dentate gyrus in those who consumed the high-cocoa-flavanol drink," said Adam Brickman, an associate professor of neuropsychology who worked on the study.
“High cocoa flavanols cause an improvement in the area of the brain that’s affected by aging,” Small said.
“This very small trial highlights some possible effects of flavanols found in cocoa beans over a short time period, but we’d need to see much longer, large-scale studies to fully understand whether a diet high in these flavanols could boost cognition in old age,” said Dr. Simon Ridley, Head of Research at Alzheimer’s Research UK.
“We also don’t know how meaningful the improvements measured in the tests used here would be for people in their daily lives. This study didn’t look at dementia, and we can’t know from this research whether a diet high in cocoa would have any effect in either preventing or delaying the onset of the condition.”
And Small cautioned against using the findings to justify loading up on chocolate.
“It is true that cocoa flavanols are found in chocolate; however, only in small amounts,” he said. “Consuming a lot of chocolate is simply bad for your health.”
When Paula Radcliffe won the New York City Marathon in 2007, nine months after giving birth to a daughter, Isla, Radcliffe was considered an anomaly. Her intense training through her pregnancy, which included twice-a-day sessions and grueling hill workouts, was scrutinized and criticized.
Seven years later, maintaining a top running career and a family has become relatively common. About a third of the women in the professional field of 31 for the New York City Marathon next Sunday have children.
“I watched Paula win New York, basically leading from the starting gun to the finish tape, and afterward she picked up her baby,” said Kara Goucher, a top American marathoner. “I realized I can do both. And I want to do both.”
Goucher, 36, finished third in the 2008 New York City Marathon, and this year she will run the New York race for the first time with her 4-year-old son, Colt, cheering her on.
When she contemplated having a child, Goucher engaged in the careful strategizing common to elite female athletes, who consider precisely when to become pregnant so as not to risk missing out on an Olympic medal or sacrificing a corporate sponsorship.
Elite female distance runners now run competitive times well into their late 30s. The average age of a top female marathoner is 30, and 19 women in next Sunday’s professional field are that age or older.
As athletic peaks for these top runners have overtaken fertility peaks, the decision to combine motherhood and training has become increasingly unavoidable. Competitive careers are stretching: The American Deena Kastor, expected to be another top finisher next Sunday, is 41.
“I always wanted to have a child,” Goucher said, “and I didn’t want to wait until I was done, because I don’t really see an end date on my career. I wanted more in my life than just running. But the details of how you do that can get incredibly complicated.”
Elite runners often try to squeeze in a pregnancy and recovery in the 16-month window between world track championships in years with no Summer Olympics. This is one such year, and pregnancies abound.
Maternity leave in professional running is rare. A pregnancy is still frequently treated as if it were an injury, and women can experience a pay cut or not be paid at all if they do not compete for six months. During that period, they often remain bound to sponsors in exclusive contracts that can last upward of six years. Because the athletes are independent contractors, they are not covered by laws that protect employed women in pregnancy.
Lauren Fleshman, an N.C.A.A. 5,000-meter champion and a professional runner, switched to a women’s-oriented sponsor, the running apparel company Oiselle, before having a son in June 2013.
Referring to Goucher and Radcliffe, Fleshman said: “Kara and Paula showed that pregnancy doesn’t necessarily need to be an impediment to the athletic part of our careers, and blew up the vestiges of the myth of the ‘fragile woman’ who can’t be both a top athlete and a mother. But in terms of your career, there’s still the feeling that if you say you want to have a kid, you’re saying you don’t want to be an athlete.”
It does not help that so many people seem to have an opinion on the matter. After Alysia Montaño, a 2012 Olympian, ran an 800-meter race in June during her eighth month of pregnancy, her decision became the subject of intense public scrutiny.
“I wanted to help clear up the stigma around women exercising during pregnancy, which baffled me,” Montaño said. “People sometimes act like being pregnant is a nine-month death sentence, like you should lie in bed all day. I wanted to be an example for women starting a family while continuing a career, whatever that might be. I was still surprised by how many people paid attention.”
Montaño’s daughter was born in August.
“Giving birth is a very athletic activity, like going through intervals on the track,” Montaño said. “Like contractions, intervals can start out easy and progress as they get harder. There’s sometimes a point where you wonder, ‘Can I do one more set?’ But you know you’re going to make it. And then you kick to the finish.”
Other women have chosen different paths.
Clara Horowitz Peterson, a former top runner at Duke, focused on starting a family in her mid-20s, aiming for a racing peak afterward. Now 30, she is pregnant with her fourth child.
“I think if I’d chosen to train at altitude and log 120-mile weeks, I could have made it to the Olympics,” said Peterson, who typically runs 80 to 90 miles a week when not pregnant. “But that comes with sacrifices; you put your career first, and before you know it, you’re 28, maybe confronting fertility issues. I always felt like having children was more important to me than a running career.”
Still, Peterson ran right up until the births of her first three children. She qualified for the 2012 United States Olympic marathon trials just four months after delivering her second child, and she logged a 2-hour-35-minute time at the race four months later.
“I trained hard through that pregnancy,” Peterson said. “You can tell when you’re pushing it. You get twingy, or feel tendons pulling, so I backed off when that happened.”
To bounce back for the trials, Peterson said, she breast-fed her second child for only five weeks — finding that the hormones related to breast-feeding made her feel sluggish — and dropped the 20 pounds she typically gained during pregnancy in eight weeks without dieting. (She breast-fed her third child for six months.)
The understanding of women’s physical resilience during and after pregnancy has also developed in recent years.
“We still don’t have good science to guide us,” said Dr. Aaron Baggish, associate director of the cardiovascular performance program at Massachusetts General Hospital in Boston, which counsels elite athletes through pregnancy. “But unequivocally I think women should exercise through pregnancy, both for their baby and their own health. The body has evolved that way. Your baseline fitness level is the best guideline: Elite athletes start out with a higher threshold, so they can do more.”
After athletes give birth, efforts to get back into shape are consuming, coupled with the usual adjustments to caring for an infant. Breast-feeding interrupts the sleep that heals spent muscles and restores energy to a tired body. Babies are often kept out of group day care to prevent them from bringing home illnesses that could compromise rigid training plans.
Pregnancy can be hard to combine with any job. As in other fields, partners are generally a key component of elite athletes’ ability to continue their careers after having children.
Edna Kiplagat, a 35-year-old Kenyan who is among the favorites in next Sunday’s race, had two children before becoming a two-time marathon world champion and the 2010 winner in New York.
Her husband and coach, Gilbert Koech, gave up his running career to focus on hers and manage their family, making breakfast for their five children, three of whom are adopted, and taking them to school while Kiplagat trains.
Goucher’s husband, Adam, retired from professional racing a year after their son’s birth and started a running-related business. He tries to balance supporting her racing career with managing his new one, saying that he and Kara work to share equally in caring for Colt.
“Kara’s putting her body through a lot right now,” her husband said, “and we need to do everything possible to alleviate the stress of training. When she needs to go out and run, or needs to rest and recover, that’s my first priority.”
Goucher said she was taking the trade-offs in stride.
“It’s scary because the fact is for all women when you have a child, you do need to drop out for a long time, and you don’t know how you’ll come back,” she said. “It’s a huge risk. Of course, I’m serious about my job, but in life I needed to be more than that. So I think it was worth it.”
Anyone who has spent much time in Minnesota's "Med City" can't help but notice that wheelchairs are everywhere.
From city parking ramps and downtown sidewalks to park trails and the local mall, the chairs have an inescapable presence.
More than likely that has do to with the fact that Rochester is home to Mayo Clinic, visited by thousands of patients every day. Many of them use wheelchairs to get around. So it's not surprising that they exist in big numbers.
The big curiosity is how they end up all over the city with their users nowhere in sight — a fact that some local residents can be oblivious to.
Denny and Carol Scanlan say empty wheelchairs are just part of the Rochester landscape.
"I never even thought of it until just now," Denny Scanlan says over a drink at American Legion Post 92, where he is a member. "Well, I see them kind of everywhere we go, I guess — where you least expect them."
"Yes," says his wife, with a laugh. "At the mall. In a restaurant. " She adds, "We're so used to it that I don't even notice it."
But some people do notice the big blue chairs.
At the Blue Water Salon on the skyway level of the Doubletree Hotel, owner Shelly Joseph often sees them just outside her door, in a public stairwell largely used by hotel staff.
"I don't know why they're in here, but randomly they're in this stairwell," she says. "It's a fire exit, basically."
At the Starbucks across the hall, manager Dawn Lee-Britt sees wheelchairs outside the employee entrance at the back of the coffee shop at least a couple of times a week.
"Sometimes we can't get out," she says. "I'm getting used to it because we see them so often." She adds: "It's like they don't need it anymore or it's time to go.
Mayo Clinic has 1,180 wheelchairs in its Rochester fleet, largely for patient transport. It loses up to 150 chairs each year, says general services manager Ralph Marquez, who oversees patient equipment.
At $550 each, that could be as much as $82,500 a year.
"Yes, it's a financial burden to us from that standpoint, but it's also a service we provide," Marquez says. "And if the patient, you know, truly comes first, sometimes that's the expense of the business."
Because the clinic does not want to keep patients from leaving the campus, the clinic's courier service rounds up wheelchairs weekly, mostly from hotels and other places that alert them.
But the chairs can travel much farther than that.
"We've gotten calls from Orlando Airport. Goodwill up in Duluth had one of our chairs and luckily we were able to retrieve that one. We've had them in Denver, out east in a few airports," Marquez says. "They get back to us dirty and needing to be cleaned. People may take them home for a while. They wind up everywhere."
That includes the Rochester Public Library, where communications manager John Hunziker considers wheelchairs normal.
"I'm sure if you aren't used to Rochester, seeing somebody going down the skyway, you know, pushing an IV on a rolling stand looks kind of weird," he says. "But it's just part of living in Rochester."
And on some days, part of Hunziker's job is to let the Mayo Clinic know there's a blue chair to pick up in the lobby.
With the Ebola outbreak dominating the national discourse, parents and caregivers are inevitably going to be confronted with the necessity of explaining the deadly and exotic disease to children.
One Connecticut company was already poised to help in that process, and it has seen a dramatic spike in sales as a result.
Giantmicrobes Inc. was founded about a decade ago with the intention of creating stuffed toys based on the actual microscopic images of various microbes as an educational tool for caregivers and young children, said Laura Sullivan, vice president of operations, in an interview with CBS News.
"It started with the common cold and similar things," Sullivan said. "It was marketed to pediatricians and parents initially. The idea is that kids respond favorably to stuffed animals."
The thinking is that children would be better able to understand what is happening in their body if they could see a softer, cuddlier version of it, Sullivan said.
Before long, the company's offerings expanded to a number of different of viruses and diseases, and the audience expanded with it.
About five years ago, the company began offering plush toys whose design was based on the microscopic image of the Ebola virus. Now, they are struggling to keep up with demand, Sullivan said.
While she declined to give specific sales figures for the Ebola plush toys, Sullivan said: "They're selling like hot cakes. We're out of stock again."
They have ramped up production with their Chinese manufacturers and are rushing to feed the demand, Sullivan said.
Their Ebola products - which include regular- and giant-sized plush recreations of the virus, as well a petri dish and something called "Primordial Putty" - are currently only available through the company's website, but much of the rest of their line can be found in everything from hospital gift shops to college bookstores to medical supply stores.
Sullivan said this isn't the first case of a headline-making disease affecting their sales. The swine flu outbreak a few years ago caused a similar spike in sales, but Sullivan added it was not quite at the level of Ebola.
"It's a neat little product," Sullivan said. "In the case of Ebola, it's been a helpful way for families talk about it and take some of the scariness away."
Cesarean delivery was the most common inpatient surgery in the United States in 2011 and was used in nearly one-third of all deliveries, research shows.
The new study found that 1.3 million babies were delivered by cesarean section in 2011. The findings also revealed wide variations in C-section rates at hospitals across the United States, but the reasons for such differences are unclear.
"We found that the variability in hospital cesarean rates was not driven by differences in maternal diagnoses or pregnancy complexity. This means there was significantly higher variation in hospital rates than would be expected based on women's health conditions," lead author Katy Kozhimannil, an assistant professor in the School of Public Health at the University of Minnesota, said in a university news release.
The researchers analyzed data from more than 1,300 hospitals in 46 states. They found that the overall rate of C-section was about 33 percent. Between hospitals, however, that rate ranged between 19 and 48 percent, according to the study.
For women who'd never previously had a C-section, the overall C-section rate was 22 percent. Depending on the hospital, that rate ranged between 11 percent and 36 percent, the researchers said.
C-section rates ranged from 8 percent to 32 percent among lower-risk women and from 56 percent to 92 percent among higher-risk women, according to the study published Oct. 21 in the journal PLoS Medicine.
The findings highlight the roles that hospitals' policies, practices and culture may have in influencing C-section rates, the study authors concluded.
"Women deserve evidence-based, consistent, high-quality maternity care, regardless of the hospital where they give birth, and these results indicate that we have a long way to go toward reaching this goal in the U.S.," Kozhimannil said in the news release.
For children with food allergies, Halloween usually means they receive far fewer treats than their friends. But this year, their luck may improve if they can spot a teal pumpkin by the doors where they trick-or-treat.
That’s because a new campaign from the Food Allergy Research & Education (FARE), Teal Pumpkin Project, aims to make Halloween safe for everyone.
“Food allergies are potentially life-threatening. When we are looking at a Halloween celebration, it is really nice to provide something that is safe,” says Veronica LaFemina, spokeswoman for FARE.
LaFemina says that one in 13 children in the United States has a food allergy.
“The Teal Pumpkin Project encourages people to raise awareness of food allergies by providing non-food treats and painting a pumpkin teal … [which] indicates that house has non-food treats,” she says. Teal is the color for food-allergen awareness.
FARE recommends that families hand out stickers, glow-sticks, vampire teeth, bouncy balls, or spider rings instead of candy, which frequently contain allergens.
“What people don’t understand or realize is that the small candy bars that people pass out for Halloween are manufactured differently,” says Beth Demis, whose 4- year-old son Luke is allergic to tree nuts and coconut. “A regular Hershey bar is okay but a smaller one [is not].”
Demis says she learns this kind of information by being a vigilant label reader and participating in groups where people share information about allergens. But people unfamiliar with food allergies often don’t realize that smaller versions of safe candy are dangerous.
While most parents of children with allergies provide a plan to their children, trick-or-treating remains a chore. FARE recommends that parents fill out an emergency plan with the help of their allergists and make sure they carry all the needed gear, including epinephrine autoinjectors (also known as EpiPens).
“For Halloween time, they are just like other kids and want to dress up and participate,” says LaFemina. “It can be tough when you have to say ‘no thank you’ and trade away most of your candy because it’s not safe.”
Demis, who lives in Cincinnati, says that her three children abide by a long-standing rule: No one can eat any candy until mom or dad examines it. Luke can swap with his brothers for candy that is safe and it is placed in his own plastic baggie. He knows he can’t touch his brothers’ candy.
Katherine Eagerton’s 3-year-old son, Caden, is allergic to soy, milk, strawberries, and tomatoes. He knows he should stay away from food that’s red, but he doesn’t quite understand what having a food allergy means. She’s excited that the Teal Pumpkin Project encourages non-food treats so that her son can enjoy Halloween like other children.
“I’m excited to see that it’s actually catching on,” says Eagerton, who lives outside of Baton Rouge, Louisiana. She’s using Facebook to encourage others in the state to offer non-food items this Halloween.
LaFemina says that 4.5 million people viewed the campaign’s first two posts and they have been shared 44,000 times.
Eagerton says that helping kids with food allergies feel included at Halloween will have a tremendous impact.
“These little treats will make such a big difference,” she says.
The trickiest part, explains Ryan Hait Campbell, is the interview. “You’re not required to tell an employer you’re deaf until the interview, but sometimes, they’re a little shocked,” says Campbell, who has been deaf since birth. “They don’t know how to handle it.”
Because of things like this, he says, unemployment rates are staggeringly high among the deaf. Hard numbers are tough to come by, but some figures estimate that around half of people with hearing disabilities are unemployed.
But Campbell wants to change this. He’s the co-founder and CEO of MotionSavvy, an Alameda, California-based startup that’s developing a case for tablet computers that can serve as a virtual interpreter for the deaf. Known as UNI, the case uses gesture recognition technology developed by Leap Motion to translate sign language into audible speech. It then merges this with voice recognition technology to convert spoken word to text. Because there are a variety of signs for any given word, users can upload new signs using a feature called Sign Builder. The system learns how individual users sign, while also distributing each new sign to every UNI device.
‘THIS COULD REALLY GIVE DEAF PEOPLE THE POWER TO LIVE THE LIFESTYLE THEY WANT TO LIVE. WE THINK THAT IS VERY POWERFUL.’
On Tuesday, MotionSavvy launched an IndieGoGo campaign for UNI to raise money and recruit beta testers to help build its dictionary of signs. For $499, a discounted rate, 200 selected backers will get a tablet and UNI case to try at home. “This could really give deaf people the power to live the lifestyle they want to live,” Campbell says, “and we think that is very powerful.”
Such technology would have seemed a distant dream not long ago. But the past decade has brought a wave of investment and interest in both gesture recognition technology and voice recognition technology, driven by companies like Apple and Microsoft, as well as smaller players like Nuance and Leap Motion. That hasn’t gone unnoticed by those who want to improve the lives of the deaf community. MotionSavvy is one of several players trying to capitalize on the convergence of these trends.
Just last week, Transcense, launched an IndieGoGo campaign for an app that provides real-time voice recognition so deaf people can follow a conversation. But unlike UNI, it doesn’t give deaf people who haven’t mastered speech a clear way to talk back. For MotionSavvy, that is the final—and most important—puzzle piece.
“It’s kind of like solving a quadratic equation at this point. It’s figuring out the right variables and stacking things together in such a way that they’ll all perform efficiently,” says Stephen Jacobs, associate director of Rochester Institute of Technology’s Center for Media Arts, Games Interaction, and Creativity.
Jacobs introduced Campbell to MotionSavvy CTO Alexandr Opalka when both were studying at RIT. Opalka, who also is deaf, had been working on similar technology as a student in RIT’s National Technical Institute for the Deaf. They teamed up with four other deaf students, and in 2012, launched MotionSavvy.
The technology is in its earliest stages. UNI recognizes only 300 signs, and its voice recognition component remains unreliable, though Opalka says UNI will come equipped with new and improved voice recognition for beta testers. And yet, during a demo of UNI at WIRED’s New York City office, it wasn’t hard to see just how transformative a technology like this could be. Campbell used it to sign a few common phrases to Opalka, such as “What’s your name?” and “Where are you from?” Yes, it was wonky, but still it struck me as sort of magical.
‘I BROUGHT THIS TO A TABLE OF OLDER DEAF PEOPLE, AND THEY ALL FREAKED OUT.’
Campbell says that reaction’s not entirely unique. “I brought this to a table of older deaf people, and they all freaked out,” he says.
But it’s not just the deaf and hard of hearing who are excited about UNI. Campbell says the FCC has gotten in touch. For many low-income deaf people, translators, video relay services, and other communication tools are prohibitively expensive. So the National Deaf-Blind Equipment Distribution Program picks up the tab. When the commercial version of UNI launches in 2015, it’ll cost $799, plus a $20 monthly subscription for Sign Builder. It’s not cheap, but it’s better than the alternative.
Campbell acknowledges the product is a “moonshot,” and admits it may never replace human interpreters. In fact, he and Opalka hope that it does the opposite. If UNI can achieve its intended purpose—facilitating one-on-one communication— then it could become easier for deaf people to get decent jobs. And who typically pays for interpreters? Employers. “If you can’t communicate during an interview, you’re not getting the job,” Opalka says. “With UNI, we predict more people who are deaf will be able to get jobs and stay working, and that’s how we’ll get more people to hire interpreters. There will be more people in the workforce.”
A Department of Veterans Affairs initiative targeting staph infections in hospitalized patients has produced positive results, according to data released by the VA.
Among VA patients in ICUs between 2007 and 2012, healthcare-associated MRSA infection rates dropped 72% — from 1.64 to 0.46 per 1,000 patient days. Infection rates dropped 66% — from 0.47 to 0.16 per 1,000 patient days — for patients treated in non-ICU hospital units.
“These results are striking,” Carolyn Clancy, MD, VA’s interim under secretary for health, said in a news release. “Healthcare-associated infections are a major challenge throughout the healthcare industry, but we have found in VA that consistently applying some simple preventive strategies can make a very big difference, and that difference is being recognized.”
VA’s prevention practices consist of patient screening programs for MRSA, contact precautions for hospitalized patients found to have MRSA, and hand hygiene reminders with hand sanitizer stations placed in common areas, patient wards and specialty clinics throughout medical centers, according to the release. Practices are reinforced via computerized reminders, training, measurement and continual feedback.
MRSA infections are a serious global healthcare issue and are difficult to treat because the bacterium is resistant to many antibiotics. In a Centers for Disease Control and Prevention 2012 MRSA surveillance report from its Active Bacterial Core surveillance, the CDC cites 75,309 cases of invasive MRSA infections and 9,670 deaths due to invasive MRSA in 2012, according to the release.
“The VA healthcare system is able to implement and assess these prevention strategies,” Martin Evans, MD, director of VA’s MRSA control program, said in the release. “What we’ve learned translates into better healthcare for the veterans we serve.”
James Wathen had stopped eating. Frail and barely able to speak, the 73-year-old whispered to a health care worker that he missed his dog, a one-eyed Chihuahua he hadn't seen since paramedics whisked him away to a Kentucky hospital weeks earlier.
So a team of nurses hustled to learn the fate of Wathen's beloved pet, Bubba, hoping a reunion might provide some peace and comfort to their heartbroken and deteriorating patient — even if arranging one meant bending ahospital rule against pets.
A series of phone calls eventually led the nurses to the Knox-Whitley Animal Shelter, where Bubba was taken and placed with a foster family, said Mary-Ann Smyth, president of the non-profit facility.
Coincidentally, Bubba had also recently fallen ill.
"The dog quit eating a week ago, which is very strange," Smyth told TODAY.com. "The dog didn’t know where James was and James didn't know where the dog was and believe it or not, they both stopped eating at about the same time."
Plans were made to bring the little pooch, who lacked his bottom row of teeth along with his right eye, to the hospital over the weekend.
“He was so sad at first. We had him wrapped in a baby blanket and he was shivering,” Smyth said. “The minute we got about 20 steps from this guy’s room — I kid you not — his little head went up. His eyes got real bright and he was like a different dog.”
She says a similar transformation took place in Wathen during his roughly 30-minute hospital reunion Saturday with Bubba.
"They didn’t think James was going to make it," she recalled being told during her initial visit to the hospital. “I was 10 feet from his bed and you could barely understand him because he was so hard to hear. The nurse had to lean up right against his face to hear what he was saying."
But he slowly perked up as his dog snuggled with him on his bed. By the time Bubba returned for a second visit Tuesday, visible changes were noticeable in both man and his best friend.
"He’s done a complete turnaround. He's speaking, he's sitting up, he’s eating. He doesn't look like the same guy," said Smyth, who didn't attend the second visit but saw Wathen in footage recorded by the shelter's director. "And the dog is eating and doing better now, too."
Baptist Health Corbin, the hospital treating Wathen, did not return repeated messages left by TODAY.com seeking comment.
But nurse Kimberly Probus told WKYT-TV a team of nurses went looking for Bubba after "one of our social workers realized it was mourning the loss of the dog that was making our patient even worse and emotionally unhealthy."
Smyth said she's not surprised at the healing power pets provide their owners.
"I hope this story will show to people the tremendous difference that animals can make in people’s lives," she said. She also hopes it will encourage people to think about rescuing pets from shelters like hers, which is rebuilding its facility after its previous home burned down in a fire last November.
“One of the biggest problems we face is the way some people think of animals. People just don’t see animals as creatures and beings, they see them as property,” she said. “I hope people understand they’re not 'its,' they’re 'beings.'”
The UCLA Health Interpreter/Translation and Deaf Services program provides services to all UCLA Health inpatients, outpatients, and their relatives at no cost. Every attempt is made to provide services in any language. The service will be provided by an in-person interpreter, video conference or by telephone.
Facebook CEO Mark Zuckerberg and his wife Dr. Priscilla Chan are donating $25 million to the CDC Foundation to help fight the Ebola epidemic, which has taken the lives of more than 4,000 people and continues to rage out of control in West Africa.
The donation will be used for the CDC Ebola response effort in the most severely affected countries of Guinea, Liberia and Sierra Leone and other areas of the world where the disease poses the greatest threat, the foundation said Tuesday.
"The Ebola epidemic is at a critical turning point," Zuckerberg said Tuesday in a statement posted on Facebook. "It has infected 8,400 people so far, but it is spreading very quickly and projections suggest it could infect 1 million people or more over the next several months if not addressed."
The CDC Foundation says the money will go towards urgent needs on the ground, including equipping community care centers, hiring and training local staff, identifying Ebola cases and tracing contacts, vehicles to be used for specimen transport, burial support, and translation services and communications -- all of which it says are vital to fighting the outbreak.
"The most important step we can take is to stop Ebola at its source," CDC director Dr. Tom Frieden said in a statement. "The sooner the world comes together to help West Africa, the safer we all will be." He said today's "significant contribution from Mark Zuckerberg and Dr. Priscilla Chan will help us rapidly advance the fight against Ebola."
When Donna Tookes learned she had breast cancer last winter, the 59-year-old thought she had no choice but to accept one of the most dreaded side-effects of chemotherapy: losing her mane of silver hair, a feature that strangers young and old frequently stopped to admire.
"I had resigned myself," Tookes told CBS News. "I had purchased an array of scarves, about 10. And I actually practiced tying them."
Tookes was diagnosed with breast cancer in January after her annual mammogram, when her doctors detected some mild calcifications in her right breast. These clusters of white flecks visible on her scan indicated there might be something seriously wrong. After a few subsequent tests, Tookes learned she had HER2 breast cancer, an especially aggressive form that can be difficult to treat. Though her doctors caught the cancer early, they wanted to be certain it would never return, which meant a unilateral mastectomy followed by 12 rounds of punishing chemotherapy.
"You have a consultation before you start chemotherapy," said Tookes, who lives with her husband and children in Stamford, Connecticut, and has worked for more than three decades as a flight attendant. "I was told I would lose my hair. And then the nurse assured me, she told me 'you're beautiful,' and that I was one of the only ones who could carry the bald look because I have that bone structure."
But her family could see that losing her hair would take a serious toll on her psyche. Tookes had heard about some treatment in Europe that helps prevent chemo-related hair loss, though she didn't know many details. Secretly, her husband began to conduct research. He wrote to friends in Sweden, who were able to obtain information about a new and innovative therapy called a scalp cooling cap. He soon found out that Mount Sinai Beth Israel in New York City was involved in a clinical trial on the device, known as the DigniCap System, which is worn by a patient during chemotherapy transfusions.
The snug cap is secured onto a patient's head each time she undergoes chemotherapy. It chills the scalp down to 5 degrees Celsius so that the blood vessels surrounding the hair roots contract, meaning that less of the toxins from chemo enter the hair follicle. This minimizes -- and in some cases completely stops -- a patient's hair from falling out.
At first, Tookes was slightly skeptical, but her family finally convinced her to move her cancer treatment from her hospital in Connecticut to Mount Sinai Beth Israel in New York City.
Dr. Paula Klein, assistant professor of medicine, hematology and medical oncology at the Icahn School of Medicine at Mount Sinai and principal investigator for the clinical trial, told CBS News the device has been effective at limiting hair loss in nearly all of her patients enrolled.
"Unfortunately, in breast cancer the two most active agents are associated with significant hair loss," said Klein. "For many women with early stage breast cancer, they are getting chemotherapy for prevention of recurrence."
Klein said overall, women who use the cap lose just 25 percent of their hair. There are some patients who lose more and a lucky handful who lost no hair at all.
The clinical trial is now in its final phase. The company behind the cap, Dignitana, will be submitting results to the U.S. Food and Drug Administration by the end of November, and hope to win FDA approval for the cap in 2015.
For women struggling through a difficult medical ordeal, the benefit is significant. Research published in 2008 in the journal Psycho-Oncology looked at 38 existing studies on breast cancer treatment and quality of life issues, and found hair loss consistently ranked the most troubling side effect of treatment for women. "Significant alopecia [hair loss] is problematic," said Klein. "Every time you look in the mirror, you remember you're getting cancer treatment."
Many breast cancer survivors report that even when their hair finally grows back after chemotherapy it is often different in color or texture than the hair they had before, due to the period of time it takes the hair follicles to recover from the damage caused by the drugs.
Moreover, the feelings associated with hair loss impact nearly every aspect of a breast cancer patient's life -- from her self-image and sexuality to whether or not she is comfortable at work or even walking into the supermarket to buy a quart of milk.
When she first prepared for treatment, Tookes worried how people would react to her appearance if she lost all of her hair. But it didn't happen. Seven weeks into chemo, she finally felt confident enough to return the unused wardrobe of scarves. She still had a full head of hair. Because the cooling therapy was used only on her scalp, Tookes did still lose her eyebrows and "everything south of there."
Tookes is now cancer-free and says the therapy helped her stay optimistic about her prognosis. "My mother used to say, you just comb your hair and get yourself together and you'll get through hard times," she said.
For more than two months, health officials have been struggling to understand the size of a national wave of severe respiratory illnesses caused by an unusual virus. This week, they expect the wave to start looking a whole lot bigger.
But that's because a new test will be speeding through a backlog of cases. Starting Tuesday, the Centers for Disease Control and Prevention is using a new test to help the agency process four or five times more specimens per day that it has been.
The test is a yes/no check for enterovirus 68, which since August has been fingered as the cause of hundreds of asthma-like respiratory illnesses in children — some so severe the patients needed a breathing machine. The virus is being investigated as a cause of at least 6 deaths.
It will largely replace a test which can distinguish a number of viruses, but has a much longer turnaround.
The result? Instead of national case counts growing by around 30 a day, they're expected to jump to 90 or more.
But for at least a week or two, the anticipated flood of new numbers will reflect what was seen in the backlog of about 1,000 specimens from September. The numbers will not show what's been happening more recently, noted Mark Pallansch, director of the CDC's division of viral diseases.
Enterovirus 68 is one of a pack of viruses that spread around the country every year around the start of school, generally causing cold-like illnesses. Those viruses tend to wane after September, and some experts think that's what's been happening.
One of the places hardest hit by the enterovirus 68 wave was Children's Mercy Hospital in Kansas City, Missouri. The specialized pediatric hospital was flooded with cases of wheezing, very sick children in August, hitting a peak of nearly 300 in the last week of the month.
But that kind of patient traffic has steadily declined since mid-September, said Dr. Jason Newland, a pediatric infectious diseases physician there.
"Now it's settled down" to near-normal levels, Newland said. Given the seasonality of the virus, "it makes sense it would kind of be going away," he added.
The germ was first identified in the U.S. in 1962, and small numbers of cases have been regularly reported since 1987. Because it's not routinely tested for, it may have spread widely in previous years without being identified in people who just seemed to have a cold, health officials have said.
But some viruses seem to surge in multi-year cycles, and it's possible that enterovirus surged this year for the first time in quite a while. If that's true, it may have had an unusually harsh impact because there were a large number of children who had never been infected with it before and never acquired immunity, Newland said.
Whatever the reason, the virus gained national attention in August when hospitals in Kansas City and Chicago saw severe breathing illnesses in kids in numbers they never see at that time of year.
Health officials began finding enterovirus 68. The CDC, in Atlanta, has been receiving specimens from severely ill children all over the country and doing about 80 percent of the testing for the virus. The test has been used for disease surveillance, but not treatment. Doctors give over-the-counter medicines for milder cases, and provide oxygen or other supportive care for more severe ones.
The CDC has been diagnosing enterovirus 68 in roughly half of the specimens sent in, Pallansch said. Others have been diagnosed with an assortment of other respiratory germs.
As of Friday, lab tests by the CDC have confirmed illness caused by the germ in 691 people in 46 states and the District of Columbia. The CDC is expected to post new numbers Tuesday and Wednesday.
Aside from the CDC, labs in California, Indiana, Minnesota and New York also have been doing enterovirus testing and contributing to the national count. It hasn't been determined if or when the states will begin using the new test, which was developed by a CDC team led by Allan Nix.
Meanwhile, the virus also is being eyed as possible factor in muscle weakness and paralysis in at least 27 children and adults in a dozen states. That includes at least 10 in the Denver area, and a cluster of three seen at Children's Mercy, Newland said.
It takes nerves of steel to win World Cup, World Championship and Olympic titles like Mikaela Shiffrin. Yet, the alpine skier melted into a pool of tears after hearing from a young Swedish girl she has called her “little lucky charm.”
Shiffrin met 11-year-old Emma Lundell two years ago in Are, Switzerland, after winning her first World Cup title, NBC Sports reported. Emma was battling leukemia at the time and had asked Shiffrin for a photograph.
“That was the biggest wake up call," Shiffrin recalled for Swedish publication SPORT-Expressen, which surprised her with a video update from Emma, who is now 13 and has finished chemotherapy treatments. Emma, whose hair has grown back, says she's even healthy enough to resume cross-country skiing.
“I’m so honored that you have thought of me. To be mentioned as your lucky charm is the nicest and greatest thing ever,” she said in her message to Shiffrin, who repeatedly wiped away tears while watching.
“Wow,” Shiffrin said. “She looks so good. Oh my gosh, that makes me so happy. I wonder about her a lot actually.”
And the skier's reply to her young fan was equally moving.
"Emma, I’m so glad that you’re healthy, and that your chemo is done, and your hair is beautiful,” she said.
“I hope I see you again, maybe in Are. I think about you a lot and I’m very glad that I met you because you keep me grounded when I get arrogant. And I think about how tough it must have been for you, and I’m so glad to have met you and I wish you the best.”
Released on Friday, the survey of 700 Registered Nurses at over 250 hospitals in 31 states included some sobering preliminary results in terms of hospital policies for patients who present with potentially infectious diseases like Ebola.
80% say their hospital has not communicated to them any policy regarding potential admission of patients infected by Ebola
87% say their hospital has not provided education on Ebola with the ability for the nurses to interact and ask questions
One-third say their hospital has insufficient supplies of eye protection (face shields or side shields with goggles) and fluid resistant/impermeable gowns
Nearly 40% say their hospital does not have plans to equip isolation rooms with plastic covered mattresses and pillows and discard all linens after use, less than 10 percent said they were aware their hospital does have such a plan in place
More than 60% say their hospital fails to reduce the number of patients they must care for to accommodate caring for an “isolation” patient
National Nurses United (NNU) started the survey several weeks ago and released the preliminary results last Friday (here). The NNU has close to 185,000 members in every state and is the largest union of registered nurses in the U.S.
The release of the survey coincided with Friday’s swirling controversy on how the hospital in Dallas mishandled America’s first case of Ebola. The patient ‒ Thomas E. Duncan ‒ was treated and released with antibiotics even though the hospital staff knew of his recent travel from Liberia ‒ now the epicenter of this Ebola outbreak.
On October 2, the hospital tried to lay blame of the mishandled Ebola patient on their electronic health record (EHR) software with this statement.
Protocols were followed by both the physician and the nurses. However, we have identified a flaw in the way the physician and nursing portions of our electronic health records (EHR)interacted in this specific case. In our electronic health records, there are separate physician and nursing workflows. Texas Health Presbyterian Hospital Statement ‒ October 2 (here)
Within 24 hours, the hospital recanted the statement by saying no, in fact, “there was no flaw.”
The larger issue, of course, is just how ready are the more than 5,700 hospitals around the U.S. when it comes to diagnosing and then treating suspected cases of Ebola. Given the scale of the outbreak (a new case has now been reported in Spain ‒ Europe’s first), it’s very likely we’ll see more cases here in the U.S.
As an RN herself ‒ and Director of NNU’s Registered Nurse Response Network ‒ Bonnie Castillo was blunt.
What our surveys show is a reminder that we do not have a national health care system, but a fragmented collection of private healthcare companies each with their own way of responding. As we have been saying for many months, electronic health records systems can, and do, fail. That’s why we must continue to rely on the professional, clinical judgment and expertise of registered nurses and physicians to interact with patients, as well as uniform systems throughout the U.S. that is essential for responding to pandemics, or potential pandemics, like Ebola. Bonnie Castillo, RN ‒ Director of NNU’s Registered Nurse Response Network (press release)
As a part of their Health Alert Network (HAN), the CDC has been sounding the alarm since July ‒ and released guidelines for evaluating U.S. patients suspected of having Ebola through the HAN on August 1 (HAN #364). As a part of alert #364, the CDC was specific on recommending tests “for all persons with onset of fever within 21 days of having a high‒risk exposure.” Recent travel from Liberia in West Africa should have prompted more questioning around potential high-risk exposure ‒ which was, in fact, the case.
As it was, a relative called the CDC directly to question the original treatment of Mr. Duncan given all the circumstances.
“I feared other people might also get infected if he wasn’t taken care of, and so I called them [the CDC] to ask them why is it a patient that might be suspected of this disease was not getting appropriate care.” Josephus Weeks ‒ Nephew of Dallas Ebola patient to NBC News
The CDC has also activated their Emergency Operations Center (EOC).
The EOC brings together scientists from across CDC to analyze, validate, and efficiently exchange information during a public health emergency and connect with emergency response partners. When activated for a response, the EOC can accommodate up to 230 personnel per 8-hour shift to handle situations ranging from local interests to worldwide incidents.
The EOC coordinates the deployment of CDC staff and the procurement and management of all equipment and supplies that CDC responders may need during their deployment.
In addition, the EOC has the ability to rapidly transport life-supporting medications, samples and specimens, and personnel anywhere in the world around the clock within two hours of notification for domestic missions and six hours for international missions.
One out of every six newly licensed nurses (more than 17 percent) leave their first nursing job within the first year and one out of every three (33.5 percent) leave within two years. But not all nurse turnover is bad, according to a new study from the RN Work Project, funded by the Robert Wood Johnson Foundation.
“It seemed high,” said Carol S. Brewer, PhD, RN, FAAN, professor at the University at Buffalo School of Nursing and co-director of the RN Work Project, the only longitudinal study of registered nurses conducted in the United States. “Most of them take a new job in a hospital. We’ve emphasized who left their first job, but it doesn’t mean they have left hospital work necessarily.”
While many nursing leaders have voiced concern that high turnover among new nurses may result in a loss of those nurses to the profession, that’s not what the RN Work Project team has found. Most of those leaving move on to another job in health care.
“Not only are they staying in health care, they are staying in health care as nurses,” said Christine T. Kovner, PhD, RN, FAAN, professor at the New York University College of Nursing and co-director of the RN Work Project. “Very few leave. A tiny percent become a case manager or work for an insurance company, verifying people had the right treatment.”
Such outside jobs tend to offer better hours, with no nights or weekends. The nurses are still using their knowledge and skills but they are not providing hands-on care.
The RN Work Project looks at nurse turnover from the first job, and the majority of first jobs are in the hospital setting, Brewer explained. However, in the sample, nurses working in other settings had higher turnover rates than those working in acute care.
Kovner hypothesized that since new nurses are having a harder time finding first jobs in hospitals, they may begin their careers in a nursing home and leave when a hospital position opens up. On the other hand, those who succeed in landing a hospital job may feel the need to stay at least a year, because that’s what many nursing professors recommend. Hospitals also tend to offer better benefits, such as tuition reimbursement and child care, and hold an attraction for new nurses.
“Our students, if they could get a job in an ICU, they’d be happy, and the other place they want to work is the emergency room,” Kovner said. “They want to save lives, every day.”
The RN Work Project data excludes nurses who have left their first position at a hospital for another in the same facility, which is disruptive to the unit but may be a positive for the organization overall, since the nurse knows the culture and policies. The nurse may change to come off the night shift or to obtain a position in a specialty unit, such as pediatrics.
“That’s an example of the type of turnover an organization likes,” Kovner said. “You have an experienced nurse going to the ICU [or another unit].”
While nurse turnover represents a high cost for health care employers, as much as $6.4 million for a large acute care hospital, some departures of RNs is good for the workplace. Brewer, Kovner and colleagues describe the difference between dysfunctional and functional turnover in the paper, published in the journal Policy, Politics & Nursing Practice.
“Dysfunctional is when the good people leave,” Brewer said.
The RN Work Project has not differentiated between voluntary and involuntary departures, the latter of which may be due to poor performance or downsizing. And some nurse turnover is beneficial.
“If you never had turnover, the organization would become stagnant,” Kovner added. “It’s useful to have some people leave, particularly the people you want to leave. It offers the opportunity to have new blood come in.”
New nursing graduates might bring with them the latest knowledge, and more seasoned nurses may bring ideas proven successful at other organizations.
Once again, Brewer and Kovner report managers or direct supervisors play a big role in nurses leaving their jobs. Organizations hoping to reduce turnover could consider more management training for people in those roles.
“Leadership seems a big issue,” Brewer said. “The supervisor support piece has been consistent.”
Both nurse researchers cited the challenge of measuring nurse turnover accurately. Organizations and researchers often describe it differently, Brewer said. And hospitals often do not want to release information about their turnover rates, since nurses would most likely apply to those with lower rates, Kovner added. When assessing nurse turnover data, she advises looking at the response rate and the methodology used.
“There are huge inconsistencies in reports about turnover,” Kovner said. “It’s extremely important managers and policy makers understand where the data came from.”
For years Larry Hester lived in darkness, his sight stolen by a disease that destroyed the photoreceptor cells in his retinas. But last week, through the help of a “bionic eye,” Hester got a chance to once again glimpse a bit of the world around him.
Hester is the seventh patient to receive an FDA-approved device that translates video signals into data the optic nerve can process. The images Hester and others “see” will be far from full sight, but experts hope it will be enough to give a little more autonomy to those who had previously been completely blind.
Hester’s doctors at Duke University Eye Center believe that as time goes on the 66-year-old tire salesman from Raleigh, N.C., will be able to “see” more and more. After only five days, there has been remarkable progress.
“I hope that [after some practice] he will be able to do things he can’t do today: maybe walk around a little more independently, see doorways or the straight line of a curb. We don’t expect him to be able to make out figures on TV. But we hope he’ll be more visually connected.” said Dr. Paul Hahn, an assistant professor of ophthalmology at the university in Durham.
It was at Duke three decades ago that Hester learned that something was seriously wrong with his eyes. After a battery of tests, doctors delivered the disheartening news: Hester had retinitis pigmentosa, a disease that would inexorably chip away at the rods and cones in his retinas, eventually leaving him blind.
“It was a pretty devastating blow, frankly,” Hester said. “I was 33 at the time.”
But Larry Hester wasn’t the sort of guy to sit around feeling sorry for himself. With the support of family, friends and a devoted wife, he found a way to live his life as normally as possible, depending on his memory to help him navigate around his home and his workplace.
One day his wife, Jerry, saw a story about a device that might help Larry. The FDA had just approved it for use in people who suffer from the same condition as Larry —some 50,000 to 100,000 in the U.S.
Larry was just the kind of patient that Hahn was looking for to try out the Argus II Retinal Prosthesis system, and he became the first to get the device at Duke.
Argus was designed to bypass damaged photoreceptors and send signals directly to the next layer of retinal cells, which are on the pathway to the optic nerve.
A miniature video camera seated in a pair of glasses captures what the patient is “looking” at and sends the video through a thin cable to a small external computer that transforms the images into signals that can be understood by that second layer of retinal cells. Those data are then sent back to the glasses, which transmit the information through a small antenna to an array of 60 tiny electrodes that implanted up against the patient’s retina.
The electrodes emit small pulses of electricity that make their way up the undamaged retinal cells to the optic nerves, creating the perception of patterns of light. The hope is that patients will learn to interpret those patterns as images.
Last week with the new glasses perched on his nose, Larry sat in a chair at Duke surrounded by medical staff and his family — all waiting for Hahn to turn on the device. Directly in front of Larry was a brightly lit screen.
“At the count of three, we’re going to hit the start button and we’ll see what happens,” Hahn said.
At three, a smile started to play on Larry’s lips.
“Yes,” he said and the smile broadened across his face. “Oh my goodness!”
Jerry looked at him and exclaimed, “Can you see, Larry?”
After giving her husband a kiss, she asked again, “Can you really see?”
“Yes. Flashing. Big time flashing.”
Experts see the new device as the start of something big.
“It’s a fairly limited device, but it’s an amazing leap forward,” said Dr. Colin McCannel, a retinal expert at the Jules Stein Eye Institute at the University of California, Los Angeles. “It’s not the vision you or I are used to. But for someone who has been in complete darkness it must be amazing to see again. I think it’s absolutely phenomenal.”
Dr. Neil Bressler turns to the space program for an analogy.
“It’s like the first rocket ship that went up and down, or when John Glenn went into orbit,” said Bressler, a professor of ophthalmology and chief of the retina division at Johns Hopkins Medicine. “If you asked can we put a man on the moon the next day the answer would be no. It was the first of many steps to achieve the objective of putting a man on the moon.”
While the device isn’t even close to giving Larry back the vision he was born with, he can see contrasts, which allows him, for example, to distinguish between a white wall and a darkened doorway.
If you’ve lived in darkness for decades, that little bit of new-found vision can be a huge gift.
“The other night I was sitting on a dark leather chair,” Jerry said. “He was able to scan over and see my face because it was lighter. And he reached out and touched my face. That is the first time he had done that in a long time. It was a sweet and precious moment.”
Linda Carroll is a regular contributor to NBCNews.com and TODAY.com. She is co-author of "The Concussion Crisis: Anatomy of a Silent Epidemic” and the recently published “Duel for the Crown: Affirmed, Alydar, and Racing’s Greatest Rivalry.”
At present, diagnosis of lung cancer relies on an invasive biopsy that is only effective after tumors are bigger than 3 cm or even metastatic. Earlier detection would vastly improve patients' chances of survival. Now a team of researchers is developing a "lab-on-a-chip" that promises to detect lung cancer - and possibly other deadly cancers - much earlier, using only a small drop of a patient's blood.
In the Royal Society of Chemistry journal, Yong Zeng, assistant professor of chemistry at the University of Kansas, and colleagues report a breakthrough study describing their invention.
For some time, scientists have been excited by the idea of testing for disease biomarkers in "exosomes" - tiny vesicles or bags of molecules that cells, including cancer cells - release now and again. When they first spotted them, researchers thought exosomes were just for getting rid of cell waste, but now they know they also do other important things such as carry messages to other cells near and far.
The challenge, however, is developing a technology that is small enough to target and analyze the contents of exosomes - mostly nucleic acids and proteins - to find unique biomarkers of disease. This is because exosomes are tiny - around 30 to 150 nanometers (nm) in diameter - much smaller, for example, than red blood cells.
Current methods for separating out and testing exosomes require several steps of ultracentrifugation - a lengthy and inefficient lab procedure, as Prof. Zeng explains:
"There aren't many technologies out there that are suitable for efficient isolation and sensitive molecular profiling of exosomes. First, current exosome isolation protocols are time-consuming and difficult to standardize. Second, conventional downstream analyses on collected exosomes are slow and require large samples, which is a key setback in clinical development of exosomal biomarkers."
Now, using microfluid technology, he and his colleagues have developed a lab-on-a-chip that can analyze the contents of targeted exosomes and spot the early signs of deadly cancer. They have already successfully tested it on lung cancer.
Lab-on-a-chip device uses smaller samples, is faster, cheaper and more sensitive
The new device, which uses much smaller samples, promises to produce results faster, more cheaply, with better sensitivity compared to conventional benchtop instruments, as Prof. Zeng continues to explain:
"A lab-on-a-chip shrinks the pipettes, test tubes and analysis instruments of a modern chemistry lab onto a microchip-sized wafer."
The technology behind the device - known as microfluidics - came out of new semiconductor electronics and has been under intensive development since the 1990s, he adds:
"Essentially, it allows precise manipulation of minuscule fluid volumes down to one trillionth of a liter or less to carry out multiple laboratory functions, such as sample purification, running of chemical and biological reactions, and analytical measurement."
Unlike breast and colon cancer, there is no widely accepted screening tool for lung cancer, which in most cases is first diagnosed based on symptoms that normally indicate lung function is already impaired.
To diagnose lung cancer, doctors have to perform a biopsy - remove a piece of tissue from the lung and send it to a lab for molecular analysis. It is rarely possible to do this in the early stages as tumors are too small to be spotted on scans.
"In contrast, our blood-based test is minimally invasive, inexpensive, and more sensitive, thus suitable for large population screening to detect early-stage tumors," says Prof. Zeng, adding that the technique offers a general platform for detecting exosomes from cancer cells. The team has already used the device to test for ovarian cancer, and in theory, says Prof. Zeng, it should also be applicable to other cancer types.
"Our long-term goal is to translate this technology into clinical investigation of the pathological implication of exosomes in tumor development. Such knowledge would help develop better predictive biomarkers and more efficient targeted therapy to improve the clinical outcome," he adds.
The team has received further funding from the National Cancer Institute at the National Institutes of Health to further develop the lab-on-a-chip.
In March 2013, Medical News Today learned how another team of scientists is developing a lab-on-a-chip that is implanted under the skin to track levels of substances in the blood and transmit the results wirelessly to a smartphone or other receiving device.
Editor's note: Brittany Maynard is a volunteer advocate for the nation's leading end-of-life choice organization, Compassion and Choices. She lives in Portland, Oregon, with her husband, Dan Diaz, and mother, Debbie Ziegler. Watch Brittany and her family tell her story at www.thebrittanyfund.org. The opinions expressed in this commentary are solely those of the author.
(CNN) -- On New Year's Day, after months of suffering from debilitating headaches, I learned that I had brain cancer.
I was 29 years old. I'd been married for just over a year. My husband and I were trying for a family.
Our lives devolved into hospital stays, doctor consultations and medical research. Nine days after my initial diagnoses, I had a partial craniotomy and a partial resection of my temporal lobe. Both surgeries were an effort to stop the growth of my tumor.
In April, I learned that not only had my tumor come back, but it was more aggressive. Doctors gave me a prognosis of six months to live.
Because my tumor is so large, doctors prescribed full brain radiation. I read about the side effects: The hair on my scalp would have been singed off. My scalp would be left covered with first-degree burns. My quality of life, as I knew it, would be gone.
After months of research, my family and I reached a heartbreaking conclusion: There is no treatment that would save my life, and the recommended treatments would have destroyed the time I had left.
I considered passing away in hospice care at my San Francisco Bay-area home. But even with palliative medication, I could develop potentially morphine-resistant pain and suffer personality changes and verbal, cognitive and motor loss of virtually any kind.
Because the rest of my body is young and healthy, I am likely to physically hang on for a long time even though cancer is eating my mind. I probably would have suffered in hospice care for weeks or even months. And my family would have had to watch that.
I did not want this nightmare scenario for my family, so I started researching death with dignity. It is an end-of-life option for mentally competent, terminally ill patients with a prognosis of six months or less to live. It would enable me to use the medical practice of aid in dying: I could request and receive a prescription from a physician for medication that I could self-ingest to end my dying process if it becomes unbearable.
I quickly decided that death with dignity was the best option for me and my family.
We had to uproot from California to Oregon, because Oregon is one of only five states where death with dignity is authorized.
I met the criteria for death with dignity in Oregon, but establishing residency in the state to make use of the law required a monumental number of changes. I had to find new physicians, establish residency in Portland, search for a new home, obtain a new driver's license, change my voter registration and enlist people to take care of our animals, and my husband, Dan, had to take a leave of absence from his job. The vast majority of families do not have the flexibility, resources and time to make all these changes.
I've had the medication for weeks. I am not suicidal. If I were, I would have consumed that medication long ago. I do not want to die. But I am dying. And I want to die on my own terms.
I would not tell anyone else that he or she should choose death with dignity. My question is: Who has the right to tell me that I don't deserve this choice? That I deserve to suffer for weeks or months in tremendous amounts of physical and emotional pain? Why should anyone have the right to make that choice for me?
Now that I've had the prescription filled and it's in my possession, I have experienced a tremendous sense of relief. And if I decide to change my mind about taking the medication, I will not take it.
Having this choice at the end of my life has become incredibly important. It has given me a sense of peace during a tumultuous time that otherwise would be dominated by fear, uncertainty and pain.
Now, I'm able to move forward in my remaining days or weeks I have on this beautiful Earth, to seek joy and love and to spend time traveling to outdoor wonders of nature with those I love. And I know that I have a safety net.
I hope for the sake of my fellow American citizens that I'll never meet that this option is available to you. If you ever find yourself walking a mile in my shoes, I hope that you would at least be given the same choice and that no one tries to take it from you.
When my suffering becomes too great, I can say to all those I love, "I love you; come be by my side, and come say goodbye as I pass into whatever's next." I will die upstairs in my bedroom with my husband, mother, stepfather and best friend by my side and pass peacefully. I can't imagine trying to rob anyone else of that choice.
What are your thoughts about "death with dignity"?
Ashley and Tyson Gardner of Pleasant Grove, Utah, tried to conceive for eight years when they turned to in vitro fertilization this summer.
Boy, did it work. Or rather, girl, did it work. In July, they got the “surprise of our lives” when they went in for an ultrasound and found out they are expecting two sets of identical twins -- all girls.
A photo of the couple looking shocked while holding the ultrasound images has gone viral on their Facebook page, which also features photos of the moment they first found out Ashley was pregnant.
"My whole goal in opening up about this is to promote infertility awareness," she said in a recent YouTube video. "It's not something that's talked about a lot and it's a really hard trial that people go through."
Ashley's fertility problems were caused by endometriosis, so the couple at first tried intrauterine insemination, she told BabyCenter.com. When that didn't work, they tried IVF, which cost them $12,000 out of their own pockets.
Ashley is now 18 weeks along and she and her husband are busy trying to pick names for their four girls.
"We were so blessed," she writes on her Facebook page.
Imagine swallowing a pill with tiny needles instead of getting an injection. Then again, imagine swallowing a pill with tiny needles. It may sound painful, but according to the researchers who developed the novel capsule - which could replace painful injections - there are no harmful side effects.
The researchers, from the Massachusetts Institute of Technology (MIT) and Massachusetts General Hospital (MGH), have published the results of their study - which tested the microneedle pill in the gastrointestinal (GI) tracts of pigs - in the Journal of Pharmaceutical Sciences.
Though most of us would probably prefer swallowing a pill over having an injection, many drugs cannot be given in pill form because they are broken down in the stomach before being absorbed.
Biopharmaceuticals made from large proteins, such as antibodies - known as "biologics" - are used to treat cancer, arthritis and Crohn's disease, and also include vaccines, recombinant DNA and RNA.
"The large size of these biologic drugs makes them nonabsorbable," explains lead author MIT graduate student Carl Schoellhammer. "And before they even would be absorbed, they're degraded in your GI tract by acids and enzymes that just eat up the molecules and make them inactive."
In an effort to design a capsule that is capable of delivering a wide range of drugs - while preventing degradation and effectively injecting the medicine into the GI tract - Schoellhammer and colleagues constructed the capsule from acrylic, including a reservoir for the drug that is coated with hollow, 5 mm long needles made of stainless steel.
The capsule measures 2 cm long and 1 cm in diameter.
Needle capsule worked safely and effectively in pigs
The team notes that previous studies involving humans who have accidentally swallowed sharp objects have suggested swallowing a capsule coated with short needles could be safe. They explain that there are no pain receptors in the GI tract and that, as a result, patients would not feel any pain.
But to assess whether their capsule could safely and effectively deliver the drugs, the researchers tested the pill in pigs, using insulin in the drug reservoir.
The capsules took more than a week to move through the whole digestive tract, and there were no traces of tissue damage, the researchers say. Additionally, the microneedles effectively injected insulin into the lining of the pigs' stomachs, small intestines and colons, which resulted in their blood glucose levels dropping.
Co-lead author Giovanni Traverso, a research fellow at MIT's Koch Institute for Integrative Cancer Research and gastroenterologist at MGH, notes that the pigs' reduction in blood glucose was faster and larger than the drop observed from insulin injection.
"The kinetics are much better and much faster-onset than those seen with traditional under-the-skin administration," he says. "For molecules that are particularly difficult to absorb, this would be a way of actually administering them at much higher efficiency."
'Oral delivery of drugs is a major challenge'
Though they used insulin for their tests in pigs, the researchers say they envision their capsule being used to deliver biologics to humans.
"This could be a way that the patient can circumvent the need to have an infusion or subcutaneous administration of a drug," says Traverso.
Prof. Samir Mitragotri, a professor at the University of California-Santa Barbara - who was not involved in the research - says:
"This is a very interesting approach. Oral delivery of drugs is a major challenge, especially for protein drugs. There is tremendous motivation on various fronts for finding other ways to deliver drugs without using the standard needle and syringe."
In terms of future modifications, the team plans to alter the capsule so that contractions of the digestive tract slowly squeeze the drug out of the capsule as it travels through the body, and they also want to make the needles out of degradable polymers and sugar that break off, becoming embedded in the gut lining and slowly disintegrating.
A British-American scientist and a pair of Norwegian researchers were awarded this year’s Nobel Prize in Physiology or Medicine on Monday for discovering “an inner GPS, in the brain,” that makes navigation possible for virtually all creatures.
John O’Keefe, 75, a British-American scientist, will share half of the prize of 8 million kronor, or $1.1 million, in what is considered the most prestigious scientific award. May-Britt Moser, 51, and Edvard I. Moser, 52, who are married, will share the other half, said the Karolinska Institute in Sweden, which chooses the laureates.
The three scientists’ discoveries “have solved a problem that has occupied philosophers and scientists for centuries — how does the brain create a map of the space surrounding us and how can we navigate our way through a complex environment,” the institute said in a news release.
The positioning system in the brain that they discovered helps us know where we are, find our way from place to place and store the information for the next time, said Goran K. Hansson, secretary of the Karolinska’s Nobel Committee, in announcing the laureates.
The researchers documented that certain cells are responsible for higher cognitive function that steers the navigational system, the committee said.
Dr. O’Keefe began using neurophysiological methods in the late 1960s to study how the brain controls behavior. In 1971 he discovered the first component of the inner navigational system in rats. He identified nerve cells in the hippocampus region of the brain that were always activated when a rat was at a certain location. He called them “place cells” and showed that the cells registered not only what they saw, but also what they did not see, by building up inner maps in different environments.
Dr. O’Keefe was born in New York City and graduated from the City College of New York. He earned a Ph.D. in physiological psychology at McGill University in Montreal, in 1967, and moved for postdoctoral training to University College London, where he remains. He is a professor of cognitive neuroscience.
In 2005, the Mosers discovered a second crucial component of the brain’s positioning system by identifying another type of nerve cell that permits coordination and positioning. The scientists, who work at the Norwegian University of Science and Technology in Trondheim, called the cells grid cells. While mapping connections to the hippocampus in rats moving about a room in a laboratory, “they discovered an astonishing pattern of activity in a nearby part of the brain called the entorhinal cortex,” the Nobel committee said.
When the rat passed multiple locations, the cells formed a hexagonal grid. Each cell activated in unique spatial patterns. Their research showed “how both ‘place’ and ‘grid’ cells make it possible to determine position and to navigate,” the committee said.
The Mosers grew up in rural Norway and came from nonacademic families. May-Britt was born in Fosnavag and Edvard in Alesund. Although they went to the same high school, they did not know each other well until they were undergraduates at the University of Oslo. They married while they were college students and have two daughters. Both are professors at the university in Trondheim.
At one point they were visiting scientists at University College London, studying under Dr. O’Keefe.
The three also won Columbia University’s Louisa Gross Horwitz Prize last year for their discoveries.
Only a handful of married couples have shared a Nobel Prize, and the Mosers are only the second in the medicine category, which has been awarded since 1901. Fewer than a dozen women have been named laureates in medicine.
Evidence that place and grid cells exist in humans comes from recent studies using brain imaging techniques and from patients who have undergone neurosurgery.
The laureates’ findings may eventually lead to a better understanding of the spatial losses that occur in Alzheimer’s and other neurological diseases. The hippocampus and entorhinal cortex are often damaged in early stages of Alzheimer’s, with affected individuals’ losing their way and failing to recognize the environment. The findings also open new avenues for understanding cognitive processes like memory, thinking and planning, the Nobel Committee said.
According to The Associated Press, May-Britt Moser said the couple was elated. “This is such a great honor for all of us and all the people who have worked with us and supported us,” she said in a telephone interview with The A.P. “We are going to continue and hopefully do even more groundbreaking work in the future.”
Her husband was flying when the prize was announced, she said, and he later told the Norwegian news agency NTB that he learned about it when he landed and turned on his cellphone, to a barrage of messages and calls. “I didn’t know anything. When I got off the plane there was a representative there with a bouquet of flowers who said ‘congratulations on the prize,’ ” The Associated Press reported.
The laureates traditionally receive their awards at a banquet in Stockholm on Dec. 10, the anniversary of the death in 1896 of the prize’s creator, Alfred Nobel, an industrialist and inventor of dynamite.
I just had a Skype chat with entrepreneur Olivier Jeannel about his new product. It was a text chat, as Olivier – just like roughly 70 million people in the world (of which approximately 26 million of Americans) – suffers from profound hearing loss. If he has his way, soon this is no longer going to be a problem. Together with his associate Sidney Burks and product manager Pablo Seuc-Rocher, he’s working on the launch of RogerVoice, an Android app that has been designed from the ground up for those who cannot hear on the phone.
With RogerVoice, the deaf or hard-of-hearing person starts a call and receives on his smartphone instant live transcriptions of what the other speaker is saying, regardless if he is speaking in English or another of the many other languages recognized by the system (Spanish, Portuguese, French, Italian, German, Greek and Japanese top the list).
While the idea, generally speaking, is brilliant, there are still some hurdles to overcome. Automatic speech recognition (ASR) technology is still far from flawless; also, unlike other softwares (Dragon and friends) that can be trained to recognize a single voice, improving this way the recognition rate, RogerVoice has to work with any kind of voice, so don’t imagine you can have a long, complex conversation without any trouble.
“You might use it to confirm an appointment with a doctor – Olivier says – or tell a plumber to come”. Basic stuff, but enough to significantly improve the quality of life of a deaf person, allowing he or she to rely less on other people’s intervention. It’s also up to the hearing person to make a better effort to enunciate, to help the voice recognition software’s performance. So you could in fact have a long and articulate conversation, provided that the counterpart is a relative, a friend, or someone that’s kind enough not to speak in a rush.
I asked Jeannel if – when the problem is not too severe – an hearing aid wouldn’t work as well, and the answer was quite interesting, because it pointed to the social implications of suffering from hearing loss.
“The interesting fact is – he says – that most deaf people don’t wear hearing aids, only 1 in 5 apparently bother to get equipped. This is because wearing hearing aids is often associated to a kind of social stigma. Also, of the profoundly deaf population, most manage to speak, but understanding a conversation without visual cues is difficult, if not impossible. In my case, impossible without lip-reading. More and more profoundly deaf use cochlear implants, which is a revolution: it helps a lot to understand speech, but it’s still quite difficult over a phone”.
The app is designed to be Bluetooth compatible, meaning that the RogerVoice app could connect directly to a Bluetooth-equipped hearing aid for a better listening experience and, after the launch of the Android version, the team will start working on the iOS and Windows ones.
The business model will be based on subscriptions, with one year of unlimited calls priced at $59 for those that will contribute to the Kickstarter campaign that’s currently running to support the product’s development. As for the time to market, if the $20,000 is reached on Kickstarter, founder hope to release the product by the end of the year. “Hopefully for Christmas – Jeannel says”.
Annette Tersigni decided at the age of 48 that she wanted to make a difference. She attended nursing school and became a registered nurse three years later. “Having that precious pair of letters – RN – at the end of my name gave me everything I wanted,” she writes on her website. Before long, Tersigni discovered the rewards – as well as the physical and emotional challenges – that come with nursing.
“I was always stressed when I worked, afraid to get sued for making a mistake or medical error,” says Tersigni, who was working in the heart transplant unit of a North Carolina hospital. “Plus, working the night shift caused me to gain weight and stop working out.” Tersigni moved to another hospital, but the long shifts continued. Three years later, she left her job.
Tersigni’s experience isn’t unusual. Three out of four nurses cited the effects of stress and overwork as a top health concern in a 2011 survey by the American Nurses Association. The ANA attributed problems of fatigue and burnout to “a chronic nursing shortage.” A 2012 report in the American Journal of Medical Quality projected a shortage of registered nurses to spread across the country by 2030.
Work schedules and insufficient staffing are among the factors driving many nurses to leave the profession. American nurses often put in 12-hour shifts over the course of a three-day week. Research found nurses who worked shifts longer than eight to nine hours were two-and-a-half times more likely to experience burnout.
“Our results show that nurses are underestimating their own recovery time from long, intense clinical engagement, and that consolidating challenging work into three days may not be a sustainable strategy to attain the work-life balance they seek,” says study author Linda Aiken, PhD, director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania School of Nursing.
Deborah Burger, RN, co-president of the union and professional association National Nurses United, doesn’t believe that long work shifts tell the whole story. “Most people can work a 10- or 12-hour shift if they’ve got the right support and right level of staffing,” Burger says.
“In order for nurses to feel satisfied and fulfilled with their work, the staffing issues must be seriously addressed from a very high level,” says Eva Francis, MSN, RN, CCRN, a former nursing administrator. “Nurses also need to be able to express themselves professionally about the workload, and be heard without the fear of threat to their jobs or the fear of being singled out.”
A new study suggests that nurses’ burnout risk may be related to what drew them to the profession in the first place. Researchers at the University of Akron in Ohio surveyed more than 700 RNs and found that nurses who are motivated primarily by the desire to help others, rather than by enjoyment of the work, were more likely to burn out.
“We assume that people that go into nursing because they are highly motived by helping others are the best nurses,” says study author Janette Dill, assistant professor of sociology at the University of Akron. “But our findings suggest these nurses may be prone to burnout and other negative physical symptoms.”
RELATED: Managing Job Stress
That finding doesn’t surprise Jill O’Hara, a former nurse from Hamburg, NY, who left nursing more than a decade ago.
“When a person goes into nursing as a profession, it’s either because it’s a career path or a calling,” says O’Hara, 56, who now operates her own holistic health consulting practice. “The career nurse can leave work at the end of the day and let it go, but the nurse who enters the field because she is called to it takes those emotionally charged encounters home with her. They are empathetic, literally connecting emotionally with their patients, and it becomes a part of them energetically.”
Besides driving many nurses out of the profession, burnout can compromise the quality of patient care. A study of Pennsylvania hospitals found a “significant association” between high patient-to-nurse ratios and nurse burnout with increased infections among patients. The authors’ conclusion: A reduction in burnout is good for nurses and patients.
So what can be done? O’Hara thinks the burnout issue should be addressed early on, when future nurses are still in school. “I honestly believe the way to truly help nurses avoid burnout is to begin with a foundation of teaching while in school that stresses the importance of knowing yourself,” she says. “By that I mean your strengths and weaknesses. It should be taught that self-care must come first.”
Burger stresses the importance of taking regular breaks on the job. “If you’re not getting those breaks or they’re interrupted, then you don’t have the ability to refresh your spirit,” she says. “It sounds hokey, but it is true that you do need some brain downtime so that you could actually process the information you’ve been given.”
Tersigni, 63, now works part-time at a local hospital, specializing in the health and well-being of other nurses. She founded Yoga Nursing, a stress-management program combining deep breathing, quick stretches, affirmations, and relaxation and meditation techniques. “All of these can be done anytime throughout the day,” Tersigni says. “I even teach nurses to teach these to their patients. So the nurse breathes, stretches, and relaxes, while also teaching it to the patient.”
If you are a nursing student or new nurse, you are probably wondering what you will need in your work bag. Aside from your personal stuff, what are the things you bring that signifies you are a nurse?
These nursing supplies listed below are a must if you want to do your job efficiently.
The most common supplies nurses have in their bags are:
Stethoscope
This is one of the most important tools of the trade. Nurses use this tool to listen to things such as the heart, veins, and intestines to make sure proper function. According to Best Stethoscope Reviews, here are the 6 best stethoscopes to buy. As you surely know, it's one of the most important tools for a patient's assessment.
One of today's leading stethoscope brands is Littmann. You can choose from the classic style to the most advanced kind.
Books
A handy reference listing down common medicines and conditions. MIMS provides information on prescription and generic drugs, clinical guidelines, and patient advice. Nurses can also use Swearingen's Manual of Medical-Surgical Nursing, a complete guide to providing optimal patient care.
Scissorsand Micropore Medical Tape
Bandage scissors are used for cutting medical gauze, dressings, bandages and others. Nurses need to have these in their pockets for emergency use, especially for wound care. Micropore tape is also important and should be readily available, for example, when your patient accidentally pulls his/her IV.
Lotion and Hand Sanitizer
Nurses never forget to wash their hands several times throughout the day, leaving their skin dry. That's why having lotion in their bags is important to keep the skin in good condition. Meanwhile, the sanitizer helps nurses steer clear of germs, along with other contagious agents.
Six saline flushes
Retractable pens
Sanitary items - gauze, sterilized mask and gloves, cotton balls
OTC pharmacy items (cold medicines, ibuprofen and other emergency meds)
Small notebook - for taking notes from doctors and observations of your patients.
Thermometer
Tongue depressor
Torniquet
BP apparatus
Watch with seconds hand
On Nurse Nacole’s website, she shares that she carries a drug handbook, intravenous medications, makeup mirror, tape measure, towel, lotion, wipes, 4 in 1 pen and a homemade cheat sheet for her patients.
Also, in MissDMakeup's What's In My Work Bag Youtube video, she has a box of batteries, tapes, a pack of gum, toothbrush, sanitizer, coupons, snacks, umbrella, stethoscope, pens, folder of her report sheet and information sheet, tampons, charger, name tag, ID, makeup bag, eye drops, lotion, hair clips, highlighter, pen light, and journal.
So, What's in My Bag?
In my bag, I have a 4-in-1 pen, a highlighter, IDs, bandage, journal to write some new information when I surf the net, my phone with medical e-books and medical dictionary in it, and other stuff like alcohol, sanitizer, over-the-counter meds (such as paracetamol, cold medicine, pain killers, multivitamins), eye drops, handkerchiefs, floss, toothbrush, nail file, band aids, and food.
Aside from my knowledge in providing quality patient care, I also bring things that can help me get through my shift. In an effort to make things more compact and easy for a nurse to get access to, most common nursing supplies are available in a portable kit. The size and styles are developing as new ways of making a nurse's shift easier.
These are just few of the essential nursing paraphernalia that a new nurse needs.
Far from the sea, a man-made coral reef is taking shape -- and it could change medical operations forever.
Step inside the OkCoral lab in Israel's Negev Desert and you'll find row after row of quietly bubbling fish tanks, each containing a precious substance.
It is hoped the coral grown in this surreal "farm," could one day be used in bone operations -- encompassing everything from dental implants to spinal procedures.
Unlike animal and human bones, coral can't be rejected by the body, say medical experts at the company CoreBone, which manufactures bone replacements from coral.
Grown in the lab, this coral is also free from the diseases you might find in the oceanic variety.
Start-up science
Assaf Shaham founded the unusual laboratory six years ago at a cost of $2.5 million, with an ambitious vision of tapping into the billion dollar worldwide bone grafting industry.
But first he'll need the approval of authorities in the European Union and U.S., with a decision expected next year.
The father-of-two's dedication to the business is astounding -- if not a little disconcerting.
"In six years of growing corals, I haven't left these four walls for more than 12 hours -- not even once," he said.
"For me, it's 100% learning as I go. I take the mother colony, and I cut off a branch of the coral with a diamond saw. Then I glue it to another base made out of cement."
The delicate ecosystem needs constant care to ensure the water's salinity, temperature, and chemical make-up is perfect -- any variations and the coral could die.
The fish swimming around each tank are essentially the "worker bees" of the artificial reef. They eat the algae growing on the coral, their feces helps feed the coral, and finally, their movements in the water keep the coral strong.
And much like the traditional canary in the coalmine, if the fish die, you know something's not quite right in the water.
Clever company?
Happily for Shaham, his ambitious experiment appears to be thriving, with coral in the lab growing at ten times the normal rate.
Just a small container of the coral costs roughly $5 to $10 to produce, and sells for around $250.
One of the biggest benefits of the business is its environmental sustainability.
"We have a constant supply," says Ohad Schwartz of company CoreBone.
"We don't have to worry that in several years, harvesting from the sea could be forbidden."
It's a concern they'll never have to think about, when harvesting these remarkable fruits of the desert.
With the generous support of the Robert Wood Johnson Foundation and guided by a national advisory committee, a multidisciplinary team based at the University of Pennsylvania seeks to learn from clinicians or clinical leaders who are primarily responsible for transitional care services in health systems and communities throughout the United States. Specifically, the team is conducting a research study designed to better understand how transitional care services are being delivered in diverse organizations. Participation in this research survey is voluntary.
If you are a clinician or clinical leader responsible for transitional care service delivery in your organization, I encourage you to learn more about this study. To access the survey and more information on the study, please visit:
NAHN is happy to assist Dr. Mary Naylor and the University of Pennsylvania in this 2 year project. Dr. Mary Naylor will be providing NAHN with feedback on the survey results. If you know of others who have such responsibility within your association or work environment, please forward this email to them.
Thank you in advance for your consideration of this request.
There are a number of fantastic nursing blogs on the internet. Whether you’re an aspiring nurse, a working nurse, or a curious patient, you are sure to be entertained by these sites. We have narrowed down a list of the top 100 nursing blogs online to give you plenty of reading material for the future. Prepare yourself for hours of education and entertainment.
Top General Nursing Blogs
The Nursing Site Blog The Nursing Site Blog is just one of those sites that you have to read as a nurse. We love it because it constantly has new articles to read, from helpful advice to healthcare news and more. The blog is run by public health nurse Kathy Quan, RN. Kathy has been in the nursing industry for more than 30 years now, and you can see evidence of her experience on her site. Kathy has a Bachelor of Science in Nursing, and most of her working life has been spent in hospice and home health care. She shares her stories and lessons learned on her blog, along with other information that any nurse would love to read.
The National Nurse for Public Health The National Nurse for Public Health is a blog run by The National Nursing Network Organization. This is an organization that is working hard to create a better working environment for professionals in the public health industry. The blog provides news updates for work that the organization is doing, as well as other news from the nursing sector. The commentary on here comes from doctors, nurses, and other important workers in healthcare.
Scrubs Mag Scrubs Mag is considered the “The Nurses Guide to Good Living.” The name may sound like a catalog for working attire, but the information within this site is far from that. Scrubs Mag offers a wide range of helpful articles for new, existing, and future nurses, including style secrets to keep you looking great on the job. There are a number of writers who work for Scrubs Mag, so you can see everything from career advice to personal stories on the site. You can even sign up for free giveaways to get cool outfits, accessories, and tools to use on the job.
Confident Voices in Health Care Confident Voices in Health Care is a blog run by Beth Boynton. Beth is a published author and nurse consultant who specializes in communication and collaboration in the healthcare industry. What we love about Beth’s blog is the fact that it offers advice for patients and professionals alike to ensure that everyone works together in harmony. Many of Beth’s posts are about her medical improv workshops, where she helps healthcare workers become better speakers and listeners through improvisational training. Confident Voices also features articles from many a number of credible guest bloggers who share their insights into nursing and healthcare.
Nursetopia is a blog written for nurses by nurses. It is designed to honor these wonderful members of the healthcare world and showcase their influence on the modern world. The articles in the blog cover nursing news, career advice, business help, personal stories, art, freebies, and more. You always get a chance to see something different when you come here. Nursetopia is one of the most active blogs on our site, and it is one you will see in countless blogrolls from other bloggers on here. We’re subscribed to it for a reason.
Nurse Together Nurse Together is a fun and informative blog run by a team of nurses. The bloggers here range from nurse educators to RNs and beyond. While we may love the site for its blog-like articles, Nurse Together also offers a job board, nursing school guide, discussion panel, and much more. The Nurse Together Facebook page has more than 21,000 fans, showing just how much people love visiting this site. There are new blog posts on here every day, so you can always look forward to something new to read.
Lippincott’s Nursing Center Lippincott’s Nursing Center is a site dedicated to helping nurses be the best workers they can be. The site is home to more than 50 nursing journals online, including the American Journal of Nursing, Nursing2014, Nursing Management and The Nurse Practitioner: The American Journal of Primary Health Care. In addition to these peer reviewed journals, Lippincott’s Nursing Center features more than 1,300 continuing education activities for nurses, making it easy to maintain a career as a nurse here. The authors on the site are mostly advanced practice nurses and registered nurses who share their career expertise with the world.
Off the Charts Off the Charts is a product of the American Journal of Nursing. It mostly provides news updates and research study reports for the nursing community. With this in mind, you can also find a number of helpful career advice articles on this site. Some popular categories for posts on here include patient engagement, healthcare, medical prices, nursing research, nursing perspective, and more. Off the Charts is authored by a number of nursing professionals, most of whom have a graduate level education. The blog commonly highlights influential nurses from the past to inspire nurses of the future.
Not Nurse Ratched Not Nurse Ratched is a wonderful nursing blog that has been around since 2007. The blog is run by a writer, nurse, and medical editor who enjoys “investigating ways to save time.” The articles on here fit into categories like applications, gadgets, technology, personal, medical, humor, and more. Most of the articles are written with a great sense of humor, which is sometimes hard to find in healthcare blogs.
Nursing Stories Nursing Stories is a heartfelt blog about one woman’s experiences in nursing. Marianna Crane, the blogger, has been in nursing for over 40 years, and she now uses her blog to share her stories from the past and present. She has been a certified adult nurse practitioner since 1981, and she has a passion for writing that is evident in her blog posts. Marianna says, “My goal for this blog is to encourage nurses to boast.” You can get inspired to be a better nurse thanks to this woman and the great stories she shares on her blog.
The Nursing Show The Nursing Show is more than just a blog. It is a compilation of entertaining videos about nursing. Each episode teaches a new lesson about this ever-changing career, from getting through college to dealing with tough patients. The episodes are included in short, easy-to-read articles that summarize what the videos are about. There are already more than 300 episodes of The Nursing Show for you to watch, so you don’t have to worry about getting bored on this site.
Advances in Nurse Science Blog The Advances in Nurse Science Blog is tied to a nursing publication that comes out four times a year (appropriately titled Advances in Nursing Science). The blog allows readers to discuss big issues that are mentioned in ANS so that they can understand and expand upon these ideas. The ANS journal was founded back in 1978 by Peggy L. Chinn, RN, PhD, FAAN. It has been in publication ever since, but the blog was a much more recent addition to the ANS world.
Reality RN Reality RN is a pretty interesting blog because it is run entirely by new nurses. You may not think these men and women have a lot to share about their experiences, but they convey what “reality” is like for people who are new to this profession. If you are a nursing student worried about what you might be getting yourself into, this blog should be able to answer all of your questions. Best of all, there is a great list of “must read” blogs on the home page that link to even more top nursing blogs online.
AllTop – Nursing This site doesn’t exactly fit the “norm,” but we thought it was important to put it on our list. Essentially AllTop is just a directory for other websites, but it shows you the most recent posts from many nursing blogs online. It’s a one-stop-shop for nursing tips and news online, and it features the work of several other sites on our top 100 nursing blogs list. If you want to stay updated on other topics from around the web, AllTop has plenty of other categories for you to explore.
Diversity Nursing Diversity Nursing offers a number of helpful articles and services for nursing professionals. The blog on the site features news information and career tips for nurses, but the site as a whole has a job board, college guide, and much more. There is even a forum on the site where nurses, patients, and nursing students can discuss important issues in healthcare. Diversity Nursing started off as a basic job board back in 2007, but it has grown to be so much more since then. You can even use this site to post a resume so you might get a better job in the future. Here is a look at some memorable posts from the Diversity Nursing blog:
Nursing Ideas Nursing Ideas is a blog that covers a variety of variety of nursing related topics. The blog was started back in 2008 as an online resource for nursing students. Rob Fraser, the blog’s founder, began writing articles for the blog while he was an undergraduate nursing student at Ryerson University. In 2013, Rob refocused the blog to be more about professional interviews so that his readers could see what life is really like as a nurse in today’s world.
Soliant Health is a healthcare staffing company that offers some great advice for nursing professionals around the country. You don’t have to be a member of the Soliant Health network to benefit from the articles on their blog. Even if you already have a job as a nurse, you could learn from some of the news articles and tips on the blog. If you are in fact looking for a job, you can look through the job board on Soliant Health to see what opportunities may be available for you.
Nursing Daily Nursing Daily is a fairly new blog, especially compared to other sites on our list. Nevertheless, it has already developed a great reputation in the nursing community, and we’re hoping it sticks around for years to come. Nursing Daily is dedicated to providing “nursing tips, advice, and humor” for anyone who wants to read it. Many of the posts on here are quick, simple images that will make you chuckle a little about life as a nurse.
The Nurse Path The Nurse Path is a beautiful, entertaining, and inspiring blog that is dedicated entirely to nurses. The blog features a number of categories, including: nurse mind, nursing skills, health and fitness, technology, funnybone, and more. The motto for this site is “helping nurses find the way,” and every article here is evidently doing just that. You’ll find at least one new post a week on this blog to read and learn from, so this is definitely worth putting in your RSS reader.
Living Sublime Wellness Living Sublime Wellness is a blog dedicated to transforming the nursing community for the better. The blog is authored by Elizabeth Scala, an RN with an MSN/MBA and years of working experience as a nurse. Elizabeth is a public speaker who visits nursing associations, hospitals, and other healthcare organizations to teach people what they can do to make their working environments better for nurses. Living Sublime Wellness features a lot of great resources for current and future nurses, making it a great site to visit no matter where you are in your career.
RTConnections Nurse Blog The RTConnections Nurse Blog is designed to connect all members of the nursing world so they can educate and inspire one another to do better in their careers. This blog is particularly beneficial for new nurses because they can read stories from experienced professionals that they may aspire to become. One of the big focuses on this blog is nurse bullying, which has become a hot topic of discussion over the last few years. You can learn ways to avoid and prevent bullying in the work place by reading some of the posts on RTConnections.
Dear Nurses Dear Nurses is essentially a portal for several sites under the “Dear Nurses” umbrella. These sites are all focused on educating nurses through captivating illustrations. Dear Nurses combines simple graphics with helpful information to show nurses how to improve their skills and services. It also contains multi-part educational series that expand upon other posts they have on their sites. Dear Nurses has been online since 2006, and it has grown significantly in that time.
Your Career Nursing Your Career Nursing is centered around the idea of helping nurses improve their careers. The articles here teach nurses of all stages about the skills and processes they need to succeed in this profession. There are several categories of posts to choose from here, including education, entrepreneurship, lifestyle, networking, nursing success stories, online learning, unique nursing jobs, and more. No matter who you are, you can find something to like here.
We live in a high-stress world. Between having to attend to work, kids, homes and run back and forth between meetings and all of the other demands of everyday life, to say that things can get stressful is an understatement.
If your constant on-the-go lifestyle has left you feeling run down, beat down and just plain old exhausted, then you need to stop and smell the proverbial roses for a little bit.
Taking time to enjoy something that is peaceful and that is just for you can do wonders for your health, your mental clarity and for your happiness. You don’t have to invest much time in such activities, either; reserving just 30 minutes a day to something that you enjoy and that promotes a bit of peacefulness and tranquility can do wonders.
Here’s a look at some activities that you can do for just 30 minutes a day and that will provide you with some simply amazing benefits.
Yoga: It seems like yoga is all the rage in the fitness world as of late (well, not really as of late; it’s been a trend for quite a while) – and there’s a reason why; yoga provides some pretty amazing benefits.
Just 30 minutes of yoga a day will help to increase your strength and flexibility, as well as tone your body. In addition to physical benefits, yoga can also increase your brain function. A recent study conducted by the University of Illinois found that people who participated in just 20 minutes of yoga a day experienced an increase in the speed and accuracy of their brain functions. Yoga also helps to reduce stress levels and boosts mental clarity; talk about some pretty amazing benefits for just 30 minutes of your time each day.
Meditation: Another activity that can provide fantastic benefits in just 30 minutes a day is meditation. When you think of people meditating, what comes to mind? People who are more peaceful, more astute and have more clarity? If so, there’s a good reason why – Because meditation helps to promote all of these things.
In fact, just 30 minutes of meditating a day can boost your creative thinking abilities, heighten your energy levels, decrease your stress levels and even ease the feelings of depression.
A Long Walk: If someone tells you to ‘go take a walk’, take them up on it! There are so many wonderful benefits associated with walking, and the best part is, it is so easy to do. Walking for just 30 minutes a day improves your cardiovascular health, decreases stress and anxiety, helps to keep off excess weight, tones muscles, boosts energy levels and it can even help to decrease your risk of dementia. Walking also just makes you happy. So kick off those painfulwork shoes and dust off your sneakers, and get moving. There is nothing more therapeutic than soaking up the warm sunshine and observing the beauty of nature while walking on a nice day.
Reading: Everyone knows that reading is important, but do you know why? Reading for just 30 minutes each day can increase your vocabulary, boost your creative thinking and critical thinking skills, stimulate your mind, improve your memory and focus and decrease stress levels. So, when you’re feeling like you just need to escape for a little while, curl up with a book or a magazine and submerse yourself in reading.
No matter how crazy your lifestyle is, you can spare just 30 minutes a day to enjoy the benefits that one of these activities can provide. You’ll be amazed by how much happier you will feel – you owe it to yourself!
Earlier this week, Brian Shepherd sat down in a small doctor's office in Bethesda, Maryland. A technician swabbed his arm and gave him a quick jab with a needle.
With that, Shepherd became subject No. 13 in the experiment testing a potential Ebola vaccine.
The trial was launched on an emergency basis earlier this month by the National Institute on Allergy and Infectious Disease. It's the first to test this kind of Ebola vaccine in humans.
"It's not just for the money," Shepherd wrote in a Reddit AMA. "I'm very interested in translational research and experiencing it from the guinea pig side is very rewarding. But yeah, the money helps. This one study will fund most of my grad school application costs, though not in time for application season."
The vaccine doesn't use live virus and can't infect volunteers with Ebola. Instead it uses specific Ebola proteins to trigger an immune response. They're delivered through the body on a modified version of an adenovirus, a type of cold virus.
In the initial phase, 10 healthy volunteers were given a low dose of vaccine. They were monitored for side effects and tested to see if their bodies are producing antibodies. In the second phase, of which Brian is a part, an additional 10 volunteers are being given a higher dose.
All participants will be followed for nearly a year and tested at regular intervals.
Shepherd, who has volunteered for several prior research studies at NIH, spoke with CNN about his experience.
The following is a condensed version of that conversation:
CNN: How did you come to join the study?
BrianShepherd: I actually work at NIH; I'm a post-doc researcher in a developmental biology lab. Most trials I learn about from reading a ListServ (email list).
I heard about the vaccine study from going to preliminary meetings for a different study.
CNN: When was this?
Shepherd:Less than a month ago. I had my first appointment on August 26. It was just a sit-down, to talk about the trial, go through paperwork and consent forms, explaining what the trial was for. Then they did an initial run-through of my health history.
CNN: What was next?
Shepherd:The next week I had my second appointment. They did a full physical, blood work, health history, breathing checks. A lot of poking and prodding. My third visit was Wednesday. They drew blood, then gave me a shot. Now, my next appointment is Sunday.
CNN: What was it like? You wrote that pulling off the Band-aid was the worst of the pain.
Shepherd:I'm supposed to keep a daily diary for the first seven days, logging my temperature and any symptoms. The next morning, I woke up with a slight fever, 100.5. I took some Tylenol and it went away.
Other than that I feel fine. In fact, I ran a half-mile in a relay race at lunchtime with some people from work.
CNN: You wrote that for each of these regular visits, you're paid $175. How many times have you been a human guinea pig?
Shepherd:This is my second drug trial. Before that, I did mostly MRI studies.
The first one I did, I was in the MRI machine and had three tasks. They gave me two buttons and showed pictures. If it was Spiderman, I'd hit one button; if it was the Green Goblin, I'd hit the other. So I spent 15 minutes playing Spiderman vs. Green Goblin.
CNN: Did you have any reservation at all, taking part in this Ebola vaccine trial?
Wearable tech is all the rage right now, with Google Glass and now the Apple Watch being gadget fiends' latest must-have items. Electronic activity monitors may be the most popular example of health-monitoring wearable technology. A new analysis from researchers at the University of Texas Medical Branch at Galveston - published in the Journal of Medical Internet Research - compared 13 of these devices.
"Despite their rising popularity, little is known about how these monitors differ from one another, what options they provide in their applications and how these options may impact their effectiveness," says Elizabeth Lyons, senior author of the new study and assistant professor at the Institute for Translational Sciences at the university.
"The feedback provided by these devices can be as, if not more, comprehensive than that provided by health care professionals," she adds.
Lyons and her colleagues assessed 13 wearable activity monitors available on the consumer market. The team wanted to see how the devices may promote healthy and fit behaviors and determine how closely they match successful interventions.
The researchers also compared the functionality of the devices and their apps with clinical recommendations from health care professionals.
In their analysis, the researchers write that most of the goal-setting, self-monitoring and feedback tools in the apps bundled with the devices were consistent with the recommendations health care professionals make for their patients when promoting increase in physical activity.
Despite this, the analysis also finds that some proven successful strategies for increasing physical activity were absent from the monitors. These included:
Action planning
Instruction on how to do the behavior
Commitment and problem solving.
Interestingly, though, the authors suggest that the apps with the most features may not be as useful as apps with fewer - but more effective - tools.
The researchers also consider that how successful any monitor is largely depends on matching individual preferences and needs to the functionality of the device. For instance, someone who gets most of their exercise from swimming will benefit the most from having a waterproof monitor.
Applications for activity monitors beyond aiding weight loss?
The report also contains suggestions on applications for these monitors outside of their typical role as weight loss aids.
For instance, the researchers suggest the wearable activity monitors could be useful for patients who have been released from the hospital. These patients could use the monitors to measure their recovery and quality of life.
Also, health care professionals could use data from the monitors to identify at-risk patients for secondary prevention and rehabilitation purposes.
Lyons says:
"This content analysis provides preliminary information as to what these devices are capable of, laying a foundation for clinical, public health and rehabilitation applications. Future studies are needed to further investigate new types of electronic activity monitors and to test their feasibility, acceptability and ultimately their public health impact."
The study only looked at devices compatible with personal computers and iOS mobile devices, and the researchers admit it is possible "the experiences of Android users may differ from our experiences."
Growing up, Adriana Perez experienced the kinds of challenges that are at the core of the immigrant experience in America. She learned English as a second language, attended underperforming public schools in a small town, and struggled to pay for college because her parents—who were farmworkers—couldn’t afford to send her.
Through it all, Perez focused on the gifts she received during her upbringing: love and support from her family, guidance from her teachers and mentors, a strong work ethic derived from a culture that values hard work, and a personal drive to make a difference in her community.
When she reached adulthood, she made an unusual choice—at least for her demographic group: She became a nurse. Now an assistant professor of nursing at Arizona State University, Perez, PhD, ANP, is a member of the most underrepresented racial or ethnic group in nursing.
In 2013, Latinos comprised 3 percent of the nation’s nursing workforce, according to a survey by the National Council of State Boards of Nursing and the National Forum of State Workforce Centers, and 17 percent of the nation’s population, according to a U.S. Census Bureau fact sheet. And their numbers are growing: By 2060, Latinos are projected to comprise nearly one-third of the U.S. population. But their growth in nursing has been slow, Perez said.
Recruiting more Latino nurses is about more than parity in the nursing workforce; it’s about improving health and health care for Latinos, who have disproportionately high rates of HIV transmission, teen pregnancy, and chronic conditions like obesity and diabetes, according to data compiled by the Centers for Disease Control and Prevention. Latinos also are less likely to have health care coverage than other racial or ethnic groups.
More Latino nurses can help narrow disparities, experts say, because they are more likely to be able to provide culturally and linguistically appropriate care to Latino patients. “Having a culturally competent nurse really makes a difference in terms of compliance and patient outcomes,” said Elias Provencio-Vasquez, PhD, RN, FAAN, FAANP, dean of the nursing school at the University of Texas at El Paso and an alumnus of the Robert Wood Johnson Foundation (RWJF) Executive Nurse Fellows program (2009-2012). “Patients really respond when they have a provider who understands their culture.”
The Institute of Medicine (IOM)—the esteemed arm of the National Academy of Sciences that advises the nation’s leading decision-makers on matters relating to health and medicine—agrees. In 2004, it published a report calling for a more diverse health care workforce to improve quality and access to care and to narrow racial and ethnic health disparities. And in 2010, the IOM released a report that included calls for greater diversity within the nursing profession in particular.
Latinos Aren’t Flocking to Nursing
Yet despite their growing numbers, Latinos are not flocking en masse to the nursing profession.
That’s in large part because of inequity in education, said Dan Suarez, BSN, MA, president of the National Association of Hispanic Nurses. “Many Latinos come from poor educational systems, and few concentrate on the kinds of science and math courses that are needed to enter nursing school. Latinos have the highest high school drop-out rate in the nation, and many students are just focused on staying in school and making it to graduation.”
Meanwhile, there are relatively few Latino nurse leaders and educators who can serve as role models, coaches and mentors to the next generation of nurses, Perez said. “When young people aren’t able to see themselves in those roles, it’s hard to imagine that they could be in that role.”
Language and culture also play a role. Latino parents often discourage Latino youth—and especially boys—from pursuing nursing because it is regarded as a low-status, low-pay service job in Mexico and parts of Latino America, Suarez said. “Parents tell their children they can do better than nursing ... Nursing has an image problem, and we’re trying to change that.”
The culture’s emphasis on traditional gender roles also discourages Latina wives and mothers from working outside the home and, if they do, from pursuing leadership positions, said Mary Lou de Leon Siantz, PhD, RN, FAAN, a professor at the Betty Irene Moore School of Nursing at UC Davis and an RWJF Executive Nurse Fellows program alumna (2004-2007). “The majority of Latina nurses go into associate degree programs and don’t see the need to go back for more education.”
Racism against Latinos, she added, is “full-blown,” especially amid the national debate over immigration. Academics and others retain unconscious biases against Latinos and members of other groups that are underrepresented in nursing.
RWJF is committed to increasing diversity in nursing through programs such as New Careers in Nursing, which works to increase the diversity of nursing professionals to help alleviate the nursing shortage, and the RWJF Nursing and Health Policy Collaborative at the University of New Mexico, which prepares nurses, especially those from underserved populations in the Southwest, to become distinguished leaders in health policy. The Future of Nursing: Campaign for Action, a joint initiative of RWJF and AARP, is working to diversify the nursing workforce, with help from Perez and others. The National Association of Hispanic Nurses, meanwhile, offers scholarships to Latino nursing students.
But more needs to be done, Siantz and others said. Educational bridge programs to help students transition into nursing school are needed, as are interventions to dispel negative stereotypes about nursing among Latinos and increased mentorship for aspiring nurses and nursing students. “Latino nurses often talk about the influence of a family member, or a role model, or a mentor who told them to be a nurse,” said Perez, whose grandmother, a nurse in Mexico, encouraged her to pursue nursing in the United States. “We need to do more of that kind of outreach.”
Here's a light-hearted look at cancer treatment from the point of view of my son Elliot, who was only 4 1/2 when he was diagnosed. I know many of the adults I am in touch with who have cancer or who are helping a person with cancer through this journey, will relate!
Advice to adults with cancer from a 5-year-old:
1. It is perfectly acceptable to have a complete tantrum and throw your shoes around just before leaving for the hospital.
2. You always deserve a present after chemo.
3. If you feel like showing more respect and politeness to the hospital clown than your oncologist, that's OK.
4. If you manage to grab the syringe of medicine from the nurse, it's their loss and you are then allowed to squirt its entire content around the room.
5. You are allowed to complain loudly about any smells like perfume, but you are also allowed to fart freely whenever and wherever you want.
6. Anyone who says "this one tastes like syrup" better be not be lying or they can expect to catch some spit.
7. You are allowed to worry about life and death, but only to the same extent that you worry about whether Santa Claus will be able enter your home if you don't have a chimney.
8. Speaking of worry, you are not allowed to worry about anything that is not going to happen today or tomorrow.
9. Any bad thing that happened in the past should be quickly erased from your mind using ice cream.
10. It's OK to throw up directly on your caregiver instead of into the bucket they are holding. It will create warm and funny memories for them once this is all over.
11. Good friends may stare when they first see you without any hair, but they are quickly more interested in all your new toys. So make sure you have lots of new toys around all the time.
12. It is the right thing to do to jump off the examining table if the doctor's hands are too cold.
13. A popsicle for breakfast is a good idea and goes well with bacon.
14. If someone rubs your bald head and says you're cute, you should stare at them in complete boredom until they stop.
15. Always believe that scars are badges of courage and make you look like a pirate or a superhero.
16. Jumping on the bed is a perfectly acceptable form of exercise.
17. Someone should always be available to carry you if you don't feel like walking anymore and they will be grateful if you look at them lovingly and say, "You're walking too slowly."
18. It's a good idea to frequently press the little button next to the bed that makes the nurse come running, because she might be lonely and bored and enjoys picking your crayon up from the floor.
19. The only part of hospital food you should eat is the dessert. The rest is not really food, anyway.
20. Make having fun your priority all the time, no matter where you are or what's going to happen next.
How do you pass the time when cancer treatment means you're largely confined to your hospital room for weeks on end?
Tom Gillin, a 19-year-old college student, chose a less-than-obvious choice: He filmed a funny rap video channeling Jay-Z via the cancer ward.
"Some of the other videos I've seen about cancer patients are somewhat depressing," said Gillin, who was diagnosed with the pediatric cancer acute myeloid leukemia in April. "We wanted to flip the switch and do something that was the opposite of that."
Gillin teamed with several staffers at The Children's Hospital of Philadelphia to create "Bald So Hard." The video's title refers to Gillin's chemotherapy-related hair loss but is also a play on the phrase "ball so hard" featured prominently in a hit song by Jay-Z and Kanye West. The song is parodied in Gillin's video, as is Jay-Z's "Empire State of Mind."
The rollicking video — promoted on Twitter with the hashtag #BaldSoHard — is full of swagger. Gillin is seen mouthing lyrics such as "bald so hard my head got shiny" while dancing with his oncologist, playing basketball and even steering a "boat," a cardboard cutout made by hospital art therapist Abbien Crowley. (The actual rap was performed, mostly off camera, by University of Pennsylvania medical student David Blitzer.)
But Gillin didn't shy away from the fatigue and boredom confronting hospital cancer patients. It took him and his hospital pals some two months to complete the three-minute video since chemotherapy treatments often left him too weak to shoot.
The song's lyrics, written by Gillin and CHOP music therapist Mike Mahoney, manage to make light of it: "They gave me sleeping meds all day and I was dozing/When I got up I was so bored that I watched 'Frozen.'"
Gillin said his main motivation for making the video was to raise awareness of pediatric cancer, though he'd also appreciate it if Jay-Z — one of the teen's favorite rappers — took note of the unusual homage and paid the hospital a visit.
But don't expect Gillin to use the video to launch his own hip hop career. "I'm not that musically inclined," he insists.
Instead, he's looking forward to completing his final round of chemotherapy in a couple of weeks and ultimately returning to student life at the University of California, Los Angeles, where he's studying civil engineering.
For now, he's enjoying the happy reactions to his video, which has generated more than 20,000 views on YouTube since it debuted late last month. The Jigga Man himself hasn't yet weighed in but plenty of others say they love Gillin's jam, with one YouTube user dubbing it "best medicine in the world."
It's the mother of all hackathons — a group of MIT researchers are bringing together engineers, designers, health experts and parents with the goal of building a better breast pump. "We really want to bring the breast pump out of the lactation closet," said Alexis Hope, a research assistant at the MIT Media Lab. "If you talk to moms about something that makes the first part of having a baby miserable, they always say the breast pump. They're loud, they have a million parts, they're impossible to clean, heavy. They're completely impractical for the realities of your life."
In May, a small group from the lab came together to brainstorm, and a blog post about their efforts drew so much interest the organizers — who include four moms — decided to expand. They expect up to 80 people to join forces Sept. 20 and 21 and work all weekend "to make the breast pump not suck." Participants will split into five-person teams and then pitch their prototypes to the group at the end. Hope said it's "just a starting point," but ideally some of the innovations will catch the eye of pump manufacturers.
Half of all new moms in the United States now breastfeed for the six months recommended by pediatricians. Many of them use pumps to produce milk for when they return to work or are away from the baby. Studies have shown breast milk and nursing has health benefits for both the infant and the mother.
For three young siblings, eating is a life or death proposition, thanks to a rare white blood cell disease, reported KSL.
The Frisk children— Jaxen, age 9; Tieler, age 7; Boston, age 4— have spent weeks in the hospital and are allergic to pets, pollens and multiple foods. The siblings all have eosinophilic gastrointestinal disorder (EGID), an abnormal build-up of eosinophil white blood cells in their GI tracts that can cause inflammation and tissue damage in response to foods and allergens. While the disease is relatively rare, it has increased in prevalence over the past decade affecting one in 2,000 people, according to the American Partnership for Eosinophilic Disorders.
"You need food to survive. But it is also what can kill you in our house," their mother, Jenny Frisk, told KSL.
When they’re exposed to their triggers, the children could have an anaphylactic reaction— potentially fatal allergic symptoms throughout the body.
"Tieler had one sip of milk when she was 1-year-old, and instantly started projectile vomiting and got hives all over her body," her father, Gary, told KSL. "It's a life and death situation at birthday parties, or religious events, or anywhere we go, because food is such a big part of our culture."
Between the three children, they’ve endured 11 surgeries and eight extended hospital stays, with more expected in the future.
On top of the children’s health issues, Gary battled cancer two years ago and Jenny had to have several surgeries due to serious adrenal insufficiencies that were unrelated to EGID.
The family has been bankrupted twice by medical bills. While they make too much income to qualify for help, they don’t make enough to pay for their children’s medical needs. Friends and family have started a GoFundMe account to raise money to pay for genetic testing and treatment.
"When we're looking at an illness that is not curable, and the treatment isn't covered (by insurance), the light at the end of the tunnel is really far away," Jenny said.
Recently, Medical News Today reported on a breakthrough in xenotransplantation - the science of transplanting functional organs from one species to another. Scientists from the Cardiothoracic Surgery Research Program of the National Heart, Lung and Blood Institute (NHLBI) demonstrated success in keeping genetically engineered piglet hearts alive in the abdomens of baboons for more than a year.
While that is a sentence that might sound absurd, or even nightmarish to some, xenotransplantation is a credible science involving the work of leading scientists and respected organizations like the NHLBI and the Mayo Clinic, as well as large private pharmaceutical firms such as United Therapeutics and Novartis.
What is more, xenotransplantation is not a new science, with experiments in cross-species blood transfusion dating as far back as the 17th century.
Why transplant the organs of animals into living humans?
The reason why xenotransplantation is a burning issue is very simple: because of a crippling shortage of available organs for patients who require transplants, many people are left to die.
US Government information on transplantation reports that an average of 79 people receive organ transplants every day, but that 18 people die each day because of a shortage of organs.
The number of people requiring an organ donation in the US has witnessed a more than five-fold increase in the past 2 decades - from 23,198 in 1991 to 121,272 in 2013. Over the same period, the number of people willing to donate has only doubled - 6,953 donors in 1991, compared with 14,257 donors in 2013.
Although some researchers are attempting to solve this shortage by developing mechanical components that could assist failing organs, these devices are considered to increase the risk of infection, blood clots and bleeding in the patient.
Stem cell research is also actively pursuing the goal of growing replacement organs, but despite regular news of breakthroughs, the reality of a functional lab-grown human organ fit for transplant is a long way off.
As the NHLBI's Dr. Muhammad M. Mohiuddin, who led the team responsible for the baboon trial, explained:
"Until we learn to grow organs via tissue engineering, which is unlikely in the near future, xenotransplantation seems to be a valid approach to supplement human organ availability. Despite many setbacks over the years, recent genetic and immunologic advancements have helped revitalized progress in the xenotransplantation field.
Xenotransplantation could help to compensate for the shortage of human organs available for transplant."
Xenotransplantation's eccentric history
The earliest known example of using animal body parts to replace diseased or faulty components of human bodies dates back to the 17th century, when Jean Baptiste Denis initiated the clinical practice of animal-to-human blood transfusion.
Perhaps predictably, the results were not successful and xenotransfusion was banned in Denis' native France.
Fast forward to the 19th century and a fairly unusual trend for skin xenotransplantation had emerged. Animals as varied as sheep, rabbits, dogs, cats, rats, chickens and pigeons were called upon to donate their skin, but the grafting process was not for the squeamish.
Medical records show that, in order for the xenosurgeons of the time to be satisfied that the donor skin had vascularized (developed capillaries), the living donor animal would usually have to be strapped to the patient for several days. However, the most popular skin donor - the frog - was typically skinned alive and then immediately grafted onto the patient.
Despite several reputed successes, modern physicians are skeptical that these skin grafts could have been in any way beneficial to the patient.
The first corneal xenotransplantation - where the cornea from a pig was implanted in a human patient - took place as early as 1838. However, scientists would not look seriously again at the potential for xenotransplantation until the 20th century and the first successes in human-to-human organ transplantation.
In 1907, the Nobel prize-winning surgeon Alexis Carrel - whose work on blood vessels made organ transplantation viable for the first time - wrote:
"The ideal method would be to transplant in man organs of animals easy to secure and operate on, such as hogs, for instance. But it would in all probability be necessary to immunize organs of the hog against the human serum. The future of transplantation of organs for therapeutic purposes depends on the feasibility of hetero [xeno] transplantation."
These words have been described as "prophetic" because Carrel is describing the exact line of research adopted by xenotransplantation scientists a century later.
A few years later, another leading scientist, Serge Voronoff, would also predict modern science's interest in using the pancreatic islets of pigs to treat severe type 1 diabetes in human patients. However, other xeno experiments by Voronoff have not endured critical reappraisal quite so well.
Voronoff's main scientific interest was in restoring the "zest for life" of elderly men. His attempt to reverse this element of the aging process was to transplant slices of chimpanzee or baboon testicle into the testicles of his elderly patients.
Incredibly, this surgery proved quite popular, with several hundred operations taking place during the 1920s in both the US and Europe.
By the 1960s, despite limited availability, the transplantation of kidneys from deceased to living humans had been established by French and American surgeons.
Dialysis was not yet in practice and given that, in the absence of an available donor kidney, his renal failure patients were facing certain death, the Louisiana surgeon Keith Reemtsma took the unprecedented step of transplanting animal kidneys. He chose chimpanzees as the donor animals, due to their close evolutionary relationship with humans.
Although 12 of his 13 chimpanzee-to-human transplants resulted in either organ rejection or infectious complications within 2 months, one patient of Reemtsma continued to live and work in good health for 9 months, before dying suddenly from acute electrolyte disturbance. Autopsy showed that the chimpanzee kidneys had not been rejected and were working normally.
Experiments in the xenotransplantation of essential organs continued in living patients until the 1980s - without lasting success. However, the procedures attracted widespread publicity, with some attributing a subsequent rise in organ donation to the failed attempt to transplant a baboon heart into a baby girl in 1983.
Where does research currently stand?
Despite the more obvious similarities between humans and other primates, pigs are now considered to be the most viable donor animal for xenotransplantation.
Despite diverging from humans on the evolutionary scale about 80 million years ago, whole genome sequencing of the pig has shown that humans and pigs share similar DNA, while the pig's organs - in size and function - are anatomically comparable to humans.
However, perhaps the main advantage of the pig as donor is in its availability - potentially providing an "unlimited supply" of donor organs. If transplantation is viable, pig donors would provide an immediate solution for the organ shortage problem.
Xenotransplantation optimists also believe that the process can improve on the existing success rate of transplantation of human organs. By keeping the pigs healthy, regularly monitored for infection, and alive right until the point when the required organs are excised under anesthesia, the adverse effects associated with transplantation from deceased donors - such as non-function of organs or transmission of pathogens - would be much less likely, this group argues.
However, there are still significant scientific barriers to the successful implementation of xenotransplantation.
The company United Therapeutics - who moved into xenotransplantation research after the daughter of CEO Martine Rothblatt was diagnosed with pulmonary hypertension, a condition with a 90% shortage rate of available lung donors - claim to be making progress with eliminating these barriers.
MedIcal News Today spoke to Rothblatt, who once claimed that the company will have successfully transplanted a pig lung into a human patient "before the end of the decade."
"For a first clinical trial, which was my goal, I think we are on track," she told us. "I said our goal by end of decade is to transplant a xeno lung into a patient with end-stage lung disease and bring them safely back to health."
As well as pioneering lung xenotransplants, the company has ambitions of making pig kidneys, livers, hearts and corneas available for human transplant.
"All are years away, but lung may well be most difficult," admits Rothblatt. "We call it the canary in the coal mine."
In order to make pig lungs compatible with humans, Rothblatt has estimated that 12 modifications need to be made to the pig genome that will prevent rejection. She claims United Therapeutics have now succeeded in making six of these genome modifications.
Also, it was United Therapeutics' genetically modified piglets that provided the world record-beating pig hearts for the NHLBI study in baboons.
Opposition to xenotransplantation
However, science is not the only obstacle to xenotransplantation. Despite clearing all steps of the research with ethics committees at every step, Rothblatt - who has a doctorate in medical ethics - admits there will be unforeseeable regulatory dilemmas and ethics conversations before xenotransplantation can be accepted into clinical practice.
In 2004, the UK's Policy Studies Institute conducted the first major survey of public attitudes towards potential solutions for the organ shortage crisis. The public perception of xenotransplantation was shown to be overwhelmingly negative.
Indeed, response to animal-to-human transplantation was so hostile that some respondents demanded that it be removed as an option on the survey. Although many respondents considered xenotransplantation unethical, the major concern was that animal viruses could infect humans and spread into the population.
Following the survey, an intriguing debate over the ethics of xenotransplantation took place in the pages of Philosophy Now. Making the case against xenotransplantation, Laura Purdy - professor emerita of philosophy at Wells College in Aurora, NY - commented that "the xeno debate proceeds as if saving lives is our top moral priority." She argues that, from this perspective, it suggests that the lives lost down the line as a result of perfecting xenotransplantation do not count.
"What about the 11 million babies and children who die every year from diarrhea, malaria, measles, pneumonia, AIDS and malnutrition?" she questioned. "What about the half-million women who die every year during pregnancy and childbirth when simple measures could save most of them?"
We asked Prof. Purdy why the fact that people die from matters unrelated to transplantation issues would morally preclude science from attempting to also solve the issue of organ donor shortages.
"I agree that, other things being equal, saying that people are dying from other causes doesn't show why we should not also tackle this cause," she replied.
"But once one has taken on board the larger risks to society, both from the research as well as the deployment of the technology, as well as the probability that this is merely a bridge technology that, hopefully will be made obsolete by future developments (such as partial or whole artificial hearts) or advances in public health (making headway against diabetes) and the probability that both research and implementation will be very expensive, that seriously erodes the case for proceeding.
Resources for health are far from infinite. There is a great deal that we could be doing now to advance human health that does not have these downsides - why not focus more there?"
Whether public attitudes toward xenotransplantation have mellowed in the decade since the Policy Studies Institute's survey is not currently known.
However, as the technology advances and the likelihood of implementation draws closer, so too must the public conversation over the perceived rights and wrongs of animal organ transplantation advance in order to hold the science accountable.
Do you have a view on this issue? If so, use our comments box to join the debate.
Pediatricians prescribe antibiotics about twice as often as they're actually needed for children with ear and throat infections, a new study indicates.
More than 11 million antibiotic prescriptions written each year for children and teens may be unnecessary, according to researchers from University of Washington and Seattle Children's Hospital. This excess antibiotic use not only fails to eradicate children's viral illnesses, researchers said, but supports the dangerous evolution of bacteria toward antibiotic resistance.
"I think it's well-known that we prescribers overprescribe antibiotics, and our intent was to put a number on how often we're doing that," said study author Dr. Matthew Kronman, an assistant professor of infectious diseases at Seattle Children's Hospital.
"But as we found out, there's really been no change in this [situation] over the last decade," added Kronman. "And we don't have easily available tools in the real-world setting to discriminate between infections caused by bacteria or viruses."
The study was published online on Sept. 15 in the journal Pediatrics.
Antibiotics, drugs that kill bacteria or stop them from reproducing, are effective only for bacterial infections, not viruses. But because doctors have few ways of distinguishing between viral or bacterial infections, antibiotics are often a default treatment.
To determine antibiotic prescribing rates, Kronman and his colleagues analyzed a group of English-language studies published between 2000 and 2011 and data on children 18 and younger who were examined in outpatient clinics.
Based on the prevalence of bacteria in ear and throat infections and the introduction of a pneumococcal vaccine that prevents many bacterial infections, the researchers estimated that about 27 percent of U.S. children with infections of the ear, sinus area, throat or upper respiratory tract had illnesses caused by bacteria.
But antibiotics were prescribed for nearly 57 percent of doctors' visits for these infections, the study found.
"I thought it was really a clever study, actually, to get a sense of the burden of bacterial disease and what the antibiotic usage is," said Dr. Jason Newland, medical director of patient safety and system reliability, and associate professor of pediatrics at University of Missouri-Kansas City School of Medicine.
Newland, former director of the Antimicrobial Stewardship Program at Children's Mercy Hospital and Clinics in Kansas City, cited the 2013 "threat report" by the U.S. Centers for Disease Control and Prevention that indicated 23,000 Americans die each year due to antibiotic-resistant infections.
"We all know when we use antibiotics that we increase the chance of resistance because bacteria evolve," he said. "We need to use them well and not in such excess doses. We have to do way better."
A rapid strep test is currently available to distinguish between bacterial or viral throat infections. But other than that test, physicians have no other clinical tools to tell the cause of most upper respiratory infections, according to background information in the study. Kronman said he hopes the new research will not only help encourage the development of more such tools, but also spur clinicians to think more critically about prescribing antibiotics unless clearly needed.
Kronman added that prior research indicates that parents -- who often pressure pediatricians into prescribing antibiotics -- respond to alternate suggestions to alleviate their children's upper respiratory symptoms, such as using acetaminophen and humidifiers, instead of doctors simply saying they won't prescribe antibiotics.
"We have to take this [problem] on as a society," Newland said. "The reality is that the excess, unnecessary use of antibiotics is really putting us at great risk of not having these antibiotics [work] in the future."
Modern Healthcare readers selected four nurses in leadership roles to be ranked on this year’s 100 Most Influential People in Healthcare list, based on their effect on the industry.
“It’s great for nursing, because we do this together,” said Marla J. Weston, PhD, RN, FAAN, chief executive officer of the American Nurses Association, who made the magazine’s annual list for the first time, ranking 45th.
“I’m honored to be recognized,” she continued, “but I realize this is not about me. It’s about the hundreds and thousands of nurses working together to make the American Nurses Association a powerful force, to make nursing a powerful force, and to help our colleagues in health care and the general public understand the impact of nursing practice. I am the lucky person to be in the CEO role, but there are a lot of people making this happen.”
Other nurses in leadership who made the list included Marilyn Tavenner, agency administrator with the Centers for Medicare & Medicaid Services (CMS), listed fifth; Sister Carol Keehan, DC, MS, RN, president and CEO of Catholic Health Association in Washington, D.C., 34th; and Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI) in Cambridge, Mass., 50th.
“The four nurses on Modern Healthcare’s 100 Most Influential People list this year are transformative and visionary leaders, and some of the brightest lights in the nursing world,” said Susan B. Hassmiller, PhD, RN, FAAN, the Robert Wood Johnson Foundation senior adviser for nursing. “They are role models.”
Weston was one of 19 new people to join the list, which is dominated by elected and appointed government officials, top executives of health care industry corporations and physicians. Anyone can nominate a candidate. The magazine received 15,000 submissions for 2014. The top 300 nominees, including 10 nurses, were presented to Modern Healthcare readers for voting. Half of the candidates are selected through the reader votes and the other half by the magazine’s editors.
While not a nurse, RoseAnn DeMoro, executive director of National Nurses United (NNU), with 185,000 members, made the list again, at 41st.
“With the disproportionate economic influence of the hospital and insurance giants in particular, it is especially gratifying to see the name of RoseAnn and NNU on this list,” said NNU Co-president Deborah Burger, RN.
With the relatively small showing for nursing on this year’s list, opportunity exists for more nurses to move up to positions of leadership and influence.
“Nurses spend the most direct time with patients and, therefore, offer a vitally important perspective,” Keehan said. “As a nurse myself who moved into leadership, I encourage nurses to lend their voice to management decisions and consider leadership roles in their units or hospitals. It may not feel natural for some nurses to assert themselves, but the future of health care requires that we listen to their ideas and concerns. I hope to see many more nurses bring their passion for patient care and support of staff to the work of making health care better for everyone.”
Weston pointed out that nurses practice throughout the health care system, not only in hospitals but in home health, public health, primary care and long-term care. They observe when the system works and when it doesn’t for patients.
“That gives nurses the capacity to help make the system work for patents and communities and to redesign the system to transform and improve care,” Weston said. “Nurses are stepping forward to be leaders, and people are understanding nurses are not just functional doers of things, but thoughtful strategists.”
Weston expects more nurses will make the list in the years ahead. She encourages nurses to talk more about the work they do and the effect it has on people.
“The more we highlight the impact we are making, the more people will understand the great strategists and decision makers that nurses are,” Weston said. “There are a lots of pockets of innovation being led by nurses that are improving the quality of care, reducing the cost of health care and improving the access. We need to support each other in taking those pockets of innovation and spreading them.”
Weston has forged partnerships with other disciplines when delivering clinical care and when transforming the health care system.
“Health care is a team sport,” Weston said. “The degree we can work together catalyzes the work getting done.”
Increasing the number of nurses in leadership positions is one of the key recommendations of the Institute of Medicine’s groundbreaking Future of Nursing report and a central goal of the Campaign for Action.
“As the largest group of health professionals, and as those who spend the most time with patients, nurses have unique insight into health care,” Hassmiller said. “We need that insight at the highest levels of our health care system--on the boards of health care systems and hospitals; leading federal, state and local agencies; and more.”
Two members of the Campaign for Action’s strategic advisory committee made the 2014 Most Influential People in Healthcare list: Leah Binder, president and CEO of The Leapfrog Group, and Alan Morgan, CEO of the National Rural Health Association. Additionally, several members of organizations on the Champion Nursing Council and Champion Nursing Coalition were recognized.
“Health care transformation is underway in our country,” Hassmiller concluded. “Nurses possess the skills to ensure that the perspectives of people, families and communities remain front and center in any health decisions that get made.”
Meet the ‘Most Influential’ Nurses¹
5. Marilyn Tavenner, agency administrator with the Centers for Medicare and Medicaid Services, began her career as a nurse at Johnson-Willis Hospital in Richmond, Va., and spent 25 years working in various positions for HCA Inc., culminating as group president for outpatient services. Tavenner was one of several people in government to make Modern Healthcare’s annual list of the 100 Most Influential People in Healthcare.
34. Sister Carol Keehan, DC, MS, RN, president and CEO of Catholic Health Association, started out as a nurse and served in the 1980s as Providence Hospital's vice president for nursing, ambulatory care, and education and training. She joined the Catholic Health Association in 2005. She told NurseZone that she hopes many more nurses will bring their passion for patient care to make health care better for everyone.
45. Marla J. Weston, PhD, RN, FAAN, chief executive officer of the American Nurses Association, has held a variety of nursing roles, including direct patient care in intensive care and medical-surgical units, nurse educator, clinical nurse specialist, director of patient care support and nurse executive. She has served as executive director of the Arizona Nurses Association and deputy chief officer of the Veteran’s Affairs Workforce Management Office. Weston reported that she has had great role models and mentors in her nursing career.
50. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement, began as a staff nurse in 1973 at Quincy City Hospital, moved up and became chief operating officer in 1986, before joining IHI. Bisognano is one of many quality improvement leaders on this year’s Most Influential list.
A study in the current issue of Policy, Politics & Nursing Practice estimates 17.5% of newly licensed RNs leave their first nursing job within the first year and 33.5% leave within two years, according to a news release. The researchers found that turnover for this group is lower at hospitals than at other healthcare settings.
The study, which synthesized existing turnover data and reported turnover data from a nationally representative sample of RNs, was conducted by the RN Work Project, funded by the Robert Wood Johnson Foundation. The RN Work Project is a 10-year study of newly-licensed RNs that began in 2006. The study draws on data from nurses in 34 states, covering 51 metropolitan areas and nine rural areas. The RN Work Project is directed by Christine T. Kovner, PhD, RN, FAAN, professor at the College of Nursing, New York University, and Carol Brewer, PhD, RN, FAAN, professor at the School of Nursing, University at Buffalo.
“One of the biggest problems we face in trying to assess the impact of nurse turnover on our healthcare system as a whole is that there’s not a single, agreed-upon definition of turnover,” Kovner said. “In order to make comparisons across organizations and geographical areas, researchers, policy makers and others need valid and reliable data based on consistent definitions of turnover. It makes sense to look at RNs across multiple organizations, as we did, rather than in a single organization or type of organization to get an accurate picture of RN turnover.”
According to the release, the research team noted that, in some cases, RN turnover can be helpful — as in the case of functional turnover, when a poorly functioning employee leaves, as opposed to dysfunctional turnover, when well-performing employees leave. The team recommends organizations pay attention to the kind of turnover occurring and point out their data indicate that when most RNs leave their jobs, they go to another healthcare job.
“Developing a standard definition of turnover would go a long way in helping identify the reasons for RN turnover and whether managers should be concerned about their institutions’ turnover rates,” Brewer said in the release. “A high rate of turnover at a hospital, if it’s voluntary, could be problematic, but if it’s involuntary or if nurses are moving within the hospital to another unit or position, that tells a very different story.”
The RN Work Project’s data include all organizational turnover (voluntary and involuntary), but do not include position turnover if the RN stayed at the same healthcare organization, according to the release.
McBaine, a bouncy black and white springer spaniel, perks up and begins his hunt at the Penn Vet Working Dog Center. His nose skims 12 tiny arms that protrude from the edges of a table-size wheel, each holding samples of blood plasma, only one of which is spiked with a drop of cancerous tissue.
The dog makes one focused revolution around the wheel before halting, steely-eyed and confident, in front of sample No. 11. A trainer tosses him his reward, a tennis ball, which he giddily chases around the room, sliding across the floor and bumping into walls like a clumsy puppy.
McBaine is one of four highly trained cancer detection dogs at the center, which trains purebreds to put their superior sense of smell to work in search of the early signs of ovarian cancer. Now, Penn Vet, part of the University of Pennsylvania’s School of Veterinary Medicine, is teaming with chemists and physicists to isolate cancer chemicals that only dogs can smell. They hope this will lead to the manufacture of nanotechnology sensors that are capable of detecting bits of cancerous tissue 1/100,000th the thickness of a sheet of paper.
“We don’t ever anticipate our dogs walking through a clinic,” said the veterinarian Dr. Cindy Otto, the founder and executive director of the Working Dog Center. “But we do hope that they will help refine chemical and nanosensing techniques for cancer detection.”
Since 2004, research has begun to accumulate suggesting that dogs may be able to smell the subtle chemical differences between healthy and cancerous tissue, including bladder cancer, melanomaand cancers of the lung, breast and prostate. But scientists debate whether the research will result in useful medical applications.
Dogs have already been trained to respond to diabetic emergencies, or alert passers-by if an owner is about to have a seizure. And on the cancer front, nonprofit organizations like the In Situ Foundation, based in California, and the Medical Detection Dogs charity in Britain are among a growing number of independent groups sponsoring research into the area.
A study presented at the American Urological Association’s annual meeting in May reported that two German shepherds trained at the Italian Ministry of Defense’s Military Veterinary Center in Grosseto were able to detect prostate cancer in urine with about 98 percent accuracy, far better than the prostate-specific antigen (PSA) test. But in another recent study of prostate-cancer-sniffing dogs, British researchers reported that promising initial results did not hold up in rigorous double-blind follow-up trials.
Dr. Otto first conceived of a center to train and study working dogs when, as a member of the Federal Emergency Management Agency’s Urban Search and Rescue Team, she was deployed to ground zero in the hours after the Sept. 11 attacks.
“I remember walking past three firemen sitting on an I-beam, stone-faced, dejected,” she says. “But when a handler walked by with one of the rescue dogs, they lit up. There was hope.”
Today, the Working Dog Center trains dogs for police work, search and rescue and bomb detection. Their newest canine curriculum, started last summer after the center received a grant from the Kaleidoscope of Hope Foundation, focuses on sniffing out a different kind of threat: ovarian cancer.
“Ovarian cancer is a silent killer,” Dr. Otto said. “But if we can help detect it early, that would save lives like nothing else.”
Dr. Otto’s dogs are descended from illustrious lines of hunting hounds and police dogs, with noses and instincts that have been refined by generations of selective breeding. Labradors and German shepherds dominate the center, but the occasional golden retriever or springer spaniel — like McBaine — manages to make the cut.
The dogs, raised in the homes of volunteer foster families, start with basic obedience classes when they are eight weeks old. They then begin their training in earnest, with the goal of teaching them that sniffing everything — from ticking bombs to malignant tumors — is rewarding.
“Everything we do is about positive reinforcement,” Dr. Otto said. “Sniff the right odor, earn a toy or treat. It’s all one big game.”
Trainers from the center typically notice early on that certain dogs have natural talents that make them better suited for specific kinds of work. Search and rescue dogs must be tireless hunters, unperturbed by distracting environments and unwilling to give up on a scent – the equivalent of high-energy athletes. The best cancer-detection dogs, on the other hand, tend to be precise, methodical, quiet and even a bit aloof — more the introverted scientists.
“Some dogs declare early, but our late bloomers frequently switch majors,” Dr. Otto said.
Handlers begin training dogs selected for cancer detection by holding two vials of fluid in front of each dog, one cancerous and one benign. The dogs initially sniff both but are rewarded only when they sniff the one containing cancer tissue. In time, the dogs learn to recognize a unique “cancer smell” before moving on to more complex tests.
What exactly are the dogs sensing? George Preti, a chemist at the Monell Chemical Senses Center in Philadelphia, has spent much of his career trying to isolate the volatile chemicals behind cancer’s unique odor. “We have known for a long time that dogs are very sensitive detectors,” Dr. Preti says. “When the opportunity arose to collaborate with Dr. Otto at the Working Dog Center, I jumped on it.”
Dr. Preti is working to isolate unique chemical biomarkers responsible for ovarian cancer’s subtle smell using high-tech spectrometers and chromatographs. Once he identifies a promising compound, he tests whether the dogs respond to that chemical in the same way that they respond to actual ovarian cancer tissue.
“I’m not embarrassed to say that a dog is better than my instruments,” Dr. Preti says.
The next step will be to build a mechanical, hand-held sensor that can detect that cancer chemical in the clinic. That’s where Charlie Johnson a professor at Penn who specializes in experimental nanophysics, the study of molecular interactions between microscopic materials, comes in.
He is developing what he calls Cyborg sensors, which include biological and mechanical components – a combination of carbon nanotubes and single-stranded DNA that preferentially bond with one specific chemical compound. These precise sensors, in theory, could be programmed to bind to, and detect, the isolated compounds that Dr. Otto’s dogs are singling out.
“We are effectively building an electronic nose,” said Dr. Johnson, who added that a prototype for his ovarian cancer sensor will probably be ready in the next five years.
Some experts remain skeptical.
“While I applaud any effort to detect ovarian cancer, I’m uncertain that this research will have any value,” said Dr. David Fishman, a gynecologic oncologist at Mount Sinai Hospital in New York City. One challenge, he notes, is that any cancer sensor would need to be able to detect volatile chemicals that are specific to one particular type of cancer.
“Nonspecificity is where a lot of these sort of tests fail,” Dr. Fishman said. “If there is an overlap in volatile chemicals — between colon, breast, pancreatic, ovarian cancer — we’ll have to ask, ‘What does this mean?’ ”
And even if sensors could be developed that detect ovarian cancer in the clinic, Dr. Fishman says, he doubts that they would be able to catch ovarian cancer in its earliest, potentially more treatable, stages.
“The lesions that we are discussing are only millimeters in size, and almost imperceptible on imaging studies,” Dr. Fishman says. “I don’t believe that the resolution of the canine ability will translate into value for these lesions.”
McBaine remains unaware of the debate. After correctly identifying yet another cancerous plasma sample, he pranced around the Working Dog Center with regal flair, showing off his tennis ball to anyone who would pay attention. In an industry saturated with hundreds of corporations and thousands of scientists all hunting for the earliest clues to cancer, working dogs are just another set of (slightly furrier) researchers.
Imagine a time when a device alerts you to the onset of a disease in your body long before it’s a problem. Or when your disease is diagnosed in Shanghai, based on the medical scan you did in Kenya. This future is far closer that you might think due to rapid advances in connected devices and sensors, big data and the integration of health services. Combined, these innovations are introducing a new era in healthcare and personal well-being.
In only a few years, mobile technologies have spawned tremendous innovation of consumer-level health tools. The emerging solutions are focusing on health conditions over a person’s lifetime and on holistic care. They generate constant insights through analytics and algorithms that identify patterns and behaviours. Social technologies enable better collaboration and interconnected digital propositions that reach out to communities of people with similar conditions, engaging them in ways which were never before possible.
We are starting to get a taste of what the consumerization of healthcare will mean in the future. In two to three years, analysing your personal health data will become commonplace for large parts of the population in many countries. Also, it is very likely that for the first time it will not be the chronically ill but the healthy people who will invest the most in managing their health.
Digitization and consumerization will rattle the healthcare industry. It is already tearing at the very fabric of the traditional healthcare companies and providers. Innovation is not only about just adding a new channel or connecting a product. It is also a complete redesign of business models, adjustment of systems and processes and, most importantly, it calls for changing the culture in companies to reflect the new opportunities – and challenges – presented by the digital world.
To drive true industry transformation, companies need to collaborate and continue to learn from each other. Great strides will be made in alliances, which, for example, will deliver open, cloud-based healthcare platforms that combine customer engagement with leading medical technology, and clinical applications and informatics.
The game will not only be played by the traditional healthcare providers. With consumerization, even companies without healthcare expertise, but with strong consumer engagement and trust, could potentially become healthcare companies. Big multinationals invest incremental budgets in developing new propositions and count on their global user bases or professional networks to gain a foothold in the market.
And in parallel, a raft of start-ups are attempting to transform the worlds of preventive or curative healthcare – in many cases, limited only by their imaginations. For example, we may see virtual reality technology moving from gaming industry to healthcare for improving patients’ rehabilitation after a stroke. Or we may see facial recognition software become common in monitoring and guiding patients’ daily medical routines.
While these new propositions tackle a number of healthcare industry’s core concerns and provide solutions to completely new areas, these propositions still need to mature. They need to become scalable, reliable, open, and the user experience needs to be harmonized.
But perhaps one of the most important challenges is related to people’s behaviour and preferences. Regardless of whether these new and existing companies are analysing health data, using virtual reality or reading people’s vital signs, they all need ample time to become trusted and accepted in the emerging digital health care space. Especially for the new entrants, obtaining the right level of credibility will be one of the key success factors.
Consumers, patients and professionals alike, will need the right motivation, reassurance and mindsets to adopt these new solutions. The companies that know how to offer us tailored, cutting-edge solutions, combined with meaningful advice and trustworthiness, will be the winners and become our trusted advisers in health.
Making the transition to working nights may feel a bit intimidating, but many night nurses, myself included, have grown to love the position! It tends to be quieter and less chaotic because the patients are generally asleep, and there's a special camaraderie that develops between a team of night nurses. Put these tips into practice to survive, and even thrive, in your night shifts.
Stack several night shifts in a row: Rather than spacing out your night shifts during the week and having to switch between being up during the day and up during the night, try to put all your night shifts for the week in a row. That way, you can really get yourself onto a schedule of being awake during the nights you work and sleeping during the days in between.
Nap before work: As you transition from being awake during the day to being awake as you work at night, take a nap in the afternoon to help you go into your first night shift as rested as possible. Alternately, if your schedule allows, stay up later than usual the night before your first night shift and sleep in as late as you can the next morning.
Fuel up with healthy foods: While sugars may seem like they provide energy, they also come with a crash. Before heading into work, eat a filling meal with a healthy balance of carbohydrates, protein, and fiber. Then bring healthy snacks for the night that include protein and fiber to keep you going strong. Some options include yogurt, mixed nuts, hard boiled eggs, cheese cubes, or carrots with hummus dip
Plan caffeine carefully: It can be tempting to drink a cup of coffee anytime you feel sleepy, but you may develop an unhealthy dependence or be unable to fall asleep when you get home after your shift. Therefore, try to limit yourself to just one or two cups of coffee per shift, and drink your last one at least six hours before you plan to go to sleep.
Create a restful sleeping environment at home: The key to surviving night shifts in the long term is getting lots of restful sleep after each shift. Set up room darkening curtains and a white noise machine to help you block out signs of the day. When you get home, don't force yourself to go to bed right away. Instead, develop a routine that includes some time to bathe, read, and relax as your body winds down after work. Try to avoid bright screens, which block your body from releasing melatonin, the hormone that makes you feel sleepy.
With some attention to detail, you will probably find yourself really enjoying working at night. Many of the night nurses I know started out stuck on the shifts, but grew to prefer them. Plus, the pay differential doesn't hurt at all!
One California teacher is happy to simply be back in the classroom as the new school year kicks off.
After being diagnosed with breast cancer last year, Carol Clark was forced to stay out of the classroom for nearly the entire year due to treatments and complications.
Eventually she was gone for so long, her health insurance and salary were threatened. But Clark's benefits were saved after multiple colleagues donated their sick days to the 6th grade teacher.
Clark, 56, a teacher at Jaime Escalante Elementary School in Cudahy, California, ended up receiving an additional 154 sick days from co-workers or other teachers as part of a program run by the Los Angeles Unified School District to help teachers in Clark’s situation, according to ABC News station KABC-TV in Los Angeles.
Before the donation Clark had been struggling to keep her salary and benefits. For many teachers in the Los Angeles area, once they use up their sick days and their vacation days they can start losing both their salary and health benefits.
Last year Clark missed nearly all of the school year except for just two months. Clark originally thought she would be able to come back for the spring semester, but she ended up needing major surgery after complications arose.
“I finished chemotherapy. Within a week I developed complications,” said Clark. “I couldn’t come back to school at all.”
To cover her time off, Clark used her vacation days and another 120 sick days that she had accrued over 16 years of teaching. But it wasn’t enough.
At the end of last year, she had no more sick days and was still too sick to teach. Clark had one other option. Her husband, also a teacher at Jaime Escalante Elementary School, was able to rally co-workers and other teachers to donate their sick days as part of the “Catastrophic Illness Donation Program.”
"We get paid for 180 days in the school year. So she got 154, so almost a whole year," Dave Clark told KABC-TV.
Gayle Pollard-Terry, deputy director of communications for the Los Angeles Unified School District, told ABC News that the program helps around 20 to 25 teachers every year.
“When you run out of all of your sick paid leave…if you run out, you [can] lose your health benefits and your income,” she said.
Pollard-Terry said the program can help fill the gap for sick teachers or school district employees.
She said although most donations are not as extreme as Clark’s tally, there have been at least two other donation drives where more than 150 days were raised for a teacher.
For Carol Clark the outpouring of donations from co-workers both past and present was surprising and emotional. She now has extra days to help her through new surgeries scheduled for this year.
“Other people ask me ‘What do you say to people who donate?’” said Clark. “I don’t know what to say to them. I say thank you. But that doesn’t’ seem like enough. It was really a tremendous thing that they did.”
Clark said she tried to thank her co-workers in a staff meeting but was too “chocked up” to speak. Instead she ended up writing them an email to thank them.
When a fire department gets a call for medical help, most of them scramble both an ambulance and a fully staffed fire truck. But that's way more than most people need, according to Rick Lewis, chief of emergency medical services at South Metro Fire Rescue Authority in the Denver suburbs.
"It's not the prairie and the Old West anymore, where you have to be missing a limb to go to the hospital," Lewis says, "Now it's a sore throat or one day of cold or flu season sometimes, and that can be frustrating for people, I know it is."
South Metro receives more than 12,000 emergency medical calls a year, and takes about 7,000 patients to area hospitals. Somebody who's been running a fever for a couple of days may need help — just not necessarily a ride to the ER. That disconnect can be frustrating for both ambulance crews and patients.
Crews aren't required to transport everyone who calls, but Lewis says they fear lawsuits if they were to leave and a patient got worse. Also, ambulance companies typically don't get paid unless they take somebody to the hospital. So Lewis teamed up with Mark Prather, an emergency room doctor, to try and come up with a better way.
"We created a mobile care unit that can go to a given patient, if we think they're safe to treat on scene, and provide definitive on-scene treatment," says Prather.
The mobile care unit is, basically, a station wagon. Advance practice paramedic Eric Bleeker shows off some of the gear. "This one is a suture set, so it has everything for wound closure, from staples to regular sutures," he says.
Ambulances don't have that kind of equipment, so even someone who just needs a few stitches gets a ride to the emergency department.
Several cities across the country are using paramedics as physician extenders, sending ambulance crews to do routine things like hospital follow-up visits in places where basic health care is hard to get. South Metro's model focuses on responding to calls. The team always includes at least one nurse practitioner, who can prescribe basic medicines that they stock in the mobile unit.
"A lot of what we do is sort of that mid-level between the acute care you receive in an emergency department and what the paramedics can currently do," says Bleeker.
It's kind of like an urgent care clinic on wheels.
There's also a miniature medical lab. "We can run full blood chemistry, we can do complete blood counts, we can check for strep throat, we can check for influenza," he says. Those are capabilities that even many doctors' offices don't have on site.
South Metro Fire also relies heavily on Colorado's new electronic medical records network. The nurse or EMT can call up patient records on the scene to provide care that's more like an office visit, and dispatchers can check recent medical histories to make sure they send ambulances to people who might really need one.
That person who called 911 because they were running a fever could end up being diagnosed and treated in their living room by South Metro's station wagon for about $500, instead of spending a lot more for similar care at an emergency room.
Insurance companies don't yet pay for this, though, says Prather.
"That's maybe why nobody has done it yet," he says, laughing.
For the last nine months South Metro has been running the service basically for free, to prove that it saves money. But Prather thinks that's about to change because of Obamacare. The law aims to get insurance companies, Medicare and Medicaid to stop paying for too much medical care. And it can penalize health care providers who contribute to overuse of emergency rooms.
"It allowed us to think about payment differently, and basically switch from a volume situation to a quality situation," he says.
But it's not like the law just flips a switch and starts paying for appropriate care instead of rewarding providers who see a high number of patients and do lots of procedures. The change to reward efficient, appropriate health care is just starting to happen. Slowly. But Prather is now in talks with insurers and hopes to be getting paid soon.
Raymond and Mazie Huggins, a devoted West Virginia couple with the same failing heart condition, didn’t think they would make it to their upcoming 74th wedding anniversary on Oct. 10.
But in August, Raymond or “Huggie Bear,” 96, and Mazie Leota, 93, received newly FDA-approved heart valves in a life-saving procedure on the same day.
“We went to the supper table one night and Raymond said, ‘If you have it done, then I will have it done and that’s how we will do it — together,'” Mazie said. “We went in together, had it done together and came home together.”
The couple went to the Cleveland Clinic for transcatheter aortic valve replacement or TAVR, a procedure designed for those who typically can’t withstand the risk of open-heart surgery. A catheter is wound through an artery in the groin and into the heart muscle.
This non-invasive surgery has been used on patients for some time, but the smaller valve required for the Huggins’ surgery was just approved in June after successful clinical trials.
“I’m very glad we had it and I am feeling fine,” said Mazie, a great-grandmother and former dental secretary. “I can’t get over there not being any pain afterwards.”
Now, the couple, both “with it” intellectually and otherwise healthy, can celebrate their long marriage at home in Moundsville, where they continue to live independently. They have every reason to expect to live an even longer life: Mazie’s maternal grandmother lived to be 108.
“My father’s goal was to live long enough to get on the Smuckers jar,” said their son, Roger Huggins, 67. “Last year, even with his heart problems, he made apple butter and applesauce out of the tree in the backyard.”
Roger said his father, a former glass factory shipper and retired prison guard, is “very strong and a tremendously hard worker.” He calls his mother an “angelic” woman who worries about others and is beloved by all who know her.
“My mother protects my father to the fullest,” said Roger. “He might make her madder than the dickens, but she protects him to the fullest.”
Two years ago, his parents had stents put in their hearts on the same day.
“I was in pre-op with them,” said Roger, a retired food company sales rep. “Their tables passed in the hallways and they were awake enough to make [the medical staff] stop their beds. They held hands and kissed each other and had the whole hospital crying.”
Roger, who drives three hours each way from his home in Erie, Pennsylvania, to check in on his parents and organize their medications, persuaded them to have the TAVR procedure after doing his own research.
Raymond insisted his wife go first, then his surgery followed.
“They both were prepared to pass away on the table,” said their son. “But it very well could have been much worse if my mother had woken up and my dad had died beside her. Or harder if my father had woken up.”
“The first thing my father said when he came out of the anesthesia was, ‘Am I alive?’” said Roger. “The second thing he said was, ‘Is my wife alive?’ The third thing he said is, ‘I’ve got to go out and fix the yard.’ He’s a workaholic.”
The Hugginses may not be the oldest patients ever to undergo TAVR surgery (some patients have been 98 and 100), but they were the first couple, according to their surgeon, interventional cardiologist Dr. Samir Kapadia.
“The data suggest that 50 to 60 percent would not make it until the end of the year with their condition,” he said. “They were declining fairly fast. … When they came to us they were very short of breath and had medical problems that were unbelievably complex.”
The aortic valve is the “door” to the heart, according to Kapadia. A normal opening is about 2.5 cm. But theirs were closed down to .3 and .4 — “about 10 times less.”
“Five or 10 years ago, nothing could have been done for them,” he said. “We would have had to stop the heart and open up the chest, and at that age the recovery would be up to two months, with significant risk,” he said.
Mazie was prepped for surgery first at 5:30 a.m. and Raymond followed at 9:30 a.m.
“The kissed each other and were in recovery opposite each other and wanted to be together holding hands in the same room,” said Kapadia.
By the evening after surgery, they were out of bed, and the next day, they were walking. Mazie’s release was delayed because of fluid in her lungs, so Raymond insisted on staying at the hospital with her for several more days.
The couple is now back at home with a part-time caregiver, looking forward to their anniversary next month.
Mazie attributes their 74-year happy marriage to good communication.
“There have been a few ups and downs,” she said. “If you don’t agree, get it out and say it and get it over with.”
Kapadia said the family’s closeness was an important factor in the surgery’s success.
“They are wonderful people,” he said. “Their son fought for them to be treated together as the only best option. Who would take care of the other one? It would have been a disaster for their family life.”
“But more than anything else, they wanted to live and celebrate and enjoy the last part of their life together.”
A respiratory virus is sending hundreds of children to hospitals in Missouri and possibly throughout the Midwest and beyond, officials say.
The unusually high number of hospitalizations reported now could be "just the tip of the iceberg in terms of severe cases," said Mark Pallansch, a virologist and director of the Centers for Disease Control and Prevention's Division of Viral Diseases.
"We're in the middle of looking into this," he told CNN on Sunday. "We don't have all the answers yet."
Ten states have contacted the CDC for assistance in investigating clusters of enterovirus: Colorado, North Carolina, Georgia, Ohio, Iowa, Illinois, Missouri, Kansas, Oklahoma and Kentucky.
What is Enterovirus EV-D68?
Enteroviruses, which bring on symptoms like a very intense cold, aren't unusual. They're actually common. When you have a bad summer cold, often what you have is an enterovirus, he said. The season often hits its peak in September.
The unusual situation now is that there have been so many hospitalizations.
The virus has sent more than 30 children a day to a Kansas City, Missouri, hospital, where about 15% of the youngsters were placed in intensive care, officials said.
In a sign of a possible regional outbreak, Colorado, Illinois and Ohio are reporting cases with similar symptoms and are awaiting testing results, according to officials and CNN affiliates in those states.
In Kansas City, about 475 children were recently treated at Children's Mercy Hospital, and at least 60 of them received intensive hospitalization, spokesman Jake Jacobson said.
"It's worse in terms of scope of critically ill children who require intensive care. I would call it unprecedented. I've practiced for 30 years in pediatrics, and I've never seen anything quite like this," said Dr. Mary Anne Jackson, the hospital's division director for infectious diseases.
"We've had to mobilize other providers, doctors, nurses. It's big," she said.
The Kansas City hospital treats 90% of that area's ill children. Staff members noticed an initial spike on August 15, Jackson said.
"It could have taken off right after school started. Our students start back around August 17, and I think it blew up at that point," Jackson said. "Our peak appears to be between the 21st and the 30th of August. We've seen some leveling of cases at this point."
What parents should know about EV-D68
No vaccine for virus
This particular type of enterovirus -- EV-D68 -- is uncommon but not new. It was identified in the 1960s, and there have been fewer than 100 reported cases since that time. But it's possible, Pallansch said, that the relatively low number of reports might be because EV-D68 is hard to identify.
EV-D68 was seen last year in the United States and this year in various parts of the world. Over the years, clusters have been reported in Georgia, Pennsylvania, Arizona and various countries including the Philippines, Japan and the Netherlands.
An analysis by the CDC showed at least 30 of the Kansas City children tested positive for EV-D68, according to the Missouri Department of Health and Senior Services.
Vaccines for EV-D68 aren't currently available, and there is no specific treatment for infections, the Missouri agency said.
"Many infections will be mild and self-limited, requiring only symptomatic treatment," it said. "Some people with several respiratory illness caused by EV-D68 may need to be hospitalized and receive intensive supportive therapy."
Some cases of the virus might contribute to death, but none of the Missouri cases resulted in death, and no data are available for overall morbidity and mortality from the virus in the United States, the agency said.
Symptoms include coughing, difficulty breathing and rash. Sometimes they can be accompanied by fever or wheezing.
Jackson said physicians in other Midwest states reported cases with similar symptoms.
"The full scope is yet to be known, but it would appear it's in the Midwest. In our community, meticulous hand-washing is not happening. It's just the nature of kids," Jackson said.
'Worst I've seen'
Denver also is seeing a spike in respiratory illnesses resembling the virus, and hospitals have sent specimens for testing to confirm whether it's the same virus, CNN affiliate KUSA said.
More than 900 children have gone to Children's Hospital Colorado emergency and urgent care locations since August 18 for treatment of severe respiratory illnesses, including enterovirus and viral infections, hospital spokeswoman Melissa Vizcarra said. Of those, 86 have been sick enough to be admitted to the Aurora facility.
And Rocky Mountain Hospital for Children had five children in intensive care and 20 more in the pediatric unit, KUSA said last week.
"This is the worst I've seen in my time here at Rocky Mountain Hospital for Children," Dr. Raju Meyeppan told the outlet. "We're going to have a pretty busy winter at this institution and throughout the hospitals of Denver."
Will Cornejo, 13, was among the children in intensive care at Rocky Mountain Hospital for Children after he came down with a cold last weekend and then woke up Tuesday night with an asthma attack that couldn't be controlled with his medicine albuterol. His mother, Jennifer, called 911 when her son's breathing became shallow, and her son was airlifted to the Denver hospital, she told KUSA.
Her son was put on a breathing tube for 24 hours.
"It was like nothing we've ever seen," Jennifer Cornejo told KUSA. "He was unresponsive. He was laying on the couch. He couldn't speak to me. He was turning white, and his lips turned blue.
"We're having a hard time believing that it really happened," she added. "We're much better now because he is breathing on his own. We're on the mend."
Restricting kids' visits with patients
In East Columbus, Ohio, Nationwide Children's Hospital saw a 20% increase in patients with respiratory illnesses last weekend, and Dr. Dennis Cunningham said patient samples are being tested to determine whether EV-D68 is behind the spike, CNN affiliate WTTE reported.
Elsewhere, Hannibal Regional Hospital in Hannibal, Missouri, reported "recent outbreaks of enterovirus infections in Missouri and Illinois," the facility said this week on its Facebook page.
Blessing Hospital in Quincy, Illinois, saw more than 70 children with respiratory issues last weekend, and seven of them were admitted, CNN affiliate WGEM reported. The hospital's Dr. Robert Merrick believes that the same virus that hit Kansas City is causing the rash of illnesses seen at the Quincy and Hannibal hospitals, which both imposed restrictions this week on children visiting patients, the affiliate said.
"Mostly we're concerned about them bringing it in to a vulnerable patient. We don't feel that the hospital is more dangerous to any other person at this time," Merrick told WGEM.
Blessing Hospital is working with Illinois health officials to identify the virus, the hospital said in a statement.
While there are more than 100 types of enteroviruses causing up to 15 million U.S. infections annually, EV-D68 infections occur less commonly, the Missouri health agency said. Like other enteroviruses, the respiratory illness appears to spread through close contact with infected people, the agency said.
"Unlike the majority of enteroviruses that cause a clinical disease manifesting as a mild upper respiratory illness, febrile rash illness, or neurologic illness (such as aseptic meningitis and encephalitis), EV-D68 has been associated almost exclusively with respiratory disease," the agency said.
Clusters of the virus have struck Asia, Europe and the United States from 2008 to 2010, and the infection caused relatively mild to severe illness, with some intensive care and mechanical ventilation, the health agency said.
To reduce the risk of infection, individuals should wash hands often with soap and water for 20 seconds, especially after changing diapers; avoid touching eyes, nose and mouth with unwashed hands; avoid kissing, hugging and sharing cups or eating utensils with people who are sick; disinfect frequently touched surfaces such as toys and doorknobs; and stay home when feeling sick, the Missouri agency said.
Higher education is a key requirement for nurses as the U.S. healthcare environment grows ever-more reliant on technology and specialized skills. There are three common academic pathways toward becoming a registered nurse (RN): the nursing diploma, associate degree (ADN) and bachelor’s degree (BSN).
Following completion of one of these programs, graduates must pass the National Council Licensure Examination for Registered Nurses (NCLEX-RN) and satisfy state licensing requirements to begin work as an RN. Bridge programs, such as LPN-to-RN and ADN-to-BSN, allow nurses to move ahead in their nursing careers.
Each choice of training program is distinct and offers levels of education to qualify graduates for increasingly responsible roles in nursing practice. This guide is designed to break down the step-by-step process for becoming an RN, including the various routes possible on this career roadmap. Included is an overview of potential specializations and certifications for those interested in moving beyond basic nursing duties. Below are estimates for RN salaries and job growth as well as tools to help prospective nurses search for online and traditional educational programs.
WHAT DOES A REGISTERED NURSE DO?
More than 2.7 million registered nurses are employed in the United States, and nearly 30 percent work in hospitals, according to the Bureau of Labor Statistics (BLS). Other RNs work in clinics, physicians’ offices, home health care settings, critical and long-term care facilities, governmental organizations, the military, schools and rehabilitation agencies.
Duties include administering direct care to patients, assisting physicians in medical procedures, providing guidance to family members and leading public health educational efforts. Depending on assignment and education, an RN may also operate medical monitoring or treatment equipment and administer medications. With specialized training or certifications, RNs may focus on a medical specialty, such as geriatric, pediatric, neonatal, surgical or emergency care. Registered nurses work in shifts that run around the clock, on rotating or permanent schedules, and overtime and emergency hours can be unpredictable. Registered nurses are required to complete ongoing education to maintain licensing, and they may choose to return to college to complete a bachelor’s degree or master’s degree with the goal of moving into advanced nursing practice roles or health care administration.
THE STEPS: BECOMING A REGISTERED NURSE
Step 1: COMPLETE AN APPROVED NURSING PROGRAM
Anyone who wants to be an RN must finish a nurse training program. Options include programs that award nursing diplomas, associate and bachelor’s degrees. An associate degree in nursing (ADN) typically takes from two to three years to complete. Accelerated nursing degree programs could potentially shorten the time required. A bachelor’s degree in nursing (BSN) takes about four years of full-time study to complete, or two years for those in an ADN-to-BSN program. While the structure and content of these training programs differs, they should feature the opportunity to gain supervised clinical experience.
Students may initially only have the time and money to complete a two-year program, but they might later decide to convert their ADN to a BSN degree. Or, students may leap directly into a four-year BSN program if they plan on moving into roles in administration, advanced nursing, nursing consulting, teaching or research. Nursing students complete courses such as the following:
Anatomy
Biochemistry
Biology
Chemistry
Computer literacy
Health care law and ethics
Mathematics
Microbiology
Nutrition
Patient care
Psychology
A bachelor’s degree program may also include courses on specific health populations, leadership, health education and an overview of potential specializations. A four-year bachelor’s degree program could require liberal arts courses and training in critical thinking and communication to complete the curriculum. Bachelor’s programs can broaden nursing experience beyond the hospital setting. According to the BLS, some employers require newly appointed RNs to hold a bachelor’s degree.
Step 2: PASS THE NCLEX-RN
Accredited undergraduate nursing degree or diploma programs alike are designed to prepare students to sit for the NCLEX examination. Upon graduation, aspiring RNs should register with the National Council of State Boards of Nursing to sign up for the National Council Licensure Examination for Registered Nurses. Candidates receive an Authorization to Test notification before the exam. At the exam, rigorous verification of candidates' identity may include biometric scanning.
This computerized exam has an average of 119 test items to be completed within a six-hour time limit. Examinees who do not pass must wait from 45 days to three months to re-take the exam. According to the California Board of Registered Nursing, students who take the exam right after graduation have a higher chance of passing.
Step 3: OBTAIN A STATE LICENSE
Every state and the District of Columbia require that employed registered nurses hold current licenses. However, requirements vary by state, so students should contact their state board of nursing or nurse licensing to determine exact procedures. In some states, RNs need to complete the NCLEX-RN, meet state educational requirements and pass a criminal background check. The National Council of State Boards of Nursing maintains a listing of licensing requirements on its website.
Step 4: PURSUE ADDITIONAL TRAINING AND CERTIFICATION (OPTIONAL)
For professionals who decide to become advanced practice registered nurses (APRNs), a BSN degree provides an academic stepping-stone to master’s degree programs. There are also bridge programs for students who only hold a two-year nursing degree and RN licensure but wish to enroll in graduate programs.
Those with master's degrees may qualify for positions such as certified nurse specialists, nurse anesthetists, nurse practitioners (NPs) and nurse midwives. It's important to research evolving professional requirements. For example, the American Association of Colleges of Nursing proposes that NPs should earn a Doctor of Nursing Practice (DNP) degree. A DNP or a PhD degree may appeal to nursing professionals who seek positions as scientific researchers or university professors in the nursing sciences. RNs may also seek certifications in a medical specialty such as oncology. Certifications are offered by non-governmental organizations attesting to nurses' qualifications in fields such as critical care, acute care, nursing management or other advanced areas.
To learn more about RN statistics, jobs, salary and other information CLICK HERE.
The path to becoming a nurse depends on which type of nursing career you’d like to pursue. You could choose to be a licensed practical nurse (LPN) or a registered nurse (RN).
An LPN program is typically one year long. Programs to become an RN are either three-year hospital-based nursing school programs (diploma), or two- or four-year college programs. Graduates from two-year programs earn an associate degree in nursing (ADN), while those who attended four-year college programs graduate with a bachelor’s of science in nursing (BSN). Successful completion of such a program allows you to write the licensing exam, called the NCLEX. Once you have passed the NCLEX, you can apply for a license to practice as a nurse in your state.
LPNs who want to become RNs may be able to follow an LPN-to-RN bridge program. This type of program is adapted for students who already have a nursing background. Registered nurses with the ADN who want to get their BSN may be interested in following an ADN-to-BSN bridge program.
Furthering your nursing education means acquiring more advanced skills and performing more critical tasks. For example, you must be a registered nurse and have at least a master’s in nursing to enter more advanced careers in the field, including nurse practitioner, nurse midwife or nurse anesthetist.
Before applying to colleges or signing up for classes, ask yourself a handful of critical questions: Do I need a bachelor’s degree to work as a nurse? What happens if I fail the NCLEX? Where will I feel comfortable starting as a nurse? Do I want to work myself up to a higher level of nursing gradually or do I want to go straight there?
The following guide helps answer these questions and illustrates the various pathways that aspiring nurses may take to pursue the career they truly want.
WHAT DOES A NURSE DO?
Although nursing responsibilities vary by specialization or unit, nurses have more in common than they have differences. Nurses provide, coordinate and monitor patient care, educate patients and family members about health conditions, provide medications and treatments, give emotional support and advice to patients and their family members, provide care and support to dying patients and their families, and more. They also work with healthy people by providing preventative health care and wellness information.
Although nurses work mostly in hospitals, they can also work in or for schools, private clinics, nursing homes, placement agencies, businesses, prisons, military bases and many other places. Nurses can provide hands-on care, supervise other nurses, teach nursing, work in administration or do research – the sky is the limit.
Work hours for nurses vary quite a bit. While some nurses do work regular shifts, others must work outside traditional work hours, including weekends and holidays. Some nurses work longer shifts, 10 to 12 hours per day, for example, but this allows them to work fewer days and have more days off.
COMMON SKILLS FOR NURSES
Good nurses are compassionate, patient, organized, detail oriented and have good critical thinking skills. An interest in science and math is important due to the content of nursing programs and the technology involved. Nurses must be able to function in high stress situations and be willing to constantly learn as the profession continues to grow and develop.
TYPES OF NURSING CAREERS
If you choose to become an LPN, you will likely provide direct patient care under the supervision of an RN or physician.
Registered nurses have more autonomy than LPNs, and the degree of care they provide depends on their level of education. An RN with an associate degree generally provides hands-on care directly to patients and can supervise LPNs. There may also be some administrative work. An RN with a BSN can take on more leadership roles and more advanced nursing care in specialized units, for example.
Nurses can continue to get a master’s degree in nursing (MSN) and become nurse practitioners, nurse midwives or nurse anesthetists. These are called advanced practice nurses (ARPNs). They have a larger scope of practice and are more independent.
Licensed Practical Nurse (LPN)
An entry-level nursing career, LPNs provide basic care to patients, such as checking vitals and applying bandages. This critical medical function requires vocational or two-year training plus passing a licensure examination.
Neonatal Nurse
This specialization focuses on care for newborn infants born prematurely or that face health issues such as infections or defects. Neonatal nursing requires special skill working with small children and parents.
Nurse Practitioner
A more advanced nursing profession, nurse practitioners engage in more decision-making when it comes to exams, treatments and next steps. They go beyond the reach of registered nurses (RNs) and may work with physicians more closely.
Registered Nurse
Registered nurses are the most numerous in the profession and often serve as a fulcrum of patient care. They work with physicians and communicate with patients and their families. They engage in more sophisticated care than LPNs.
Some of us are lucky enough to stumble into a job that we love. That was the case for Gabrielle Nuki. The 16-year-old had never heard of standardized patients until her advisor at school told her she should check it out.
"I was kind of shocked, and I was kind of like, 'Oh, is there actually something like this in the world?' "
Since Nuki wants to be a doctor, the chance to earn $15 to $20 an hour training medical students as a pretend patient was kind of a dream come true. Every six weeks or so, Nuki comes to Maine Medical Center in her home town of Portland, Maine, slips on a johnny, sits in an exam room and takes on a new persona.
Third-year medical student Allie Tetreault knows Nuki by her fictional patient name, Emma. A lot of teens avoid the doctor, so it's important for Tetreault to learn how to make them feel comfortable.
"What kinds of things do you like to do outside of school?" Tetreault asks.
"Um, I play soccer, so preseason is coming up soon."
Nuki preps weeks ahead of time for her patient roles. She memorizes a case history of family details, lifestyle habits and the tone she should present. "I've had one case where I was concerned about being pregnant. That was kind of like the most harsh one, I guess."
As Emma, Nuki's playing just a shy, healthy teen.
"How did school finish up for you this year?" Tetreault asks.
"Um, it was good. Yeah, school's been good. Um, yeah."
Emma's an easy role, Nuki says, but she ups the shyness factor because it poses a classic challenge to the medical student: how to get a teen to open up?
"Each case kind of has what's on paper, but then you can come in and kind of add another level," Nuki says. "Depending on how complex it is, you can add your own twist to it."
After asking Emma about her personal history, Tetreault moves on to the physical exam and listens as Emma takes deep breaths.
Tetreault gives Emma a clean bill of health and the practice appointment is over. But the most important part of Gabrielle Nuki's job is about to begin.
The 16-year old now has to evaluate the adult professional. She's smooth and tactful after lots of training on how to deliver feedback. Nuki tells Tetreault she did a good job making her feel comfortable.
"I also liked how you mentioned confidentiality, because for my age group, that's important to touch on," Nuki says. "And I think that maybe you could have had a couple more times where you asked me if I had any questions, but other than that I think you did a really great job."
It's communication skills versus acting skills that really qualify someone to be a standardized patient, says Dr. Pat Patterson, the director of pediatric training at Maine Medical Center.
"A lot of patients want to please their physician," Patterson says. "It's not easy for a patient to say 'That didn't feel right', or 'The way you asked that made me feel bad.' "
Gabrielle Nuki says working with medical students and being forthright about their performance has given her more confidence. In the future, she hopes to take on more complex roles — maybe someone with depression.
But she knows no matter what kind of patient she portrays, this job will prepare her well for when she reverses roles and one day becomes a doctor.
For health care workers and researchers, wearing pressurized, full-body suits around Ebola patients may be counterproductive to treating the disease, say three Spanish researchers in a new letter published in the journal The Lancet. But other health experts, wary of wearing less protective gear, disagree.
Health agencies often require that health care workers caring for Ebola patients wear hazardous material (hazmat) suits that protect against airborne diseases. But the Ebola virus rarely spreads through the air, according to the researchers at the University of Valencia and Hospital La Paz-Carlos III, in Madrid.
Ebola is transmitted through contact with infected patients' secretions (such as blood, vomit or feces), and such contact can be prevented by wearing gloves and masks, the researchers wrote.
Wearing full-body protection gear is "expensive, uncomfortable, and unaffordable for countries that are the most affected," they said. It may also send the message that such protection against the virus is being preferentially given to health care workers and is out of reach to the general public, they wrote in their article. [Ebola Virus: 5 Things You Should Know].
Moreover, the image of health care workers in hazmat suits could lead to panic, causing people to flee the area and possibly spread the virus elsewhere, they added.
Instead, protective gear such as gloves, waterproof smocks, goggles, masks and isolated rooms may be enough to manage infected patients, so long as they are not hemorrhaging or vomiting, the letter said. "In control of infectious diseases, more is not necessarily better and, very often, the simplest answer is the best," the researchers wrote.
The current Ebola virus outbreak is the worst in history. It began in February 2014 in Guinea and has since infected people in Liberia, Nigeria and Sierra Leone, killing more than 1,500 people. Just 47 percent of infected patients have survived.
But other experts disagree with the researchers, saying a high level of protection against the virus is needed in places with struggling health care systems, including the countries in West Africa where the outbreak is raging.
"The authors have a point, but I don't think a very strong one," said Dr. William Schaffner, a professor of preventive medicine and an infectious disease specialist at Vanderbilt University Medical Center in Nashville, Tennessee, who was not involved with the letter.
"It must indeed be unsettling for people to see folks in hazmat suits come into their communities," Schaffner told Live Science. "It's very foreign, and often increases their anxiety about events."
But it's better to err on the side of safety, he said. Because the Ebola virus does spread through contact with infected bodily fluids, if health care workers don't immediately clean up such excretions, it's possible these fluids could infect others not wearing appropriate protective gear.
Patients may also start vomiting or bleeding at any time, increasing the risk of infection for health care workers who are not wearing protective suits, he said.
"I would remind us that there are any number of health care workers, including Dr. [Kent] Brantly and Ms. [Nancy] Writebol, were using elaborate equipment in Africa and nonetheless became infected," Schaffner said. (Brantly and Writebol have both since recovered.)
In hospitals with cutting-edge technologies, such as Emory University Hospital, health care workers may not have to wear full-body suits for all Ebola patients, if the patients are on the mend, he said. If they are not displaying symptoms such as vomiting or bleeding, health care workers may be able to scale down their uniforms and use goggles and gloves in lieu of wearing hazmat suits, Schaffner said.
But "when you have a circumstance as hazardous as Ebola, it's important to be secure," Schaffner said.
That's the message from the nation's largest pediatrician group, which, in a new policy statement, says delaying the start of high school and middle school classes to 8:30 a.m. or later is "an effective countermeasure to chronic sleep loss" and the "epidemic" of delayed, insufficient, and erratic sleep patterns among the nation's teens.
Multiple factors, "including biological changes in sleep associated with puberty, lifestyle choices, and academic demands," negatively impact teens' ability to get enough sleep, and pushing back school start times is key to helping them achieve optimal levels of sleep – 8½ to 9½ hours a night, says the American Academy of Pediatrics statement, released Monday and published online in Pediatrics.
Just 1 in 5 adolescents get nine hours of sleep on school nights, and 45% sleep less than eight hours, according to a 2006 poll by the National Sleep Foundation (NSF).
"As adolescents go up in grade, they're less likely with each passing year to get anything resembling sufficient sleep," says Judith Owens, director of sleep medicine at Children's National Medical Center in Washington, D.C., and lead author of the AAP statement. "By the time they're high school seniors, the NSF data showed they were getting less than seven hours of sleep on average."
Chronic sleep loss in children and adolescents "can, without hyperbole, really be called a public health crisis," Owens says.
Among the consequences of insufficient sleep for teens, according to the statement:
Increased risk for obesity, stroke and type 2 diabetes; higher rates of automobile accidents; and lower levels of physical activity.
Increased risk for anxiety and depression; increased risk-taking behaviors; impaired interpretation of social/emotional cues, decreased motivation and increased vulnerability to stress.
Lower academic achievement, poor school attendance; increased dropout rates; and impairments in attention, memory, organization and time management.
Napping, extending sleep on weekends and caffeine consumption can temporarily counteract sleepiness, but they do not restore optimal alertness and are not a substitute for regular, sufficient sleep, the AAP says.
Delaying school start time is a necessary step, but not the only step needed to help adolescents get enough sleep, Owens says. "Other competing priorities in most teenagers' lives are also components of this problem," she says, including homework, after-school jobs, extracurricular activities and electronic media use. Computers and television screens, she adds, "produce enough light to suppress melatonin levels and make it more difficult to fall asleep."
"The bottom line is if school starts at 7:20 there is no way for the average adolescent to get the 8½ to 9½ hours of sleep they need," Owens says
Research on student performance in schools that have reset the start clock, including Minneapolis Public Schools, "shows benefits across the board," says Kyla Wahlstrom, director of the Center for Applied Research and Education Improvement at the University of Minnesota.
"We've found statistically significant evidence that attendance is improved, tardiness is decreased and academic performance on core subjects, English, math, social studies and science, is improved. And now we have evidence that on national standardized tests such as the ACT, there's improvement there, too," Wahlstrom says.
Obstacles commonly cited to changing school start schedules, include curtailed time for athletic practices and games, reduced after-school employment hours for students and significant impact on bus scheduling and other transportation arrangements, she says, adding, "This is a major policy change that schools have to grapple with if they want to embrace the research about what we know about teens."
According to U.S. Department of Education statistics approximately 43% of the more than 18,000 public high schools in the U.S. have a start time before 8 a.m.; just 15% started at 8:30 a.m. or later.
In some school districts that transport students great distances, buses are picking up students as early as 5:45 a.m., "so there's also a safety element" to early start times, says Terra Ziporyn Snider, executive director of the advocacy group Start School Later.
Other major health organizations, including the American Medical Association and the Centers for Disease Control and Prevention, have all highlighted insufficient sleep in adolescents as a serious health risk, as has U.S. Education Secretary Arne Duncan, Snider says.
"What's unique about the American Academy of Pediatrics' statement is that it's very specific," she says. "It says very clearly that high school and middle schools should not start before 8:30 a.m. for the sake of the health and sleep of our children. They draw the red line."
A baby is already a viral sensation and hasn't even born yet. And It's all because of a gesture in an ultrasound photo.
The fetus was captured flashing what looks like the thumbs-up sign in an ultrasound picture taken last week.
The ultrasound image on Reddit was posted on August 28 under the username meancloth, saying "ultrasound result looks good."
Some have nicknamed the baby the "Fonzie fetus," after the iconic cool guy character in the classic television series Happy Days, according to AOL.com.
The father, Brandon Hopkins, told HLN-TV that his wife is expecting twins and the babies are due to arrive in January. The couple will find out the sex of the babies soon. Hopkins said his brother called and told him, 'Your babies are famous'!
The 77-year-old is in the middle stages of Alzheimer's and though she lives on her own, her family keeps close tabs on her. If she leaves her Washington D.C. home between 9 p.m. and 6 a.m., a silent sensor on her front door texts her daughter an alert.
There is a sensor on each of Mary Lou's two key chains that detects when she goes outside her condo's grounds. A motion sensor in the kitchen helps monitor her eating habits, and another in the bedroom notes when she wakes up in the morning and catches any sleeping issues. There is even a flood sensor in the laundry room.
All the sensors are made by SmartThings and relay the information back to a small wireless hub. Her two daughters, who act as her caretakers, can monitor it all on a smartphone app and set up special notifications.
"It's kept her to the point where we haven't even had to have in-home care yet. Our goal is to keep her in her home for as long as possible," said her daughter Cathy Johnson.
Caregivers like Johnson are increasingly turning to smart-home technology and wearable devices to monitor family members with Alzheimer's and dementia, helping them live independently longer. One of the first things Alzheimer's patients lose is the ability to learn new things. It makes getting their bearings and adjusting to a new residence especially difficult. But living alone can pose its own dangers, such as leaving a stove on, wandering off or forgetting to take medication.
"Often, decisions about care are made when safety becomes an issue" said said Beth Kallmyer, vice president of constituent services for the Alzheimer's Association. Tools like these sensors "can allow people to feel more comfortable" and ease the transition.
Finding the right system
SmartThings is a DIY home automation system that connects sensors and smart devices with a wireless hub. In addition to sensors like those in Mary Lou's home, the system can loop in smart thermostats, smart plugs, door locks and surveillance cameras.
SmartThings is highly customizable and works easily with third-party sensors, which makes it appealing to people like Cathy Johnson. It also doesn't require a monthly fee, unlike many other systems. (Samsung recently purchased the company for $200 million.)
The elder care tech industry is still young, but Laurie Orlov, an industry analyst, predicts it could be a $20 billion business by 2020. This means that both startups and big-name brands are getting in on the action.
Lowe's, Home Depot, Best Buy, AT&T and Staples all have their own connected home systems and sell starter kits that you can expand by purchasing sensors à la carte.
Systems Lively and BeClose offer senior-specific accessories such as bed, toilet and pillbox sensors. GrandCare offers connected blood pressure, weight and glucose monitoring devices.
Wearable devices can also track health and behaviors, and built-in accelerometers can pick up on physical changes or tell when a wearer has fallen. Tempo is a wristband for seniors that picks up on lapses in routine or changes in gait that might indicate mental or physical deterioration. The device is due out this winter.
"Pet doors, water heaters, you name it we've either got it connected right now or we're in the process of connecting it," said Kevin Meagher, the vice president and general manager of Lowe's smart-home system, IRIS.
Watching without invading privacy
With any device that collects data, privacy can become an issue.
"We want to respect people's autonomy, respect their desire for how they want their care to go. One of the reasons we think people should get diagnosed early is so they can be a part of the conversation," said Kallmyer.
Phil D'Eramo chose to tell his parents about the Lively system he set up in their senior housing. He uses sensors to make sure they take their pills and tracks how many times his father goes to the bathroom at night, information that gets passed on to his doctor. His father, who has Alzheimer's, said it makes him feel more comfortable to know his son is monitoring him.
It helps that Lively includes a social element that appeals to seniors. Caregivers can upload photos, texts and notes to the Lively app from their phones, and once a month Lively will print out and mail the messages and photos to the seniors in a bright orange envelope.
"I compare it to the analog version of Facebook for seniors," said D'Eramo. "It helps them be connected to the digital social world."
The future of memory care
Connected home and wearable technology isn't enough to replace professional care or personal attention from family members. However, it can extend the amount of time a person is able to live independently, and the technology is constantly improving.
"We're just touching the surface of the technology," said D'Eramo. "I think in the future, the Lively base unit could interact with the person, almost like an electronic caregiver."
Nicknamed “The Flying Squirrel," 6-year-old Quincy Symonds is making waves not only for her incredible surfing skills, but also for her courage while coping with a genetic condition called congenital adrenal hyperplasia.
With a growing social-media following both on Instagram and YouTube, the Australian phenom might just be the best 6-year-old surfer in the world.
“I have never seen a surfer male or female this good at such an early age — and I’ve taught thousands of kids to surf,” her coach, Anthony Pope, told TODAY.com.
In March 2013, when Quincy was 4, she became fascinated by her father's love of surfing, and insisted on doing some of her own. Her mother, Kim Symonds, told TODAY.com it didn't take long for Quincy to find her balance on a surfboard.
“It was just the second or third wave she stood up on, which is apparently quite phenomenal,” she added. “Within a week, she was going across the waves and looking to make turns.”
From a coaching perspective, Pope admitted he had his doubts at the start of their first session, when they swam to 3-foot waves at the surf break known as Currumbin Alley.
"There were a lot of surfers looking at me like, 'You shouldn’t be out here with that tiny kid,'" he said. "However, after pushing her into a perfect 3-foot wave, she took off down the line, tearing the wave up. I was shocked, speechless and super excited. I knew immediately she was something very special."
Pope credits Quincy's success to her fearless nature, exceptional balance and a drive to catch the best wave.
Quincy started making international headlines this month, when Australian media outlet ABC Open featured her serious skills in a Vimeo video that's racked up almost 1 million views. In that video, her father, Jake Symonds, says he still can't believe what he's seeing. "I'm amazed by it," he said. "I'm really proud of it. But, to be honest, I can't comprehend how she does it, and how she's done it so quickly."
It's especially impressive given Quincy's medical condition. According to the Mayo Clinic, congenital adrenal hyperplasia limits adrenal glands' ability to make certain vital hormones.
When Quincy was born, she spent many stints in the intensive-care unit of various hospitals. "On and off, we spent more time in a hospital than we spent at home," Kim Symonds told ABC Open.
The young surfer's health is more stable these days, but because her body doesn’t produce cortisone, she depends on three daily doses of steroids.
Because her illness means she'd require immediate medical care in the event of injury, “We keep emergency medication on hand always,” her mother told TODAY.com.
Despite her condition, Quincy seems fearless when she surfs or skateboards in her family’s hometown on Australia’s Gold Coast, north of Sydney.
That fearlessness led to her nickname, too.
According to ABC Open, when she was younger, she spotted a squirrel in a tree near her house and hopped off her father's SUV to mimic it. "The Flying Squirrel" was born.
As someone who's worked with pro surfers Owen Wright, Dion Agius and Stephanie Gilmore, Pope told TODAY.com he feels "privileged" to work with his young protégée.
"I feel like a better person just knowing Quincy," he said.
Four students at North Carolina State University hope to tackle a problem on many campuses by developing a nail polish that can detect so-called date rape drugs by changing colors when it comes into contact with them.
Women who wear the polish can simply swirl their fingers in a drink to test it for any colorless, odorless compound that may have been slipped in.
The four male entrepreneurs behind the product, which they call Undercover Colors, have received mainly positive responses. They won an $11,000 prize from a contest on campus, where they also have met with a potential investor.
A White House report estimates one in five women has been sexually assaulted while at college, but only 12 percent of those student victims ever report the crime.
“As a rape victim, and a mother of 3 daughters, I can not thank you enough,” one fan said in a post on the group's Facebook page, which has been “liked” by more than 26,000 users.
But some have expressed skepticism about the product, however well-intentioned it may be.
"I think it reflects the cultural reality where we actually put the blame on women,” often when they are the victims of rape,” said Elizabeth Plank, a senior editor at Mic. “We put the onus on them, to prevent rape, when we very well know that this is not an effective way of actually reducing sexual assault."
North Carolina State has encouraged the students to continue pursuing their project, providing them with lab space to experiment. It’s not clear when the nail polish will be available on the market.
At Boston Children’s Hospital, doctors perform practice surgeries with replicas of their patients’ body parts. Though the hospital has had a simulation program for about a decade, it started 3D-printing children’s body parts about a year ago, said Dr. Peter Weinstock, director of the hospital’s simulator program.
“They perfect what they want to do before ever bringing the child into the operating room or putting them to sleep,” Weinstock said.
The models are also used to help parents understand their children’s surgeries before the operation and to educate students afterward, Weinstock said.
The printer is precise, with a resolution of between 16 and 32 microns per layer. That means each layer is about the width of a “filament of cotton,” Weinstock said. And since the printer can print multiple resins or textures, doctors can work on replicas that model different tissue types, like brain matter and blood vessels.
The printer only takes a few hours to do their work once CT scans and other forms of imaging are collected and rendered into 3D models. A child’s finger might take three hours to print, but a chest replica they made last week took longer, Weinstock said.
The team has already printed about 100 body parts over the last year and demand is growing, Weinstock said, adding that the printer is running around the clock.
Dr. Ed Smith, a pediatric neurosurgeon at Boston Children’s, said he recently used several different 3D models to perform brain surgery on a 15-year-old patient with an abnormal cluster of veins above his optical nerve. One wrong maneuver and the patient could have gone blind.
He even used a see-through replica of the patient’s skull on a light box in the operating room as a reference.
“It’s kind of like being superman with X-ray vision where you can actually hold this up and see right through it,” Smith said.
The surgery, which would have normally taken five or six hours, wound up clocking in at 2 hours and 20 minutes, Smith said.
Though Boston Children’s hasn’t conducted any formal studies of how the models help surgeons, Smith said he’s heard anecdotally that they result in shorter surgeries because doctors know what to expect.
If something good could come out of the Boston Marathon bombing, James Costello and Krista D'Agostino seem to have found it.
Sixteen months after the attack killed three people and injured more than 260, including Costello, he married D'Agostino, the nurse who helped him recover. The couple exchanged vows Saturday at the Hyatt Regency Boston in front of about 160 guests.
A photograph of Costello with his clothes ripped to shreds and parts of his body burned became one of the most recognized images of the 2013 attack. He met D'Agostino, a nurse at Spaulding Rehabilitation Hospital, while he was recovering from multiple surgeries for shrapnel injuries and serious burns that required pig skin grafts on his right arm and right leg.
After the couple became engaged, Costello said he believed he was involved in the tragedy in order to meet D'Agostino, whom he described as his best friend and the love of his life.
"One thing that she hates that I always say is I'm actually glad I got blown up," Costello said on the "Today" show in December. "I wish everyone else didn't have to, but I don't think I would have ever met her if I didn't."
Wedding planner Rachael Gross said she and the other vendors involved in the wedding donated their services.
"They are the most gracious, generous, kind, ... loving couple," Gross said. "They believe that they were meant to meet."
The wedding ceremony was held outdoors on the hotel's third-floor terrace, with blue and white hydrangeas all around. The reception was held in the hotel's grand ballroom.
"It was more like a classic Nantucket style, but without a literal nautical theme," Gross said.
Costello, of Malden, was gathered with friends near the marathon finish line, watching for another friend who was running when two bombs exploded within seconds of each another. Three of Costello's friends lost a leg, while other friends suffered burns and shrapnel injuries.
During his two-week stay at Massachusetts General Hospital, Costello was among patients who met President Barack Obama. He was later transferred to Spaulding.
Costello and D'Agostino, both 31, are honeymooning in Hawaii.
Emergency department nurses aren't like the rest of us - they are more extroverted, agreeable and open - attributes that make them successful in the demanding, fast-paced and often stressful environment of an emergency department, according to a new study by University of Sydney.
"Emergency nurses are a special breed," says Belinda Kennedy from Sydney Nursing School, a 15 year critical care veteran who led the study.
"Despite numerous studies about personalities of nurses in general, there has been little research done on the personalities of nurses in clinical specialty areas.
"My years working as a critical care nurse has made me aware of the difficulty in retaining emergency nurses and I have observed apparent differences in personality among these specialty groups. This prompted me to undertake this research which is the first on this topic in more than 20 years.
"We found that emergency nurses demonstrated significantly higher levels of openness to experience, agreeableness, and extroversion personality domains compared to the normal population.
"Emergency departments (ED) are a highly stressful environment - busy, noisy, and with high patient turnover. It is the entry point for approximately 40 per cent of all hospital admissions, and the frequency and type of presentations is unpredictable.
"Emergency nurses must have the capacity to care for the full spectrum of physical, psychological and social health problems within their community.
"They must also able to develop a rapport with individuals from all age groups and socioeconomic and cultural backgrounds, in time-critical situations and often at a time when these individuals are at their most vulnerable.
"For these reasons, ED staff experience high levels of stress and emotional exhaustion, so it's understandable that it takes a certain personality type to function in this working environment.
"Our research findings have potential implications for workforce recruitment and retention in emergency nursing.
"With ever-increasing demands on emergency services it is necessary to consider how to enhance the recruitment and retention of emergency nurses in public hospitals. Assessment of personality and knowledge of its influence on specialty selection may assist in improving this.
"The retention of emergency nurses not only has potential economic advantages, but also a likely positive impact on patient care and outcomes, as well as improved morale among the nursing workforce," she said.
Since this article is from Aulstralia, do you agree that Emergency Room Nurses in the US should have the same characteristics to be successful in a US Emergency Room?
Inside the operating room, video cameras track every movement. Outside, a small computer-like device analyzes the recordings, identifying when mistakes are made and providing instant feedback to surgeons as they operate.
This is the dream of the surgical "black box." Operations could become flawless. Post-operative complications could be significantly reduced. Surgeons could review the footage to improve their technique and prep for the next big case.
Such a device isn't far from reality.
Researchers in Canada are working on a surgical tracking box -- like the ones placed in airplanes -- that records surgeons' movements and identifies errors during an operation.
By pinpointing mistakes and telling surgeons when they're veering "off course," a black box could prevent future slip-ups, says Dr. Teodor Grantcharov, a minimally invasive surgeon at St. Michael's Hospital in Toronto. Unlike the so-called black boxes in aviation, which are used after disasters occur, the surgical black box Grantcharov is creating will be used proactively to prevent major patient complications.
A number of hospitals have already expressed interest in using the device, Grantcharov says.
But the litigious medical environment may make its implementation problematic. If the recordings were used in court, they could open the floodgates to a new wave of malpractice concerns, which would be counterproductive to surgeons and patients, Grantcharov says.
"We have to ensure the black box is used as an educational tool to help surgeons evaluate their performance and improve," he says.
A work in progress
Grantcharov's black box is a multifaceted system. In addition to the actual box, it includes operating room microphones and cameras that record the surgery, the surgeon's movements and details about team dynamics.
It will allow surgeons to hone in on exactly what went wrong and why.
The black box will eventually assess everything from how surgeons stitch to how delicately they handle organs and communicate with nurses during high-stress situations. Error-analysis software within the black box will help surgeons identify when they are "deviating" from the norm or using techniques linked to higher rates of complications.
So far, Grantcharov's black box has been tested on about 40 patients undergoing laparoscopic weight-loss surgery.
"At this initial stage, we are analyzing surgeries to determine how many errors occur and which ones actually lead to bad results for patients," Grantcharov says. Not every error will result in a patient complication.
Grantcharov's initial research has shown that surgeons recognize few of their mistakes, and, on average, make about 20 errors per surgery -- regardless of experience level. Once Grantcharov's team determines which errors affect patient safety, it hopes to be able to provide this information to surgeons in real time. The team has also developed software that can synthesize the recorded data into user-friendly and interpretable information for surgeons.
The concept of using a black box in surgery isn't new. But until now, the technology never made it out of the laboratory because it lacked comprehensiveness, Grantcharov says. Earlier surgical black boxes didn't record all the important elements of the operating room, he says, leaving pieces of the puzzle missing.
"To truly understand what causes an error, you need to know all the factors that may come into play."
Recording mistakes
Grantcharov was inspired to develop the surgical black box after years of witnessing how patient complications affected surgeons.
"The feeling of not knowing what causes a complication, whether it's surgical technique, communication in the operating room or the patient's condition itself, is tormenting," Grantcharov says.
Many surgeons, however, may be uncomfortable with using a black box in the operating room, saysDr. Teodoro Forcht Dagi with the American College of Surgeons Perioperative Care Committee.
"If there was a legal requirement to record every operation, then many surgeons would be resistant," Forcht Dagi says. He says he believes doing so would create a sense of nervousness that would paralyze a surgeon's ability to operate and end up ultimately harming patients.
"The black box needs to be used solely by surgeons for their own education, in which case I think it's a great idea," Forcht Dagi says.
Errors during surgery have generally been dealt with after the fact, and only once a complication during the patient's recovery occurs. Weeks after surgery, cases with complications are presented to a panel of experts, who weigh in on what may have gone wrong during the operation.
Yet in many cases nothing is recorded apart from an audio transcript of the operation, making it tough to identify what caused each complication. The black box would add much needed context.
"I would rush (a black box) into service immediately," says Richard Epstein, professor of law at New York University's School of Law. Since most medical lawsuits end up being "he said, she said" arguments, not knowing exactly what happened in the operating room just adds to the level of distrust, Epstein says.
In the United States, the Healthcare Quality Improvement Act prevents courts from using data that doctors and hospitals use for peer review, a self-regulation process in which experts or "peers" evaluate one another. The law allows doctors to assess each other openly and identify areas for improvement without fear of litigation.
But there are exceptions to this rule, says William McMurry, president of the American Board of Professional Liability Attorneys. For instance, cases where surgeries are recorded but don't receive any peer review can be used in court.
While McMurry says that "keeping patients in the dark about the details of their surgery is never OK," he points out that litigation concerns should not derail use of the black box. It will be an asset to the health care system regardless of whether it can be used in court, he says.
"We care about better health care, and the black box will provide surgeons with the information they need to avoid mistakes," McMurry says. "It's a win-win situation."
The surgical black box will be tested in hospitals in Canada, Denmark and parts of South America in the next few months. Talks are also under way with a number of American hospitals.
If doctors accept it, implementation in U.S. hospitals could happen quickly since the surgical black box isn't considered a medical device and doesn't require approval from the U.S. Food and Drug Administration.
Bottom line, Grantcharov says, is that even after years of practicing medicine, the black box "made me a safer surgeon and a better teacher."
"People tend to think that happiness in schizophrenia is an oxymoron," says senior author Dr. Dilip V. Jeste, distinguished professor of Psychiatry and Neurosciences at the University of California, San Diego School of Medicine.
"Without discounting the suffering this disease inflicts on people, our study shows that happiness is an attainable goal for at least some schizophrenia patients," he adds. "This means we can help make these individuals' lives happier."
Dr. Jeste's team surveyed 72 schizophrenia outpatients in the San Diego area - all but nine of whom were taking at least one anti-psychotic medication. Just over half of the respondents were residents in assisted-living facilities.
A comparison group was comprised of 64 healthy men and women who did not currently use alcohol or illegal drugs and who had not been diagnosed with dementia or other neurological illnesses.
The mean age for both groups was 50 years.
In the survey, the respondents answered questions on their happiness over the previous week. They were asked to rate statements such as "I was happy" and "I enjoyed life" on a scale from "never or rarely" to "all or most of the time."
The results reveal that about 37% of the schizophrenia patients were happy most or all of the time, compared with about 83% of respondents in the comparison group.
However, about 15% of people in the schizophrenia group reported being rarely or never happy, but no one in the comparison group reported such a low level of happiness.
'Patients' happiness was unrelated to the severity or duration of their illness'
The researchers compared the self-reported happiness of the respondents with other factors including age, gender, education, living situation, medication status, mental health, physical health, cognitive function, stress, attitude toward aging, spirituality, optimism, resilience and personal mastery.
The study - which is published in the journal Schizophrenia Research - suggests that the patients' levels of happiness were unrelated to the severity or duration of their illness, cognitive or physical function, age or education. This is clinically significant because, among healthy adults, all of these factors are associated with a greater sense of well-being.
Lead author Barton W. Palmer, PhD, professor in the UC San Diego Department of Psychiatry summarizes the study's findings:
"People with schizophrenia are clearly less happy than those in the general population at large, but this is not surprising.
What is impressive is that almost 40% of these patients are reporting happiness and that their happiness is associated with positive psychosocial attributes that can be potentially enhanced."
The teenage years can be tough enough under the best of circumstances. But when cancer invades an adolescent’s life, the challenges grow exponentially.
When the prospects for treatment are uncertain, there’s the fear of dying at so young an age. Even with an excellent chance of being cured, teenagers with cancer face myriad emotional, educational and social concerns, especially missing out on activities and losing friends who can’t cope with cancer in a contemporary.
Added to that are the challenges of trying to keep up with schoolwork even as cancer treatment steals time and energy, and may cause long-lasting physical, cognitive or psychological side effects.
Sophie, who asked that her last name be withheld, was told at 15 that she had osteosarcoma, bone cancer. After a bout of how-can-this-be-happening-to-me, she forged ahead, determined to stay at her prestigious New York high school and graduate with her class.
Although most of her sophomore year was spent in the hospital having surgery and exhausting chemotherapy, she went to school on crutches whenever possible. She managed to stay on track, get good grades — and SAT scores high enough to get into Cornell University.
Now 20, Sophie is about to start her junior year and is majoring in biology and genetics with a minor in computer science. She plans to go to medical school, so this summer she has been studying for the MCATs and volunteering at a hospital.
Her main concern now is that people meet and get to know her as a whole, normal person, not someone who has had cancer, which is why she asked that I not identify her further.
“I’m pretty healthy, and I don’t want people to think I’m weak and need special care,” she said in an interview.
“Having cancer puts other issues into perspective,” she added. “I feel like I have to do as much as I can. I’ve gotten involved in so much. I try to enjoy myself more. And I don’t regret for a minute how I’ve been spending my time.”
Sophie’s determination to do the most she can and her desire for normalcy are hardly unusual, said Aura Kuperberg, who directs an extraordinary program for teenagers with cancer and their families at Children’s Hospital Los Angeles. Dr. Kuperberg, who has a doctorate in social work, started the program, called Teen Impact, in 1988. It operates with the support of donations and grants and deserves to be replicated at hospitals elsewhere.
“The greatest challenge teens with cancer face is social isolation,” she said in an interview. “Many of their peers are uncomfortable with illness, and many teens with cancer may withdraw from their friends because they feel they are so different and don’t fit in.”
In the popular young adult novel “The Fault in Our Stars,” a teenager with advanced cancer says, “That was the worst part of having cancer, sometimes: The physical evidence of disease separates you from other people.”
Within the family, too, teenagers can feel isolated, Dr. Kuperberg said. “Patients and parents want to protect one another. They keep up a facade that everything will be O.K., and feelings of depression and anxiety go unexpressed.”
Teen Impact holds group therapy sessions for young patients, parents and siblings so they “don’t feel alone and realize that their feelings are normal,” Dr. Kuperberg said. The goal of the program, which also sponsors social activities, is to help young cancer patients — some still in treatment, others finished — live as normally as possible.
“For many, cancer is a chronic illness, with echoes that last long after treatment ends,” Dr. Kuperberg said. “There are emotional side effects — a sense of vulnerability, a fear of relapse and death, and an uncertainty about the future that can get in the way of pursuing their hopes and dreams. And there can be physical and cognitive side effects when treatment leaves behind physical limitations and learning difficulties.”
But, she added, there is often “post-traumatic growth that motivates teens in a very positive way.”
“There’s a lot of altruism,” she said, “a desire to give back, and empathy, a sensitivity to what others are going through and a desire to help them.”
Sophie, for example, took notes for a classmate with hearing loss caused by chemotherapy. She recalled her gratitude for the friend “who was there for me the whole time I was in treatment, who would come over after school and sit on the couch and do puzzles while I slept.”
One frequent side effect of cancer treatment now receiving more attention is the threat to a young patient’s future reproductive potential.
In an opinion issued this month, The American College of Obstetricians and Gynecologists urged doctors to address the effects of cancer treatment on puberty, ovarian function, menstrual bleeding, sexuality, contraceptive choice, breast and cervical cancer screening, and fertility.
“With survival rates pretty high now for childhood cancers, we should do what we can to preserve future fertility,” said Dr. Julie Strickland, the chairwoman of the college’s committee on adolescent health care. “We’re seeing more and more cooperation between oncologists and gynecologists to preplan for fertility preservation before starting cancer treatment.”
The committee suggested that, when appropriate, young cancer patients be referred to a reproductive endocrinologist, who can explore the “full range of reproductive options,” including the freezing of eggs and embryos.
For boys who have been through puberty, it has long been possible to freeze sperm before cancer treatment.
Although some female patients may be unwilling to delay treatment, even for a month, to facilitate fertility preservation, at the very least they should be offered the option, Dr. Strickland said in an interview.
She described experimental but promising possibilities, like freezing part or all of an ovary and then implanting it after cancer treatment ends. It is already possible to move ovaries out of harm’s way for girls who need pelvic radiation.
Many children get anxious or afraid when they have to get a vaccination, but there are a number of ways that parents can make these shots easier for their kids, an expert suggests.
The first step is to explain to children in an age-appropriate way that the vaccinations help protect their health, said Rita John, director of the pediatric primary care nurse practitioner program at Columbia University School of Nursing in New York City.
"Children need to know that vaccines aren't a punishment or something negative, vaccines are something that keeps them from getting sick," John said in a Columbia news release. "When parents are anxious, they pass that fear on to their kids. The best way to talk about vaccines is to keep the conversation positive and focused on the benefits of vaccination."
Before a vaccination, you can reduce toddlers' and preschoolers' anxiety if you give them a toy medical kit so that they can give pretend shots to you or a favorite doll or other toy.
When you arrive for the shot, ask the clinician to use a numbing cream or spray to limit the pain caused by the needle. Blowing on a bubble maker or a pinwheel can help distract younger children during vaccinations, while listening to music, playing games or texting may benefit older children and teens.
"If the kids think something is going to reduce their pain, there can be a placebo effect where the technique works because they expect it to work," John explained.
"It doesn't matter so much what you use to make your child more comfortable so long as you do something that acknowledges that they may experience some pain and that they can do something to make it hurt less," she added.
Be sure to reward and/or praise children after a vaccination. For example, give stickers to younger children. "You want the final part of the experience to make kids feel like even if they suffered some momentary pain, it was worth it," John said.
"Good play preparation, a positive attitude about immunization, and bringing something to distract kids during the shots can all help make the experience better," she concluded.
Surgeons in Beijing, China, have successfully implanted an artificial, 3D-printed vertebra replacement in a young boy with bone cancer. They say it is the first time such a procedure has ever been done.
During a five-hour operation, the doctors first removed the tumor located in the second vertebra of 12-year-old Minghao's neck and replaced it with the 3D-printed implant between the first and third vertebrae, CCTV.com reported earlier this month.
"This is the first use of a 3D-printed vertebra as an implant for orthopedic spine surgery in the world," said Dr. Liu Zhongjun, the director of orthopedics at No. 3 Hospital, Peking University, who performed the surgery.
The boy was playing football when he headed the ball and injured his neck, and it was later confirmed that he had a tumor, Minghao's mother said.
Prior to the surgery, the patient had been lying in the orthopedics ward for more than two months, and he could occasionally stand up, but only for a few minutes.
Normally, a diseased axis would be replaced by a standardized, hollow titanium tube, Liu told Reuters.
"Using existing technology, the patient's head needs to be framed with pins after surgery," as his head cannot touch the bed when he is resting for at least three months, he explained. "But with 3D printing technology, we can simulate the shape of the vertebra, which is much stronger and more convenient than traditional methods."
Five days after the surgery, Minghao still could not speak and had to use a writing board to communicate. However, doctors said at the time that he was in a good physical condition and they expected him to make a strong recovery.
Roger Corcoran has been a window washer for 35 years. But on Wednesday, he was Batman.
The 61-year-old grandfather of two rappelled down the side of Mayo Clinic Children’s Center alongside Spiderman and Superman.
“When a kid wanted to know why I was so old, I told him I played the original batman,” Corcoran said with a chuckle.
John Carroll, 48, dressed up as Spiderman.
“It’s one thing I look forward to doing all year,” said Carroll, who has worked as a window washer for 15 years.
After rappelling down the side of the building, Carroll and Corcoran went inside to meet the kids, who were appropriately shocked to come face-to-face with their high-flying heroes.
“The first time it happened, I was kinda crying because it means a lot to those kids,” Carroll said.
Carroll and Corcoran work at ISS Facility Services, which washes windows for Mayo Clinic. Charlie Kleber worked with Mayo Clinic to set up the special event, and said he picked some of his best guys to swing down and make the kids smile.
He said he’s watched even the sickest kids come alive when they’re face-to-face with the superheroes.
He called Wednesday’s superhero experience “life-changing,” and said they were all struck by a special patient: 13-year-old Claire Strawman, who in April became the youngest heart-lung patient Mayo Clinic had ever transplanted.
She told them about how she went into lung failure and underwent a transplant in April. She was hospitalized for about seven months before being released a few weeks ago. But she got sick on Monday and needed to come back.
“I got goose bumps right now telling you that story,” Kleber said.
Claire is on immunosuppressant drugs to prevent her from rejecting the new organs, but the drugs also make her more prone to infections. When she got sick, her parents worried and brought her back to the hospital, according to her mom, Ellen Strawman. She was in the pediatric ICU when the superheroes visited.
“Just seeing them put a big smile on her face,” Strawman said, adding that Claire left the hospital today for her home in Bloomington, Minnesota.
“She told us what happened to her and everything. We were all standing around her tearing up,” Carroll said. “That story made you feel so proud to do it for the kids because it means so much to them. It was great.”
Disabilities among U.S. children have increased slightly, with a bigger rise in mental and developmental problems in those from wealthier families, a 10-year analysis found.
Disadvantaged kids still bear a disproportionate burden.
The increases may partly reflect more awareness and recognition that conditions, including autism, require a specific diagnosis to receive special services, the researchers said.
Meantime, physical disabilities declined, as other studies have suggested.
The study is the first to look broadly at the 10-year trend but the results echo previous studies showing increases in autism, attention problems and other developmental or mental disabilities. It also has long been known that the disadvantaged are more likely to have chronic health problems and lack of access to good health care, which both can contribute to disabilities.
The researchers studied parents' responses about children from birth through age 17 gathered in 2000-2011 government-conducted health surveys. Parents were asked about disabilities from chronic conditions including hearing or vision problems; bone or muscle ailments; and mental, behavioral or developmental problems that limited kids' physical abilities or required them to receive early behavioral intervention or special educational services. Nearly 200,000 children were involved.
Results were published online Monday in Pediatrics.
Overall, disabilities of any kind affected 8 percent children by 2010-2011, compared to close to 7 percent a decade earlier. For children living in poverty, the rate was 10 percent at the end of the period, versus about 6 percent of kids from wealthy families.
The overall trend reflects a 16 percent increase, while disabilities in kids from wealthy families climbed more than 28 percent, the researchers found. The trend was fueled by increases in attention problems, speech problems and other mental or developmental disorders that likely include autism although that condition isn't identified in the analyzed data.
Declines in asthma-related problems and kids' injuries accounted for much of the overall 12 percent drop in physical disabilities. Better asthma control and treatment and more use of bike helmets, car seats and seat-belts may have contributed to that trend, said lead author Dr. Amy Houtrow, a pediatric rehabilitation specialist at the University of Pittsburgh.
The developmental disability increases echo what Dr. Kenneth Norwood, a developmental pediatrician in Charlottesville, Virginia sees in his medical practice.
"I'm routinely backed up six months for new patients," said Norwood, chairman of the American Academy of Pediatrics' Council on Children with Disabilities.
Norwood thinks there is more awareness of these conditions and that some, including autism, are truly rising in prevalence. Autism is thought to result from genetic flaws interacting with many other factors. Some studies have suggested these may include parents' age and prenatal infections.
Parkinson's disease is like a "rolling wave" of ever-changing symptoms, not a lightning strike of different events, says its most famous patient, the actor Michael J. Fox.
So when doctors ask for a list of recent symptoms, they miss a lot of the subtleties of the progressive disease.
Hoping to change that, the Michael J. Fox Foundation and Intel announced Wednesday that they are collaborating on a project to track Parkinson's patients 24/7.
Using a device like the popular FitBit (a wristband activity monitor), patients will be tracked over the course of their day, as their medication kicks in and wears off, as food hits their system, as their environment changes and as they sink into sleep. The data generated will be so enormous that Intel's digital expertise will be needed to make sense of it, both organizations said.
The information should lead to new insights into a disease diagnosed in about 60,000 Americans a year, leading to tremors, paralyzing stiffness and physical awkwardness, among other symptoms.
"The answers are within us," Fox said in an interview. "We just need to find a way to let people into our brains both literally and figuratively to help us figure this out."
The collaboration, which started with a small pilot trial of 25 people this spring, aims to measure patient gait, tremors and sleep patterns, among other metrics, and stream the data in real time to the cloud. Intel, which provided the servers and software to collect and manage the data, is also developing algorithms to help analyze it, said Diane Bryant, senior vice president and general manager of Intel's Data Center Group.
Former Intel CEO Andrew Grove has had Parkinson's since 2000, and initiated the discussion between the company and the foundation, Bryant said.
The company isn't disclosing how much it is investing in the project, but Bryant said that costs for this kind of effort have fallen dramatically in recent years. "Ten years ago it would have been ridiculous to consider" a project like this, she said.
The collaboration is Intel's first step into health care, but it likely won't be the last.
"It's a wonderful first step for us," Bryant said. Health care lends itself well to so-called big-data analytics, because there is so much information to collect on a patient, from symptoms to genetics to lab results.
Fox Foundation CEO Todd Sherer said doctors score the disease's severity based on how the patient feels during a visit – but symptoms can change minute by minute, from near normal to completely disabling.
"If the doctor is running 15 minutes late, the assessment could be completely different than if they'd seen the disease 15 minutes earlier," Sherer said.
Also, he said, sometimes patients minimize symptoms for their doctor, or time their medication so they'll perform well during the visit. "The doctor might say everything's doing great, and we'll hear from the spouse: 'You should have seen them yesterday.' "
The same problems also make research into the disease more difficult. It's hard for researchers to get a realistic view of whether a treatment is effective, if they only get occasional snapshots of a patient.
The new devices will therefore provide a much more realistic – and objective – view of the disease than has been possible before, Sherer said.
If shown effective during pilot studies, he said, the devices will likely be used both for clinical research trials – in which the patient data will be anonymous – and, say, for a week before a doctor's visit, to provide an update on a patient's disease.
School nursing started out as a practical solution for Beth Mattey: The mom of three liked the hours. Now, 27 years later, she says it was the perfect career choice—creative, independent and full of meaning. “As Maya Angelou said, ‘People never forget how you made them feel,’” Mattey says. “That’s the connection that school nurses make.” We asked Mattey what parents might be surprised to know about her job—and their kids.
1. Sadness is one of the most common illnesses she sees in students. “Kids are anxious and want to do well,” she says, noting a 2012 National Association of School Nurses report that the top five health conditions of U. S. children are mental health- related, issues that school nurses spend about a third of their time helping students cope with.
2. Every kid should carry a water bottle. Dehydration is often the cause of headaches, another common complaint among kids, Mattey says. Also a culprit? Lack of sleep.
3. School nurses need to know your secrets. In addition to any chronic conditions your student is coping with, update your school’s nurse on any big family news like an illness, death or divorce. Your instinct might be to keep such facts private, but the nurse can offer your child valuable support.
4. Your kids aren’t eating the lunch you pack. “I often ask teens what they had for lunch, and they say, ‘Chips.’ We need to help them understand the value of nutrition and to make good choices,” Mattey says.
5. A “mental health day” is not a stress solution. Allowing your anxious teen a day off won’t get to the root of the cause. “If a kid is too stressed to go school, find out why,” Mattey says. “Is she being bullied? Did she not do her homework?”
6. Teens need vaccines. Make sure yours is up to date on the Tdap or tetanus, diphtheria, pertussis; meningitis—one at age 11, the second at age 16; and the HPV (human papilloma virus).
7. A school nurse can be a teen’s— and parent’s—best friend. Mattey sees herself as supporting students, physically and emotionally. After all, she’s there day after day, year after year. “School nurses provide a safety net,” she says.
Sometimes, being part of the nursing profession can feel exactly the same as being part of a family. You love it dearly, you can’t imagine your life without it, but there are lots of things about nursing (and family) that can drive the most balanced person completely nuts.
Deep down, you love nursing, even with all of its vein-popping, blood pressure elevating quirks.
Here is Scrubbed In’s list of things about nursing that drive nurses absolutely nuts, but we deal with anyway.
1. Call lights: Of course the purpose of call lights is to enable patients to get help when needed, but it’s hard not to get annoyed at the call light itself. It’s blinking, beeping, and taunting you because you just sat down to document. (See #2)
2. Documentation: For the love of all things nursing. Documentation is our greatest tool and the bane of our existence, all wrapped up into a flowchart, and an I&O’s chart, a nursing note, an incident report, a pre-anesthesia evaluation form, a…
3. (For our guys) Being called “male nurse:” For the men in our nursing community, hearing someone refer to them as a nurse, without “male” automatically attached, would be a breath of fresh air.
4.Body fluids: Nurses deal with body fluids all the time. It’s par for the course. But it’s not exactly something one wishes for. We don’t need to name them all. You’re well acquainted with most. They can really dampen your day. Pun intended.
5. Waving your ID to get into your bathroom at home: Many healthcare facilities have areas where you need to scan your ID to unlock the door. When you’ve tried that to get into your bathroom at home, it might be time to take a vacation.
6. Trying to use your fingerprint at the ATM: If you regularly use your fingerprint to get into medication and supply stations, you might find yourself trying to do the same at the ATM screen. Just hope that no one saw you.
7.Hearing a patient-alarm-like sound (outside of work): You’re out and about and someone’s cell phone ring sounds uncannily like an O2 sat alarm. Before you’ve had a chance to process, your pulse has quickened and you’re on high alert. Calm down, nervous system; you’re off duty today.
8.Patients who don’t take the full course of antibiotics: When a patient gaily reports that they stopped taking their antibiotics because they feel sooo much better, there’s a specific protocol you must follow. It involves closing your eyes, taking deep breaths and counting to 10 before calmly explaining the rationale behind completing the course in full.
9.Waking up at 5 a.m. on your day off: Finally, finally you can sleep in. You’ve been looking forward to it for days. But your brain seems determined to wake up as if you need to work today. At least you can stay in bed with your feet up.
10.Bringing a coffee to work, then drinking it cold four hours later: A hot cup of coffee at the start of your day is one of the simple pleasures of life. But did you really think you were going to drink it? You might at some point, it just may be more like iced coffee by then.
Inappropriate configurations of clinical alarm settings are more than just a nuisance for frontline staff, according to ECRI Institute's accident investigators.
Improper changes to preconfigured alarm settings have resulted in serious patient harm or death when caregivers weren't alerted to significant changes in patient conditions. This doesn't need to persist.
Findings from these investigations have raised concerns that many healthcare organizations do not have effective policies on configuring and managing clinical alarm settings. Establishing effective policies for setting of clinical alarms and putting a system in place to effectively follow these policies is critical to patient safety.
To educate healthcare facilities about the challenges clinicians are facing when configuring physiologic monitor alarms, ECRI Institute is presenting an educational web conference, "Good Alarm Policies are No Accident," on Wednesday, Sept. 3.
The objectives of the webinar, according of ECRI, are to help participants:
Comprehend ways to improve alarm-setting policies for successful compliance with the Joint Commission's National Patient Safety Goal on alarm safety.
Realize what to expect when planning and designing patient care areas.
Recognize how leading healthcare organizations have improved alarm-setting processes to improve patient safety.
Understand lessons learned from our accident investigations related to alarms.
The ECRI webinar is intended for risk managers, clinical staff, nursing administration, ICU staff, clinical department heads, clinical and biomedical engineers, materials managers, and other healthcare professionals. The interactive format of ECRI Institute's webinar will provide ample time to interact with the panel during the Q&A session and also encourages participation. Panelists and speakers include:
Michael Argentieri, MS, Vice President & Senior Investigator, ECRI Institute Mark E. Bruley, CCE, Vice President, Accident and Forensic Investigation, ECRI Institute (Q&A only) Maria Cvach, DNP, RN, Assistant Director of Nursing, Clinical Standards, The Johns Hopkins Hospital Sue Sendelbach, PhD, RN, CCNS, FAHA, FAAN, Director of Nursing Research, Abbott Northwestern Hospital Stacy Jepsen, APRN, CNS, CCRN, Clinical Nurse Specialist, Critical Care, Abbott Northwestern Hospital Moderator: Jeremy Suggs, PhD, Engineering Manager, Health Devices, ECRI Institute
It may be warm in parts of the country, but some people aren’t drenching themselves in ice or cold water to cool down from elevated temperatures. A new phenomenon has hit the social media circuit – the “Ice Bucket Challenge.”
The challenge involves people getting doused with buckets of ice water on video, posting that video to social media, then nominating others to do the same, all in an effort to raise ALS awareness. Those who refuse to take the challenge are asked to make a donation to the ALS charity of their choice.
Beverly, Mass., resident Pete Frates, started the “Ice Bucket Challenge” with his family on the social sites Facebook and Twitter. Frates, 29, has lived with ALS since 2012, and he has worked with The ALS Association’s Massachusetts Chapter. A former Division 1 college athlete with Boston College Baseball, Frates tirelessly spreads awareness of Lou Gehrig’s Disease.
This viral sensation, which has used the hash tag #IceBucketChallenge, has attracted thousands of followers, including Boston Bruins stars Brad Marchand and Torey Krug, who willingly dropped frozen ice on themselves and issued the challenge to others.
“This is a creative way to spread ALS awareness via social media and in communities nationwide,” said Barbara Newhouse, President and CEO of The ALS Association. “We thank Pete Frates and his family for getting so many people involved in spreading the word about ALS.”
By the time her third daughter was born last year, Gabriella McCann thought she was an old pro at handling new babies.
But nothing in her experience with Greta, now 6, or Stella, 3, could have prepared her for Elisa, who arrived missing a puzzling patch of skin on the back of one hand. Within 24 hours, that patch was followed by blisters that erupted on Elisa’s body — and stumped doctors who didn’t know what to make of the shocking condition.
“The baby was born and the whole world crashed,” recalled McCann, 40, a Minneapolis mom who was staying with family and friends in her native Palermo, Italy, when Elisa was born.
Within days, the problem was clear. Doctors in Rome diagnosed Elisa with a form of epidermolysis bullosa, or EB, a genetic disorder in which layers of the skin don’t anchor together properly, causing friction that leads to massive, painful blistering at the slightest scrape or bump.
“They actually look like burn blisters,” McCann said. “She had blisters surrounding her fingers so that they looked like hot dogs in a bun.”
Today, however, 18-month-old Elisa’s fingers look almost normal. Her mother has taken off the gloves and wraps that covered her hands and feet and she’s even allowing the toddler to experiment with walking — even if it means she falls.
That’s because in May, Elisa became the 28th child enrolled in a ground-breaking clinical trial at the University of Minnesota that uses bone marrow from healthy donors — in this case, Elisa’s sister Stella — to repair the symptoms of the devastating disorder.
Led by Dr. Jakub Tolar, director of the university’s Stem Cell Institute, the trial begun in 2007 is still considered experimental but has become the treatment of choice for the most severe cases of EB, he said.
“This is one of the most difficult to treat disorders and a very painful disorder,” Tolar said. “Before we started, there was absolutely nothing that would change the outcome of these children.”
EB is caused by a defect in the genes that make collagen, a connective tissue that allows skin layers to adhere to each other, Tolar said.
“It’s a protein that makes loops that are like Velcro that attach the upper layer to the lower layer,” he said. “When that Velcro is missing, the layers slide against each other and cause blisters.”
About 20 in every 1 million babies born in the U.S. have EB, which comes in several forms and can range from mild to severe, experts say. That means between 25,000 and 50,000 people in the U.S., mostly children, are living with the condition. Left untreated, EB results in painful disfigurement and early death, typically before the age of 30. Earlier victims of EB often developed deadly skin cancer spurred by the rapid cell turnover the condition causes.
Babies like Elisa, those born with severe EB, develop lesions everywhere: on their hands and toes, on their bottoms, in their mouths and throats. They’re often called “butterfly children” because their skin is so fragile — as fragile as butterfly wings, some say.
But when Elisa was born, McCann wasn’t interested in sentimental labels. Like many modern parents facing rare diseases in their children, she turned to experts and the Internet to demand answers.
“I said I want to know the No. 1 doctor in the world who can do something about this,” she said. Over and over, Tolar’s name came up.
“I got in contact with him and we were in contact every day,” she said. “Right away, he got very protective of Elisa.”
McCann and her husband, Dagan McCann, a travel writer, moved to Minneapolis to be close to Tolar and his treatment, she said.
Transplanting bone marrow from Stella to Elisa populated her blood with healthy cells. First, though, scientists had to give Elisa chemotherapy and radiation to make room for the new cells to “set up shop,” Tolar said. An extra boost of full-body irradiation appeared to allow the cells to engraft, or take hold, even better.
At the last measure, more than half of the donor cells from Stella had partially engrafted, a high percentage, Tolar said. In previous protocols, about a third of the children who received bone marrow transplants had some improvement, but not the dramatic results Elisa has shown. In many of the children, however, Tolar has been able to show that cells from the donated bone marrow actually gravitate to the skin, healing the injuries.
For Elisa, the real-life results have been impressive, Gabriella McCann said.
“Before the transplant, I was walking everywhere with a needle or scalpel to open the blisters and drain them,” she said. “They would get humongous in a few minutes.”
Now, Elisa still gets blisters, but they’re smaller and they heal by themselves. She’s still fed through a tube because of the blisters that scarred her throat, but that’s getting better. And just this week, she got to go out to lunch for the first time because she’s healthy enough to be just another baby out with her mom in public.
“My daughter didn’t have a life before,” McCann said. “Now my daughter has a life and they’re pretty sure she won’t blister as much as before.”
Funding for work by Tolar’s team and other leading EB experts who are investigating stem cell therapy and gene transfer therapy at Stanford University is a huge concern. EB is classified as a rare disease, and paying for the research can be a challenge. But the scientists are boosted by organizations such as the EB Medical Research Foundation, headed by Andrea Pett-Joseph and her husband, Paul Joseph. Another prominent foundation is DEBRA of America, the Dystrophic Epidermolysis Bullosa Research Association.
The Josephs' son, Brandon, was born 10 years ago with EB, galvanizing his parents into taking over the all-volunteer nonprofit that has raised $5 million for EB since 1991. They’ve attracted a star-studded honorary board of directors that includes actors Courteney Cox, Jennifer Aniston, Brad Pitt and Adam Sandler, plus other sports and political luminaries.
But with successes like Tolar’s bone marrow transplant and a natural gene therapy program and new research into gene transfer therapy at Stanford, the Josephs say the investment is paying off.
“A lot of families are feeling more hopeful that this is happening,” said Andrea Pett-Joseph. “It’s happening at a good pace and people can see the evidence of it. Sometimes, science is so far away.”
When Doctors Without Borders nurse Monia Sayah first arrived in Guinea in March, she couldn't have known she would witness the worst Ebola outbreak in history. Back then, there were 59 confirmed deaths from Ebola, a virus which can be fatal in up to 90 percent of cases. The death toll in West Africa has since soared to 932, the World Health Organization said Wednesday. In Guinea, where the first cases were reported in March, Ebola has killed 363 people.
"The fear is palpable," Sayah said, speaking to CBS News in New York after returning from her latest assignment. "People are very afraid because they never know if Ebola's going to hit their family or their village."
Because of the fear and stigma associated with the virus, Sayah said many infected people are choosing to hide their illness and often don't check in to treatment centers until it is too late. By that point, there is very little Sayah and her colleagues can do. They try to rehydrate the patients and administer antibiotics. But there is no proven treatment for Ebola, though an experimental drug is currently being tested.
Concerns have also been growing for the safety of medical workers in the field. A leading doctor died in Sierra Leone last week. A Nigerian nurse who treated that country's first Ebola victim died from the virus, Nigerian health officials said Wednesday, and two American medical missionaries infected with Ebola in Liberia are still battling the virus at Emory University Hospital in Atlanta.
But Sayah, who has spent a total of 11 weeks in Guinea, said she is not afraid. She and her colleagues take strict precautions to limit their risk of exposure. Before entering a high-risk zone, they suit up in head-to-toe protective clothing including gloves and goggles. "You do have to follow the rules," she said, "but accidents do happen."
She has to limit the amount of time she spends in the infected area. It's hot under the protective clothing, and exhaustion and dehydration are serious concerns. "The risk is you could faint, you could fall. You do not want to fall in a high-risk area," she said. "Maybe your goggles will move up and your eye will be infected."
Working so closely with patients at death's door has taken a personal toll. Sayah described the anguish of stepping outside a treatment facility to take a quick break from the intense heat, only to find that her patient had died in those ten minutes she was away. "It was really hard for me to know that they had died alone," she said, "not with someone holding their hands and reassuring them."
Sayah recalled the "hectic" challenges of setting up some of the first international treatment facilities for Ebola patients. By the end of May, she said, the medical community thought they had almost contained the virus. But soon after she left Guinea, another cluster of infected patients was found in another village. The virus was spreading like wildfire.
Several factors are contributing to the spread. The virus has an incubation period of up to 21 days, according to the WHO, and in West Africa the population is highly mobile, moving easily across porous cross-country borders. Traditional burial ceremonies in which relatives have direct contact with the body can also play a role in the transmission of Ebola.
Sayah found that many local communities distrust the healthcare system and foreigners. "Some have said we brought the Ebola to them," she said. "It's very difficult to contain the outbreak when communities are not cooperating." There were instances of infectious patients leaving the facility, she said, and many weren't receptive to the idea of isolation -- a crucial step in containing the virus.
During her breaks from the field, Sayah stays in touch with her colleagues on the front lines, hoping for the slightest bit of good news. Just this past week, she heard some. One of the patients who'd been under her care was discharged from hospital, apparently free of the virus.
But the situation on the ground remains dire, and Sayah hopes to see a greater response from the international community.
Despite the challenges, Sayah said she will return to West Africa to fight the outbreak. "When you're there and you see how much needs to be done," she said, "there is not a question of 'should I go back or not?'"
When forensic nurse examiners work with survivors of violence – sexual assault, child abuse, elder abuse or domestic assault – they’re painstakingly collecting and documenting evidence that can hold up in a potential court case. And they’re taking care of a person who’s just been traumatized, often by someone they know well. Forensic nursing takes a balance of objectivity, skill and compassion, and it’s more than just a job for the professionals who do it.
Experts on the Stand
Whatever type of assault they’ve endured, survivors’ first encounter with law enforcement or medicine “paves the way for their entire future,” says Trisha Sheridan, a forensic nurse and clinical assistant professor at Texas A&M Health Science Center College of Nursing.
Victims face a higher risk of post-traumatic stress disorder, depression, suicide and medical problems in the aftermath, she says, and those who “have a positive experience with someone who’s trained to deal with victims of violence” tend to not only have better legal outcomes, but better quality of life than others who receive standard emergency care. But in Texas, especially the more rural areas, forensic nurse examiners are few and far between.
Last year, Texas passed a law requiring emergency department nurses to undergo two hours of training in basic evidence collection, but that’s far from enough, Sheridan says. And while most facilities “either have a specific room that’s set aside in the ER or special private place for those patients,” she says, “without a forensic program or a forensic nurse, it’s just an ER bed.”
While certified forensic nurse examiners undergo extensive skills training, Sheridan believes graduate programs can move forensic nurses to the next level, with a deeper understanding of the science behind the evidence they’re collecting, helping them explain the pathology and ramification of victims’ injuries in a courtroom. For instance, she says that information helped the jury “make a better-informed” decision when she testified in two recent cases of strangulation.
Taking On Domestic Violence
Strangulation is one of the most frequent injuries in domestic violence, yet symptoms are subtle and often downplayed, says Heidi Marcozzi, coordinator of the Intimate Partner Violence Program, started last year as a branch of District of Columbia Forensic Nurse Examiners, which also works with victims of sexual assault.
Forensic nurses look not only for bruises and scratches, but less obvious symptoms such as petechiae (small red or purple spots on the skin), voice changes, cough and headaches, Marcozzi says. They ask patients about loss of bowel and bladder function, which is a good indicator that they lost consciousness during the attack.
“Domestic violence is a huge issue” in the nation’s capital, Marcozzi says. The program’s 30 forensic nurses respond to these calls from MedStar Washington Hospital Center, anytime day or night. Within an hour of getting the call for a domestic violence case, the forensic nurse arrives at the hospital, where ER staff have already made sure the patient is in a quiet, private space rather than the waiting room.
Before the exam, the forensic nurse walks the patient through the whole process. “We see a fair amount of drug-facilitated sexual assaults, so we want to make sure it’s very clear that the patient is able to consent,” Marcozzi says. “Then we do a medical exam head to toe to make sure they’re physically stable.” Nurses pays close attention while patients describe the incident and use that account to guide where they collect evidence, including swabs that will later go to the crime lab for analysis.
The FNE photographs any injuries and examines the patient using a high-powered light source that can reveal hard-to-see signs like bruising. The light also helps the nurse locate "foreign secretions ... things will fluoresce under certain wavelengths – semen, urine, saliva,” Marcozzi says.
More Than Just a ‘Rape Kit’
Victims of sexual assault go through essentially the same process, with the addition of a pelvic exam, which takes an additional 15 minutes or so. Examiners photograph the genitals for signs of injury, and then collect swabs as indicated. Treatment comes next. If appropriate, patients can receive Plan B emergency contraception to prevent unwanted pregnancy, or medications to protect against HIV and other prevalent sexually transmitted infections.
In sexual assault cases covered by DCFNE, an advocate with Network for Victim Recovery of DC accompanies the nurse to the hospital and helps patients with crisis management, discharge plans, crime victim’s compensation and referrals for counseling.
Preventing the Worst
For domestic violence victims, the DCFNE program teams up with Survivors and Advocates for Empowerment, a nonprofit that provides advocacy and crisis intervention, and works to hold offenders accountable. SAFE runs the lethality assessment project for the District of Columbia – trying to determine which victims are at highest risk for being killed by their abusers.
Advocates evaluate the victim’s environment for cues – such as whether the abuser has easy access to weapons, or even “if there’s a child in the home who doesn’t belong to him, which, believe it or not, increases the severity of the risk,” says Natalia Marlow-Otero, SAFE director.
Of the 5,000 or so domestic violence cases SAFE sees each year, up to 1,900 are deemed high-lethality cases. Isolation is a “huge” factor among the women – and some men – who are victims of domestic violence. Isolation and abuse are even more prevalent among immigrant clients, Marlow-Otero says, so SAFE provides an English/Spanish helpline (1-866-962-5048). People can also call the National Domestic Violence Hotline at 1-800-799-7233 (1-800-799-SAFE).
Pharmacy errors, hard-to-find clinical alerts, “farcical” training, and potentially life-threatening design flaws: Reading through the U.S. Food and Drug Administration’s catalog of electronic medical records malfunctions could be hazardous to your mental health.
If not yours, than that of the physicians and nurses who must work with the records systems, and who are reporting their experiences to the FDA’s adverse event database, otherwise known as MAUDE (the Manufacturer and User Facility Device Experience).
Most of the events submitted to the database involve misfiring medical equipment — broken aerosol compressors, faulty defibrillators — but as electronic records and computerized physician-order entry systems take hold at hospitals and clinics across the country, complaints about those systems are on the rise.
For decades, electronic patient records systems have been heralded as a potential game-changer for the health care industry, leading to improved patient health outcomes, fewer duplicate tests and, eventually, savings for the health care industry.
While most clinicians and academics still believe the promise is there, the systems are coming under increased scrutiny from doctors, nurses and some on Capitol Hill who say the technology is poorly regulated, often unproven and occasionally unreliable.
As such, the health records systems haven’t yet lived up the promise that was made when the Obama administration won passage its 2009 stimulus bill, which included $25.8 billion for health IT investments and incentive payments.
“Like with any new technology, there’s going to be unintended consequences,” said William M. Marella, director of Patient Safety Reporting Programs for the suburban Philadelphia Emergency Care Research Institute. He’s also director of the state’s Patient Safety Reporting System, which tracks adverse events and near-misses in Pennsylvania.
“In the long run, [electronic health records] will make us safer than we were” using paper records, Mr. Marella said. “But in the short term, we’ve got a lot of [implementation] issues that need to be addressed before [electronic health records] meet their promise.”
Last month, the nation’s largest union of registered nurses sent a letter to the FDA asking for broader and more stringent oversight of electronic records systems and of computerized physician-order entry systems, which allow clinicians to log treatment instructions for patients.
The National Nurses United, as part of its broader campaign highlighting the potential dangers of “unproven medical technology,” says FDA officials should test electronic medical records as rigorously as they might a new drug or an artificial hip implant.
“I don’t think that opinion is an outlier opinion,” Mr. Marella said. “Lots of clinicians are unhappy with the way these systems work, and are unhappy with the documentation burden we put on them.”
The nurses union also wants the U.S. Centers for Medicare and Medicaid Services to suspend its “meaningful use” program, which requires providers to start installing electronic medical records systems at the risk losing Medicare funding, “unless and until we have unbiased, robust research showing that [electronic health records] can and do, in fact, improve patient health and save lives.”
To date, since 2011, that CMS program has issued nearly $24 billion to hospitals and physicians clinics seeking to upgrade their electronic records systems and make the transition away from paper records.
Tracking the errors
The letter submitted by the nurses union to the FDA was part of the commentary related to the federal government’s proposed overhaul of its framework for regulating health IT. That draft proposal was published in April, a joint effort of the FDA, the U.S. Department of Health and Human Services, the Federal Communications Commission and the Office of the National Coordinator for Health IT.
Others offered their own responses. The College of Healthcare Information Management Executives and the Association of Medical Directors of Information Systems, in joint comments to the FDA, said that the government needs a retooled electronic health records certification program in order to “identify clear standards and require strict adherence to those standards.”
The report itself noted that “a nationwide health information technology infrastructure can offer tremendous benefits to the American public, including the prevention of medical errors, improved efficiency and health care quality, [and] reduced costs. … However, if health IT is not designed, developed, implemented, maintained, or used properly, it can pose risks to patients.”
Patient risk was a concern when, last summer, UnitedHealth Group Inc. recalled software that was used in hospital emergency rooms in more than 20 states “because of an error that caused doctor’s notes about patient prescriptions to drop out of their files,” according to Bloomberg News. There were no reports of patient harm, a UnitedHealth spokesman said, but the glitch illustrates the potential pitfalls for digital health records.
The MAUDE system, which accepts voluntary and anonymous incident reports from practitioners, and Mr. Marella’s own reporting have turned up plenty of other glitches. Some involve human error, others involve software and interoperability malfunctions, and many are simply design flaws, such as this example from a 2012 Pennsylvania Patient Safety Authority report:
Patient with documented allergy to penicillin received ampicillin and went into shock, possibly due to anaphylaxis. Allergy written on some order sheets [but] never linked to pharmacy drug dictionary.
And this one, from MAUDE:
Potassium chloride was prescribed twice per day as treatment for hypokalemia. The lab testing revealed a [bad] jump in the potassium level, but the result came to the EHR without alert or warning, and the nurses continued to give the patient potassium anyway [because] the nurse did not know that the potassium level was high. ... Though this patient did not die, others have from this type of defect.
Or this one, from 2013:
Patient’s medication list and other active orders did not appear on the doctor’s order section on the CPOE system, rendering it impossible for the doctor to confirm, alter, and reconcile the medication list. ... For obvious reasons, this defect in the CPOE is potentially life threatening when the doctor(s) do not have access to the current medication list.
And from April:
A patient [was] at risk for respiratory arrest due to a narrowing in the trachea. There is no place on the EHR to list such a life-threatening condition that would be visible to each and every care team member who opened the EHR for this patient. ... Care was delayed due to the above mentioned reasons, [and] the patient sustained a complete respiratory arrest that led to a cardiac arrest and anoxic brain injury.
Human factors
While examples of electronic health records problems can be retrieved via various state and federal databases, many in the medical field say tracking the issues in a more comprehensive way will lead to better systems. Mandatory reporting would help, too, since only a fraction of adverse events related to electronic health records are actually reported to the FDA or state authorities.
But health IT vendors are against mandatory reporting, or any other system that would run afoul of the confidentiality clauses that are built into contracts with hospitals and clinics. Public, mandatory confessions of errors might also discourage such reporting, since the clinician who admits the error could be punished by his or her employer.
“We have felt that reporting by both providers and vendors should be voluntary. That is most consistent with the notion of a learning environment,” said Mark Segal, the chairman of the Electronic Health Records Association, told The Boston Globe.
Clinicians, too, are also wary about striking the right balance. “FDA oversight and regulation could slow innovation,” particularly if electronic health records and related systems are indeed scrutinized like other medical devices, according to a letter to the FDA from American Medical Association CEO James Madara.
And they have the FDA on their side. The agency does not intend to require the reporting of electronic health records-related adverse events, and does not intend to vet electronic health records in the same way that it reviews drugs and other medical devices.
But when push comes to shove, though, regulators should err on the side of safety, said Dean Kross, a cardiologist in private practice at the Allegheny Health Network and a longtime critic of electronic health record companies and the side effects of health IT adoption.
“The vendors have not been held accountable for the devices they are manufacturing,” he said. There is negligible pre-installation vetting, or post-market surveillance, for “safety, usability and efficacy,” he said.
And regulators should keep a watchful eye on human usability.
“Ninety percent of [complaints] have got something to do with faulty user-device interaction,” said Robert A. North, chief scientist at Human Centered Strategies, a Colorado company that studies and seeks to reduce risk and error in medical device design. “It’s not that something that is breaking or freezing. ... it’s nothing to do with the electronic circuit board. It’s the human circuit board.”
While Mr. Marella is aware of the design shortcomings of electronic health records, he’s still a believer that the systems can, and are, improving patient and population health.
He points to the example of a Pennsylvania hospital that noticed some its patients were overdosing on narcotic painkillers while in the hospital, and had to be given reversal agents to mitigate the overdose symptoms. When clinicians dug into the electronic records, they saw that the overdoses were happening primarily among people being given painkillers for the first time.
“So they decided that the default dose was actually too high” for first-time opioid recipients, and adjusted the first-time dosage going forward, Mr. Marella said. Identifying a hospital-wide problem, and addressing it quickly, probably couldn’t have happened without electronic health records.
“We really have to do a lot more work in what we call human factors,” so that the systems are intuitive, he said. “We’re quite a long ways from there.”
The National Association of Hispanic Nurses (NAHN) has received a five-year, $1.24 million Science Education Partnership Award (SEPA) grant from the National Institutes of Health to support NAHN’s collaborative project with the Hispanic Communications Network (HCN) entitled Hispanic Role Models in Health Careers.
This collaborative NIH R25 program has been established to address the need for cultural and linguistic diversity among health professionals by recruiting and interviewing bilingual role models and arranging to broadcast those interviews. Through these efforts, the project aims to inform Spanish-speakers about the range of health careers open to them through proper education, and to inspire them to imagine themselves in careers focusing on health and medicine.
Leveraging HCN’s nationally-broadcast health education radio shows, whose cumulative audiences are larger than NPR’s “All Things Considered,” as well as the social media outreach of both organizations, this project has the potential to reach one-third of the nation’s Hispanic population during its first five years.
“In the United States, registered nurses represent 3 million members, the largest segment of the U.S. health care workforce.Yet, Hispanics still comprise only 3.6 percent of all nurses. I am excited that NIH has provided NAHN the opportunity to be able to reach out to our Hispanic youth with hopes to inspire them into becoming a professional nurse,” said Angie Millan, Principal Investigator of the Hispanic Role Models In Health Careers.
“This new SEPA project, Hispanic Role Models in Health Care Careers, is aligned with NAHN’s commitment to support professional career opportunities for Hispanic nurses and their effort to improve health in Hispanic communities. The project also supports the SEPA’s goals of providing opportunities for students from underserved communities to pursue careers in biomedical fields and to improve community health literacy,” said Dr. Tony Beck, director of the NIH Office of Science Education/SEPA.
In addition to national media outreach, a number of bilingual online resources for health career aspirants will be established, including an extensive database of volunteer professionals who have said “¡Sí!¡Seré Mentor!” (“Yes! I will mentor you!”). These resources will provide Hispanics of all ages and walks of life with the opportunity to form relationships with seasoned healthcare professionals.
Additional outreach to be established alongside the project include: public speaking and media relations training opportunities provided for attendees of NAHN’s annual conference; an Advisory Committee of health organizations, professionals and advocates established to recommend role models and provide periodic feedback; and bilingual independent evaluators associated with the UC Berkeley School of Public Health instituted to conduct rigorous evaluation throughout the project.
To learn more about the Hispanic Role Models in Health Careers program, please visit www.nihsepa.org
Google mapped the world's streets and developed self-driving cars to roam them. Now, the company wants to map something much larger: perfect human health.
Google Baseline, announced last week, will collect molecular and genetic information from an initial 175 volunteers and later thousands more. The philosophy is to focus on the genetics of health itself, rather than focus on disease.
Health research experts agree that Google brings a fresh perspective and technological expertise to the complex world of genetics. But they aren't sold on all facets of Google's approach.
"We want to understand what it means to be healthy, down to the molecular and cellular level," Google said in a press release. Google repeated the phrase "what it means to be healthy" a few times -- and that's what worries one expert.
"My immediate question is, what does Google mean by that? Healthy for a six-year-old boy, or a 75-year-old woman? You're injecting values about the range of humanity, right off the bat," said Arthur Caplan, the director of the division of medical ethics at the NYU Langone Medical Center and an NBC News contributor.
Google isn't purporting to develop a model of the singular perfect human. The goal is to analyze participants' data from to uncover "biomarkers," or patterns, that can be used to detect disease earlier.
"It's a perfectly reasonable approach, but I wouldn't do it under the 'what it means to be healthy' mission statement," Caplan said. "Those are fighting words. The mother of a child with Down's syndrome may consider her child perfectly healthy."
What's more, genetics alone doesn't provide a full picture of health or of disease, pointed out Kedar Mate, M.D., the vice president of the Institute for Healthcare Improvement, a Massachusetts-based not-for-profit.
"Genes are about 15 to 40 percent, behavioral patterns 30 to 40, socioeconomic factors 20 to 30, etc.," Mate told NBC News. "So even a wonderful genetic model is not a total picture of health."
What makes Baseline different, Google argues, is that it will "try to connect traditional clinical observations of health" like diet and other habits with genetic information.
But while Google (nor anyone) can't create the full model of perfect health, the company still brings two major advantages to the field: technological power and an outsider perspective.
"Anyone can collect 175 DNA samples," Caplan said. "But Google is a very, very powerful computational company. That's what makes it exciting."
Google's trove of technology resources and know-how could create a faster, smarter process for analyzing the links between genes and disease.
But not everyone in the field considers Google's computational power a major boost. Some genomics experts scoffed online at Google's assertion that Baseline is a "clinical research study that has never been done before."
"Frankly, anything Google does gets attention," Mate said.
"What would make it really different is Google's knowledge of so much of our behavior," he added. "If Google could take all of that and combine it with genetic information -- no other organization can offer us that."
But given what little we know about Baseline, it doesn't sound like Google is planning to do that -- at least not now. It's not clear they could, even if they wanted to.
Google declined to comment to NBC News on that point, or on the Baseline project overall. But the company told the Wall Street Journal, that use of data will be limited to medical and health purposes -- and won't be shared with insurance companies, for example.
Whether Google would -- or even could -- move to combine health data with the rest of the information it knows about our behavior, Mate insisted the nature of Google's business adds a unique element to the pursuit of health.
"You wonder if they’ll bring a fresh and different perspective, because this isn’t a stodgy academic project," Mate said. "The entry of a player like Google has the ability to stimulate the space -- and break it out of the way things have always been done."
For all the impressive advancements in medical technology, researchers and scientists still face a daunting challenge when they study the habits of the adorable but uncommunicative subjects called human infants.
In order to study infants without overwhelming them, scientists often try to mask the massive machines needed to view brain activity either by having the child sleep through it or by covering it in kid-friendly decorations. Other researchers have devised decidedly low-tech ways of reading an infant’s interest in a subject, even when they can’t say a single word.
In a study released Monday in the Proceedings of National Academy of Sciences, doctors used a special machine to examine infant brain activity as they start to learn language skills.
Patricia Kuhl, a professor of speech and hearing sciences at University of Washington and the lead author of the study, said the research indicated the area of the infants’ brain that controlled motor skills lit up when they heard certain words. The activity indicated that the infants are trying to mimic adults and speak much earlier before they say their first word.
However, Kuhl said, the study was important because of both the surprising findings and the way researchers were able to get them. To “read” the infant’s brain activity, they used the cutting-edge device called a magnetoencephalograph, that was quiet and nimble enough to read the chaotic world of infants’ brain activity.
Kuhl said unlike an MRI machine, which is extremely loud and requires a patient to be totally still, the magnetoencephalograph is nearly silent. However the infants still had to be strapped into a chair, so to keep them entertained the researchers were tasked with making silly faces and holding up toys all in the name of science.
“You want them to like the lab,” said Kuhl. “It’s decorated with fish and it’s got little stickies [on it.] It’s ... very baby friendly. We wave toys and we’re very aware and of their curiosity and of their desire to play. We do everything to make them comfortable.”
In a 2013 study published in Psychological Science, researchers used MRI machines to examine baby’s brain activity in response to different stimuli. However, to get the infants into a machine where they could not move, the researchers had the babies go in after they fell asleep naturally. They also used ear coverings so the loud MRI machine didn’t wake the infants.
MRI machines can be so distressing for patients because of claustrophobia or other fears about being in the hospital that a New York Hospital installed a pirate-themed scanner to put children (and some parents) more at ease.
“The genius is in this machine. ... There’s no noise and the baby can listen and can move,” said Kuhl of the magnetoencephalograph. “The ability for the first time to do this kind of recording in this kind of technical advanced machine ... [it’s like] we’re putting [on] a stethoscope.”
Aside from technological advancements, researchers rely on some decidedly low-tech approaches when studying infants.
Fei Xue, a professor of psychology at the University of California Berkeley, has done numerous studies examining how infants learn and react to new toys or information. She said researchers have plenty of tricks to keep babies focused on the tasks at hand.
Xue said most studies only last between 5-10 minutes because the infants will get bored if they're longer. If they want a baby to focus on an object, they darken the room and light up the object to draw the baby's attention.
“In a way, it’s easy to work with infants,” said Xue. “They’re very curious and they’re interested in the world.”
To measure if babies are interested in an object or scene without getting verbal confirmation, Xue and her fellow researchers simply follow the infant’s eye movement. While there are special computer programs, Xue said often it just comes down to a researcher holding a stopwatch and watching the infant through a monitor.
In spite of the infants’ inability to speak, Xue said, understanding their thought process can reveal how they learn, which could eventually help shape education programs.
“When they go to preschool and elementary school ... they will help us to know how to structure the school system,” said Xue of her young subjects. “Understanding these really young humans is important.”
In a forthcoming Cornell study published in the journal Health Environments Research and Design, Rana Zadeh, assistant professor of design and environmental analysis, discovered nurses who had access to natural light enjoyed significantly lower blood pressure, communicated more often with their colleagues, laughed more and served their patients in better moods than nurses who settled for large doses of artificial light.
Letting natural light into the nurses’ workstations offered improved alertness and mood restoration effects. “The increase in positive sociability, as measured by the occurrence of frequent laughter, was … significant,” noted Zadeh in the paper.
Nurses work long shifts, during non-standardized hours. They work on demanding and sensitive tasks and their alertness is connected to both staff and patient safety. Past evidence indicates natural light and views have restorative effects on people both physiologically and psychologically. Maximizing access to natural daylight and providing quality lighting design in nursing areas may be an opportunity to improve safety though environmental design and enable staff to manage sleepiness, work in a better mood and stay alert, according to Zadeh.
“Nurses save lives and deal with complications every day. It can be a very intense and stressful work environment, which is why humor and a good mood are integral to the nursing profession,” Zadeh said. “As a nurse, it’s an art to keep your smile – which helps ensure an excellent connection to patients. A smart and affordable way to bring positive mood – and laughter – into the workplace, is designing the right workspace for it.”
Access to natural daylight, and a nice view to outside, should be provided for clinical workspace design, said Zadeh. In situations where natural light is not possible, she suggests optimizing electric lighting in terms of spectrum, intensity and variability to support circadian rhythms and work performance.
“The physical environment in which the caregivers work on critical tasks should be designed to support a high-performing and healthy clinical staff,” she said “ improving the physiological and psychological wellbeing of healthcare staff, by designing the right workspace, can directly benefit the organization’s outcomes”.
In addition to Zadeh, this study, “The Impact of Windows and Daylight on Acute-Care Nurses’ Physiological, Psychological, and Behavioral Health,” was authored by Mardelle Shepley, Texas A&M University; Cornell doctoral candidate Susan Sung Eun Chung; and Gary Williams, MSN, RN. The research was supported by the Center for Health Design Research Coalition’s New Investigator Award.
Cancer is plaguing a growing number of first responders and rescuers who worked at ground zero after the terrorist attack on the World Trade Center on September 11, 2001. These are cancers the federal government says are thought to be directly related to that effort -- cancers like leukemia, myeloma, thyroid and prostate cancers.
There are at least 1,646 certified cancer cases that have been documented by Mount Sinai Selikoff Centers for Occupational Health. There are some additional 863 cancer cases among both fire and EMS personnel, according to FDNY, which keeps a separate database for its members.
That's a total of 2,509 cases. The center has screened more than 37,000 World Trade Center rescue and recovery workers since 2002. It will continue to monitor those workers and volunteers for any new cases.
Some reports suggest the number of cancer cases in this group has doubled since last year. While that may be mathematically true, cancer experts caution that we can't draw any significant conclusions from the increase.
"For every decade of life, if you look at a population ... cancer rates go up the older you are," said Dr. Otis Brawley, the chief medical and scientific officer and executive vice president of the American Cancer Society. "Looking at an increase from one year to the next is a nonscientific way of making an assessment that is incredibly biased to find a link between the activity and the cancer."
To be scientifically accurate, Brawley said someone would have to look at all the cancer records for the people in the 9/11 group and compare them to a group that had the same age makeup, same gender, and other demographic data. There would also have to be a significant portion of firefighters in that sample, because as a profession they tend to have higher cancer rates than the general population, Brawley said.
A deep scientific analysis of available medical data through 2010 showed a 20% increase in the rate of cancer cases for 9/11 rescue and recovery workers when compared to the general population, according to Mount Sinai.
Government reports suggest workers at the World Trade Center were exposed to a number of chemicals that were known to be carcinogens, or agents that may cause cancer.
Many people who worked at the site are struggling with devastating cancers they may not otherwise have had, had they not responded to the tragedy. That much is clear, according to the U.S. government, which set up a special World Trade Center Health Program.
The program provides medical monitoring and treatment services for 9/11 responders and survivors. Nearly 65,000 people are enrolled. Enrollees are qualified to get health care treatment through several reputable medical centers that keep experts on staff who are qualified to treat and identify illnesses related to the terrorist attacks. The program plans to continue to monitor those workers.
"I think all of us are open to the possibility that these brave folks were exposed to things that caused further illness," Brawley said. "What's most important is that someone has cancer and needs help and we should continue to provide them with the good care they truly deserve."
When you're sick, sometimes it feels impossible to get out of bed, let alone get to the doctor. And the last thing anyone wants to do is spend hours at the emergency room.
So Silicon Valley is retooling a service that was common almost a century ago: the house call. Several companies have developed smartphone apps that bring doctors to patients, often in less time than it would take to seek treatment elsewhere. With apps like Pager and Medicast, a patient can request a doctor with the push of a button.
In the 1930s, physician house calls accounted for 40% of medical visits, according to a 2011 article in the journal American Academy of Family Physicians. By the 1980s, that number had dropped to 1%, due in part to a lack of funding by insurance carriers.
Elizabeth Krusic, a mother of two young children from Seal Beach, California, knows how difficult it can be to take a sick child to see a doctor. When her daughter developed an eye infection, she took a friend's advice and tried Medicast, calling a doctor into her home and saving the stress of getting her small children ready and out of the house.
The doctor arrived in 30 minutes and had the necessary prescription medication on hand.
"My son was able to sleep during the entire visit, because the doctor came to the house," Krusic said. "The doctor came into my daughter's room and conducted the visit there, where she was comfortable."
The house call also removed the risk that her children would be exposed to illnesses in a waiting room.
Inspired by Uber
In early 2014, Uber co-founder Oscar Salazar saw room for improvement in the health care system and seized the opportunity.
The app he developed, Pager, offers house call services for customers in Manhattan and, starting next week, Brooklyn. Pager's doctors are available from 8 a.m. to 10 p.m., 365 days a year, with an additional after-hour fee for nights and weekends.
Toby Hervey, Pager's head of marketing and business development, said that several aspects of Uber informed Pager's approach. Like Uber, the app is structured as a mobile, location-based service.
"Convenient access to quality health care when you need it is a real problem," he said. "We're using technology to make the house call -- one of the best ways to get personal care -- viable again."
Hervey said customers range from parents not wanting to take a sick child to an emergency room to businesspeople with no time to see a doctor during the day.
A similar company, Medicast, started in South Florida in late 2013, with services now also available in San Diego, Orange County and Los Angeles.
"Long wait times are frustrating for everyone," Sam Zebarjadi, co-founder and CEO of Medicast, said. "With the proliferation of technology and increasing levels of education, we knew there were alternate ways to get amazing health care."
Dr. Kimberly Henderson is a Pager physician and works in the emergency room at New York's Beth Israel Medical Center. For her, the idea of being a part of a new practice of medicine was appealing.
"I believe we will see a shift away from medical practice exclusively in the brick and mortar model," Henderson said. "Medicine will become, or return to being, more mobile."
As the doctor shortage grows and patients struggle to balance their busy lives, telemedicine has become a fast-growing field. Health care professionals offer their services using two-way video, e-mail, smartphones and other forms of technology. Apps, such as Doctor on Demand and Ringadoc, allow patients to speak to a physician via phone or video chat.
Doctors enrolled with the service PINGMD can receive text, photo or video messages from their patients that can be forwarded to colleagues for referrals and are automatically saved to the patient's medical file. Another app, HealthTap, connects patients to 50,000 doctors across the country for verified answers to medical questions. Patients can search the database or ask their own questions and receive responses from multiple doctors, providing them with several opinions.
The American Medical Association says that telemedicine, including house call services, is useful for both patients and the health care industry as a whole, according to its June Report on the Council of Medical Service.
"Telemedicine, a key innovation in support of health care delivery reform, is being used in initiatives to improve access to care, care coordination and quality, as well as reduce the rate of growth in health care spending."
How house call apps work
After a brief video conference, a doctor will assess the patient's need for a home visit. If no visit is necessary or the physician recommends a trip to the emergency room, there's no charge.
"With this system, we're able to provide high quality care that goes beyond the issue at hand," Zebarjadi said. "With the doctor visiting patients in their own homes, it's easy to make observations and discuss other health concerns and lifestyle choices."
"I love the concept of bringing our services to people's homes," said Medicast's Dr. Elisa Malin. "It's a convenience factor, both for the patients and for us as physicians, in the sense that I can choose to be on call whenever I'm available."
Malin also works as a pediatric hospitalist for Kaiser Permanente. She said that a typical house call visit lasts about 45 minutes, as opposed to the average 10-minute visit at a clinic.
"The fact that I get the luxury of time with Medicast patients improves the quality of care they receive."
With both apps, physicians follow up with the patient via phone and are available to answer any questions that may have come up since the visit.
Although the apps are only currently available for iPhone, Pager and Medicast are actively working on an Android app. For non-iPhone users, their services are also available by phone and on their websites. They also have plans to move into other markets in the near future.
The house calls are comparable to an urgent care visit, and cost much less than the emergency room, where many people still go to seek treatment for minor ailments. Both companies offer flat rates, starting at $199 for a house call. Customers can also sign up for a monthly plan that allows them two or four visits a year.
The companies aren't able to accept insurance, but are in talks with various providers to make that option available in the future.
House calls have their advantages, such as privacy and convenience, according to Dr. Jane Orient, executive director of the Association of American Physicians and Surgeons. They also can save on office overhead for physicians. But they do have limitations, she said.
"The doctor's black bag won't have all the equipment available in the office," she said.
Both companies' websites have long lists of conditions they treat, such as cold and flu, sprains, eye infections, pneumonia, abdominal pain and cuts that require stitches. But there are also conditions their doctors cannot handle. You should call 911 or go to the emergency room if you are experiencing chest pain, shortness of breath, or have had a head injury and lost consciousness.
This questionnaire will be used to address nurse job satisfaction as it relates to low nurse to patient staffing ratios. By completing the questionnaire, you are providing Informed Consent for use of the data collected. Anonymity will be maintained. Please read the questions carefully and answer to the best of your knowledge.
Nearly one-third of U.S. children and adolescents are obese or overweight, but many don't realize that they fall into that category.
According to new government statistics, approximately 30% of children and adolescents ages 8-15 years (32% of boys and 28% of girls) — an estimated 9.1 million young people — don't have an accurate read on their own weight.
About 33% of kids (ages 8–11) and 27% of teens (ages 12–15) misperceive their weight status, says the report from the National Center for Health Statistics.
Based on data collected between 2005 and 2012 from more than 6,100 kids and teens for the National Health and Nutrition Examination Survey (NHANES), the report also finds:
• 42% of those classified as obese (48% of boys; 36% of girls) considered themselves to be about the right weight.
• 76% of those classified as overweight (81% of boys; 71% of girls) believed they were about the right weight.
• 13% of those classified as being at a healthy weight considered themselves too thin (9%) or too fat (4%).
Studies have shown that recognizing obesity can be an important step in reversing what is a major health problem for U.S. children and adolescents, and it can be an important predictor of later weight-control behaviors, says Neda Sarafrazi, a nutritional epidemiologist at NCHS and lead author of the report.
"When overweight kids underestimate their weight, they are less likely to take steps to reduce their weight or do additional things to control their weight, like adopt healthier eating habits or exercise regularly," Sarafrazi says.
"On the other hand, when normal weight or underweight kids overestimate their weight, they might have unhealthy weight-control behaviors," she says.
Weight misperception varied by race and Hispanic origin, according to the report. Black and Mexican-American youths were more likely to misperceive their weight than white children. It also varied by income level and was significantly less common among higher-income families compared with lower-income families.
The report's findings are not a surprise, says Timothy Nelson, an assistant professor of psychology at the University of Nebraska-Lincoln. He was not involved in the study.
"In general, children and adolescents have a tendency to underestimate their health risks, and this certainly appears to be the case with obesity," says Nelson, who studies pediatric health behaviors. "We see a similar pattern of misperception when parents are asked about their children's weight. Parents are often unaware of the problem."
With obesity so prevalent today, it's understandable that many kids might have a skewed take on their weight, he says. "If they are surrounded by people who are overweight, they may be less likely to label their own weight as a problem."
The findings highlight the need for health professionals "to communicate with families about the child's weight," Nelson says. "This can be a tough conversation when the child is overweight, but it is critical that pediatricians help parents understand where their child stands and what steps need to be taken to get the child on a healthier track."
Odds are small, but family, doctors should keep possibility in mind, researchers say.
Babies born prematurely appear to have a slightly increased risk of potentially fatal blood clots that they will carry into adulthood, Swedish researchers report.
Doctors have previously suspected that babies born earlier than 37 weeks' gestation have a raised risk of deep vein thrombosis and pulmonary embolism, two serious conditions caused by blood clotting in the veins, the researchers noted in background information.
This new study confirms that link, and takes it even further. Premature birth appears to be linked to an increased chance of blood clots in the veins in childhood and early adulthood, according to findings published online July 28 in the journal Pediatrics.
The researchers also reported that a baby's chances of blood clot-related illnesses are directly related to the degree of prematurity. "The more premature, the higher the risk," said Dr. Edward McCabe, chief medical officer of the March of Dimes. A full-term pregnancy lasts from 39 to 40 weeks.
While parents and doctors should keep this risk in mind, they should also be aware that the risk is not huge, said Dr. Kristi Watterberg, chair of the American Academy of Pediatrics' committee on the fetus and newborn. Watterberg and McCabe were not involved with the study.
The association between premature birth and clot risk seen in the study does not prove a cause-and-effect relationship.
The study involved 3.5 million babies born in Sweden between 1973 and 2008, including almost 207,000 born preterm. Out of all the births, only about 7,500 children -- 0.2 percent -- suffered either deep vein thrombosis or pulmonary embolism later in life.
"I think it's important scientifically to know, but it's such a low incidence phenomenon that there are a lot of things to think about before that," said Watterberg, a professor of pediatrics and neonatology at the University of New Mexico School of Medicine.
Deep vein thrombosis involves blood clots that form in a vein deep in the body. If these clots aren't treated and dissolved, they can break off and travel through the bloodstream to the lungs, causing a blockage called a pulmonary embolism. Such a blockage can be deadly.
For the study, Dr. Bengt Zoller, of the Center for Primary Health Care Research at Lund University in Malmo, Sweden, and colleagues used records from the Swedish Birth Registry to track the babies' health. The researchers found that premature babies had an increased risk of blood clots in their veins in infancy, but also from ages 1 to 5 and from 18 to 38.
Very preterm births -- before 34 weeks of gestation -- also had a risk of blood clot-related illness in adolescence, from age 13 to 17.
Boys had an increased risk of blood clots in infancy, while girls were more likely to carry the risk into adolescence and adulthood, the study authors reported.
No one knows why this increased risk exists, but it could be due to genetic factors that caused the mother to deliver prematurely in the first place, Watterberg and McCabe said.
Diseases such as diabetes, thyroid problems and obesity are genetic in nature and can cause preterm delivery, McCabe said.
Also, some mothers who suffer a genetic deficiency in a key protein that controls blood clotting may be predisposed to give birth prematurely, Watterberg said.
"It may be that maternal genetics are a setup for preterm delivery, and those problems are passed along to the infant," she said.
The mother's wellness and lifestyle also play a role in a baby's lifelong health, and could influence their risk of blood clots, McCabe said.
Finally, this link might arise because the babies are born prematurely, and are robbed of maternal hormones and nutrition in the womb that could have decreased their future risk of blood clots.
"We are not as good at getting nutrition into those babies as the mother and placenta are, and we do know that hormones have something to do with the predisposition to clotting," Watterberg said. "It makes sense to me you'd have changes in those long-term outcomes as well."
In any case, it is something for the family and doctor of a person born prematurely to keep in mind, McCabe said.
"If a patient has a history of preterm birth, and the more preterm, the more attention it needs to have," he said. "It helps us be better prepared. If a patient comes in with unusual findings, this provides us some clue."
Wyatt Scott turned a year old earlier this summer, but he ate his birthday dinner through a tube in his tummy.
It’s been more than four months since the Scott family launched WhatsWrongWithWyatt.com to find out why their baby boy can’t open his mouth, and though they’ve been flooded with emails, their little boy’s condition remains a mystery.
Wyatt’s lockjaw has baffled doctors since he was born in June 2013 in Ottawa, Canada, and though the Scott family has taken him to every specialist imaginable, they can’t figure out the root of the problem, Andrew Scott said. Wyatt spent the first three months of his life in the hospital, and his parents have had to call 911 several times because he's been choking and unable to open his mouth.
So Wyatt's mother, Amy, decided to create a website, WhatsWrongWithWyatt.com last spring in the hopes that someone would recognize the condition and offer a solution.
Wyatt's doctor, Dr. J. P. Vaccani, told ABC News in April that the condition, congenital trismus, is rare and usually the result of a fused joint or extra band of tissue. But Wyatt’s CT and MRI scans appear to be normal.
"It's an unusual situation where he can’t open his mouth, and there’s no kind of obvious reason for it,” Vaccani, a pediatric otolaryngologist at Children’s Hospital of Eastern Ontario told ABC News. “Otherwise, he’s a healthy boy."
Andrew Scott said he’s sifted through 500 emails submitted to WhatsWrongWithWyatt.com over the last several months, and compiled a list of the most important ideas to give to Wyatt’s doctors. One letter-writer from Virginia told the Scotts that Wyatt’s story made her cry because her now-14-year-old had similar mysterious symptoms.
“She could have written it herself,” Andrew Scott recalled her saying.
Though the Virginia 14-year-old underwent surgery and therapy, Andrew Scott said Wyatt seems to have something different.
“It’s not just that his mouth doesn’t open,” he said.
Wyatt underwent a study in which doctors X-rayed him while he was feeding to see how the muscles in his mouth and throat worked. They found that he has problems with motor function and swallowing in addition to the lockjaw.
“His blinking is erratic,” Andrew Scott added. “He’ll wink on one side a bunch, then the other side and back and forth.”
Their quest for answers has been slow. A recent muscle biopsy came back negative, and Wyatt is awaiting results of his third genetic test.
Since the website launched, Wyatt had a major health scare: he stole a piece of chicken off his mother’s plate and put it in his mouth, Andrew Scott said. His lips were parted just enough to get it in, but neither of his parents could get it out, so they pulled it out in pieces. They thought it was all gone when Wyatt fell asleep.
Then, Wyatt started choking.
“He almost died,” Andrew Scott said. “I ended up just giving him breath.”
Wyatt “came back” just as ambulances and fire trucks arrived, Andrew Scott said. At the hospital, doctors scoped Wyatt’s lungs, but he was still coughing up chicken pieces several days later.
The emergency forced doctors to use anesthesia to put Wyatt to sleep, which they were too afraid to do before because they feared he would stop breathing. While he was out for the lung scope, the also did a muscle biopsy and put in a G-tube. Now, instead of being fed through a tube in his nose that leads to his stomach, Wyatt can “eat” through a tube in his belly.
Wyatt’s birthday party at the end of June was a pig roast that drew 50 people and included a piñata, goats and a trampoline. Though Wyatt didn’t get any mashed-up pig in his G-tube, Andrew Scott said “maybe next time.” By the end of the party, Wyatt was sound asleep in the grass.
A nice firm handshake has long been a mark of good manners and elevated social skills.
It is also a very germy way to greet your fellow humans, much worse than a couple of more casual alternatives, a new study shows.
"A short, sweet fist bump will transmit the least bacteria," and even a high-five is better than a traditional shake, says David Whitworth, a senior lecturer in biochemistry at Aberystwyth University-Ceredigion in the United Kingdom.
Whitworth and a colleague systematically tested the three greetings for a study published Monday in the American Journal of Infection Control.
For the experiment, one of them repeatedly dipped a gloved hand into a container loaded with a not-too-dangerous strain of E. coli bacteria. The dirty-gloved scientist let the film dry, then shook, fist-bumped or high-fived the other person's clean, gloved hand. Finally, the receiving gloves were tested for bacteria.
Result: The shakes transmitted about 10 times more bacteria than the fist bumps and about two times more than the high fives. The longest, firmest shakes transmitted the most.
In a separate round in which the gloves were dipped in paint rather than bacteria, the researchers found one rather obvious explanation: Bigger areas of the hands touched during the shakes. Handshakes also tended to last longer, but the researchers found more clinging germs even when they compared shakes to fist bumps and high-fives of the same duration.
Since we don't go around dipping our hands in vats of bacteria, the experiment does not perfectly mimic real life – in which different areas of the hand carry different amounts of bacteria, for one thing. It does provide some new ammunition for those who would like to ban handshaking in hospitals and other places where germs are a particular concern.
Whitworth says it also provides an especially good alternative, the fist bump. "You can't really imagine a world where people don't greet each other physically," he says. "It seems to be a basic human need."
Whitworth's findings "are not surprising," says Mary Lou Manning, an associate professor in the school of nursing at Thomas Jefferson University in Philadelphia and president-elect of the Association for Professionals in Infection Control and Epidemiology.
She is not enthusiastic about replacing handshakes with fist bumps in hospitals. The better, more hygienic idea, she says, is to promote rigorous hand-washing and ban hand-to-hand greetings altogether. "That's already starting to happen" in a lot of places, she says.
She says she "can't even imagine" health workers and patients greeting one another with a casual fist bump. A nod or slight bow might be nicer, she says.
Whitworth concedes that the perceived informality of fist bumps and high fives might be a problem. Figures as august as President Obama and the Dalai Lama have used them, he notes – "but I couldn't imagine the British prime minister doing that."
An 11-year-old's wish to give the gift of life to others came true on the last day of his life. The photograph below shows doctors bowing to Liang Yaoyi, a gifted student from Shenzhen, China, who died from a brain tumor in June. His mother can be seen crying in the background.
Liang was diagnosed with the tumor at the age of 9, just after he moved to Shenzhen to join his brother and sister, and to attend primary school, Shanghai Daily reports. One day, Liang felt dizzy and the next day had trouble walking, so his sister took him to a hospital where he learned he had a brain tumor.
Before passing away on June 6, Liang told his mother, Li Qun, that he wanted to donate his organs.
"There are many people doing great things in the world," he said according to China Daily. "They are great, and I want to be a great kid too."
CCTV News reported that Liang also said it was also a chance for him to be "alive in another way."
Liang's teacher said he may have learned of organ donation by reading stories in a school textbook. Liang's mother honored his wishes and doctors were able to save his kidneys and liver for donation, according to China Daily.
The picture has created a firestorm within Chinese media outlets and on Reddit, where users commented on the beauty of the photo, the strength of Liang and the importance of organ donation.
If you would like to learn more about how you can become an organ donor, contact Donate Life.
A second American aid worker in Liberia has tested positive for Ebola, according to the Christian humanitarian group she works for.
Nancy Writebol is employed by Serving in Mission, or SIM, in Liberia and was helping the joint SIM/Samaritan's Purse team that is treating Ebola patients in Monrovia, according to a Samaritan's Purse statement.
Writebol, who serves as SIM's personnel coordinator, has been living in Monrovia with her husband, David, according to SIM's website. The Charlotte, North Carolina, residents have been in Liberia since August 2013, according to the blog Writebols2Liberia. They have two adult children.
On Saturday, Samaritan's Purse announced that American doctor Kent Brantly had become infected. The 33-year-old former Indianapolis resident had been treating Ebola patients in Monrovia and started feeling ill, spokeswoman Melissa Strickland said. Once he started noticing the symptoms last week, Brantly isolated himself.
Brantly, the medical director for Samaritan Purse's Ebola Consolidated Case Management Center in Monrovia, has been in the country since October, Strickland said.
"When the Ebola outbreak hit, he took on responsibilities with our Ebola direct clinical treatment response, but he was serving in a missionary hospital in Liberia prior to his work with Ebola patients," she said.
Deadliest Ebola outbreak
Health officials say the Ebola outbreak, centered in West Africa, is the deadliest ever.
As of July 20, some 1,093 people in Guinea, Sierra Leone and Liberia are thought to have been infected by Ebola since its symptoms were first observed four months ago, according to the World Health Organization.
Testing confirmed the Ebola virus in 786 of those cases; 442 of those people died.
Of the 1,093 confirmed, probable and suspected cases, 660 people have died.
There also are fears the virus could spread to Africa's most populous country, Nigeria.
Last week, a Liberian man hospitalized with Ebola in Lagos died, Nigerian Health Minister Onyebuchi Chukwu said.
Lagos, the largest city in Nigeria, has a population of more than 20 million.
The man arrived at Lagos airport on July 20 and was isolated in a local hospital after showing symptoms associated with the virus. He told officials he had no direct contact with anyone with the virus nor had he attended the burial of anyone who died of Ebola.
Another doctor infected
Confirmation of the death in Lagos came after news that a doctor who has played a key role in fighting the Ebola outbreak in Sierra Leone is infected with the disease, according to that country's Ministry of Health.
Dr. Sheik Humarr Khan is being treated by the French aid group Medecins Sans Frontieres -- also known as Doctors Without Borders -- in Kailahun, Sierra Leone, agency spokesman Tim Shenk said.
Before falling ill, Khan had been overseeing Ebola treatment and isolation units at Kenema Government Hospital, about 185 miles east of the capital, Freetown.
Ebola typically kills 90% of those infected, but the death rate in this outbreak has dropped to roughly 60% because of early treatment.
Spread by bodily fluids
Officials believe the Ebola outbreak has taken such a strong hold in West Africa because of the proximity of the jungle -- where the virus originated -- to Conakry, Guinea, which has a population of 2 million.
Because symptoms don't immediately appear, the virus can easily spread as people travel around the region. Once infected with the virus, many people die in an average of 10 days as the blood fails to clot and hemorrhaging occurs.
The disease isn't contagious until symptoms appear. Symptoms include fever, headache and fatigue. At that point, the Ebola virus is spread via bodily fluids.
Health workers are at especially high risk, because they are in close contact with infected people and their bodily fluids. Adding to the danger, doctors may mistake the initial stages of an Ebola infection for another, milder illness.
Music has an unmatched power to bring back our pasts. But what if our memories have been lost to Alzheimer's or some other condition? Can music still work its magic?
A new film, Alive Inside, says yes. The film, opening Friday in New York, features the work of Dan Cohen, a New York social worker who started taking personalized iPods to people with dementia in nursing homes several years ago. Cohen's non-profit Music & Memory got a huge boost in 2012 when an early clip from the film, featuring a gentleman named Henry, became an online sensation. It has been viewed more than 10 million times at various websites, filmmaker Michael Rossato-Bennett says.
In the clip, Henry, then 94, is shown slumped and unresponsive in a wheelchair – until a nursing home worker places a set of headphones over his ears. Henry comes alive. He scats along with Cab Calloway and sings a soulful I'll Be Home for Christmas. The music "gives me the feeling of love, romance," he says.
Henry has since passed away, but that clip is one big reason that the Music & Memory program is in 640 nursing homes and assisted-living facilities, Cohen says. He says he won't be satisfied until personalized iPods – loaded with music especially chosen for each participant – are in all 16,000 U.S. nursing homes, available to all 1.6 million residents.
"Ninety-nine percent of these people are still sitting around and doing nothing all day when they could be rocking to their music," he says.
The reasons for Cohen's passion become clear in what Rossato-Bennett dubs "the only good-news film ever made about Alzheimer's." In segment after segment, people with Alzheimer's and other conditions don the headphones, hear the music of their youths and light up. A World War II veteran named John dances in his chair as the Andrews Sisters sing Oh Johnny, Oh Johnny, Oh! Another man holds his wife's hands and sings a duet of Can't Take My Eyes Off of You. An agitated woman becomes serene as she dances to strains of Schubert.
Such scenes are interspersed with comments from doctors, including the neurologist Oliver Sacks, who says, "Music has more ability to activate more parts of the brain than any other stimulus." Others talk about the need to reconnect with lonely, inactive and neglected elders, in and out of nursing homes.
Viewers might come away with the idea that a skillfully loaded iPod is a proven and universally effective cure for all that. In fact, the first big study of Music & Memory is just getting underway in Wisconsin, as part of a state-funded rollout in 200 nursing homes. Researchers will look at whether the approach improves social engagement and reduces agitation, anxiety and depression, say University of Wisconsin-Milwaukee researchers Jung Kwak and Michael Brondino. The study won't focus on memory but will look at overall effects on dementia, Brondino says. One thing they know, he says, is that staffs and patients "absolutely love this program."
The program, which relies on families and aides to work with patients, should not be confused with formal music therapy delivered by professionals trained in that discipline, says Alicia Clair, professor of music education and therapy at the University of Kansas.
Still, she says, "it's a wonderful thing" for many people. Caregivers need to know, she says, that not everyone will respond and that some people can even respond negatively. A song that stirs up sadness or anger might do more harm than good, she says.
Cohen says, "This is not a cure for Alzheimer's, and this does not work for everybody." But, he says, it is something just about anyone can try – something that might open up a whole lost world.
Cohen's tips for setting up an individualized music program and for donating used iPods to the program are at musicandmemory.org.
Alive Inside will open in theaters and be shown in film festivals around the country through mid-September.
Surviving a life-threatening illness or injury may be more likely if you're treated at a busy emergency department instead of one that handles fewer patients, a new study finds.
Researchers analyzed data on 17.5 million emergency patients treated at nearly 3,000 hospitals across the United States. The overall risk of death in the hospital was 10 percent lower among those who initially went to the busiest emergency departments rather than to the least busy ones, the study found.
"It's too early to say that based on these results, patients and first responders should change their decision about which hospital to choose in an emergency," said the study's lead author, Dr. Keith Kocher, an assistant professor of emergency medicine at the University of Michigan Medical School.
"But the bottom line is that emergency departments and hospitals perform differently, there really are differences in care and they matter," he added.
The survival difference was even greater for patients with serious, time-sensitive conditions. Death rates were 26 percent lower for sepsis patients and 22 percent lower for lung failure patients who went to the busiest emergency departments, compared to those who went to the least busy ones.
Heart attack patients were also more likely to survive if they went to the busiest emergency departments, according to the study published July 17 in the journal Annals of Emergency Medicine.
If all emergency patients received the kind of care provided at the busiest emergency departments, 24,000 fewer patients would die each year, the researchers said.
The finding held even when the researchers accounted for differences in the patients' health, income level, hospital location and technology, they said.
But the study wasn't designed to look into the reasons for the finding; it only found an association between better survival rates and busier ERs.
"The take-home message for patients is that you should still call 911 or seek the closest emergency care, because you don't know exactly what you're experiencing. What makes one hospital better than another is still a black box, and emergency medicine is still in its infancy in terms of figuring that out," Kocher said in a university news release.
"For those who study and want to improve emergency care and post-emergency care, we hope these findings will inform the way we identify conditions in the pre-hospital setting, where we send patients, and what we do once they arrive at the emergency department and we admit them to an inpatient bed," he added.
For women going through menopause, hot flashes can be one of the most uncomfortable symptoms. But a new study suggests that acupuncture may help to reduce the severity and frequency of hot flashes among menopausal women.
Hot flashes, also known as hot flushes, are a sudden feeling of heat over all or parts of the body. They may also cause redness on the face and neck, red blotches on the arms, back and chest, and heavy sweating or cold shivers. Many health conditions can cause hot flashes, but they are most common among women going through menopause.
The most effective treatment for hot flashes is hormone therapy - the use of medication that contains estrogen or progesterone. However, such treatment can increase the risk of other health conditions, including stroke, heart disease and cancer.
In this latest study, recently published in the journalMenopause, researchers wanted to see how acupuncture affected the regularity and severity of hot flashes a woman experienced while going through natural menopause.
Acupuncture is a form of alternative medicine that is more than 2,500 years old. It incorporates a number of procedures that stimulate anatomical points on the body as a form of healing. The most common form of acupuncture involves the use of thin, metallic needles that penetrate the skin.
The technique is most commonly used to help treat chronic pain, but past research has indicated it can help reduce inflammation and may even boost weight loss.
Acupuncture 'reduced severity and frequency of hot flashes for up to 3 months'
The research team analyzed 104 studies that assessed the effectiveness of acupuncture. The team included 12 of these studies in their research, involving 869 women between the ages of 40-60 who were going through natural menopause.
The women included in the study underwent various forms of acupuncture, including acupressure, electroacupuncture, laser acupuncture, ear acupuncture and traditional Chinese medicine acupuncture.
The investigators found that women who underwent acupuncture experienced a reduction in the severity and frequency of hot flashes for up to 3 months. Furthermore, the treatment appeared to have a beneficial effect on hot flashes regardless of the number of doses, sessions or duration of treatment received.
However, the researchers note that sham acupuncture reduced the frequency of hot flashes as much as true acupuncture.
The team is unable to explain why acupuncture appears to help alleviate hot flashes among menopausal women, but they hypothesize that acupuncture may trigger a reduction in the concentration of beta-endorphin - a neuropeptide found in the cells of the central and peripheral nervous system - in the hypothalamus of the brain. They say lower levels of beta-endorphin may activate the release of calcitonin gene-related peptide (CGRP), which regulates body temperature.
Commenting on the team's findings, Dr. Margery Gass, executive director of The North American Menopause Society (NAMS), says:
"More than anything, this review indicates that there is still much to be learned relative to the causes and treatments of menopausal hot flashes. The review suggests that acupuncture may be an effective alternative for reducing hot flashes, especially for those women seeking non-pharmacologic therapies."
A 2012 study, also published in the journal Menopause, suggested that hypnosis can also minimize the occurrence of hot flashes during menopause by around 75%.
(CNN) -- Do you tend to forget things when you're stressed? Like when you're late for a meeting and can't remember where you left your car keys? Or when you have to give a big presentation and suddenly forget all your talking points seconds before you start?
There's nothing like stress to make your memory go a little spotty. A 2010 study found that chronic stress reduces spatial memory: the memory that helps you recall locations and relate objects.
Hence, your missing car keys.
University of Iowa researchers recently found a connection between the stress hormone cortisol and short-term memory loss in older rats. Their findings, published in the Journal of Neuroscience this week, showed that cortisol reduced synapses -- connections between neurons -- in the animals' pre-frontal cortex, the area of the brain that houses short-term memory.
But there's a difference between how your brain processes long-term job stress, for example, and the stress of getting into a car accident. Research suggests low levels of anxiety can affect your ability to recall memories; acute or high-anxiety situations, on the other hand, can actually reinforce the learning process.
Acute stress increases your brain's ability to encode and recall traumatic events, according to studies. These memories get stored in the part of the brain responsible for survival, and serve as a warning and defense mechanism against future trauma.
If the stress you're experiencing is ongoing, however, there can be devastating effects.
Neuroscientists from the University of California, Berkeley,found that chronic stress can create long-term changes in the brain. Stress increases the development of white matter, which helps send messages across the brain, but decreases the number of neurons that assist with information processing.
The neuroscientists say the resulting imbalance can affect your brain's ability to communicate with itself, and make you more vulnerable to developing a mental illness.
Defects in white matter have been associated with schizophrenia, chronic depression, bipolar disorder, obsessive-compulsive disorder and post-traumatic stress disorder. Research on post-traumatic stress disorder further shows that it can reduce the amount of gray matter in the brain.
The Berkeley researchers believe their findings could explain why young people who are exposed to chronic stress early in life are prone to learning difficulties, anxiety and other mood disorders.
To reduce the effects of stress, the Mayo Clinic recommends identifying and reducing stress triggers. Eating a healthy diet, exercising, getting enough sleep and participating in a stress-reduction activity such as deep breathing, massage or yoga, can also help.
(CNN) -- Chikungunya -- a tropical disease with a funny name that packs a wallop like having your bones crushed -- has finally taken up residence in the United States.
Ever since the first local transmission of chikungunya was reported in the Americas late last year, health officials have been bracing for the arrival of the debilitating, mosquito-borne virus in the United States. Just seven months after the first cases were found in the Caribbean, the Centers for Disease Control and Preventionreported the first locally acquired case of chikungunya in Florida.
Even though chikungunya is not on the National Notifiable Diseases Surveillance System list, 31 states and two U.S. territories have reported cases of the disease since the beginning of the year. But only Puerto Rico and the U.S. Virgin Islands reported locally acquired cases. All the other cases were travelers who were infected in countries where the virus was endemic and were diagnosed upon returning to the United States.
That ended Thursday, when the CDC reported a man in Florida, who had not recently traveled outside the country, came down with the illness.
As of right now, the Florida Department of Health confirmed there are at least two cases. One case is in Miami Dade County and the other is in Palm Beach County.
Its arrival did not surprise the chair of the Florida Keys Mosquito Control Board.
"It was just a matter of when. We are prepared in the Keys and have been prepared for some time to deal with chikungunya," Steve Smith said. "From what I am seeing, I'm sure there are more cases out there that we don't know about. It's really a matter of time."
The CDC is working closely with the Florida Department of Health to investigate how the patient came down with the virus. The CDC will also monitor for additional locally acquired U.S. cases in the coming weeks and months.
The virus, which can cause joint pain and arthritis-like symptoms, has been on the U.S. public health radar for some time.
Usually about 25 to 28 infected travelers bring it to the United States each year. But this new case represents the first time that mosquitoes themselves are thought to have transferred the disease within the continental United States
"The arrival of chikungunya virus, first in the tropical Americas and now in the United States, underscores the risks posed by this and other exotic pathogens," said Roger Nasci, chief of CDC's Arboviral Diseases Branch. "This emphasizes the importance of CDC's health security initiatives designed to maintain effective surveillance networks, diagnostic laboratories and mosquito control programs both in the United States and around the world."
The virus is not deadly, but it can be extremely painful, with symptoms lasting for weeks. Those with weak immune systems, such as the elderly, are more likely to suffer from the virus' side effects than those who are healthier. About 60% to 90% of those infected will have symptoms, says Nasci. People infected with chikungunya will often have severe joint pain, particularly in their hands and feet, and can also quickly get very high fevers.
The good news, said Dr. William Schaffner, an infectious diseases expert with Vanderbilt University in Nashville, is that the United States is more sophisticated when it comes to controlling mosquitoes than many other nations and should be able to keep the problem under control.
"We live in a largely air-conditioned environment, and we have a lot of screening (window screens, porch screens)," Shaffner said. "So we can separate the humans from the mosquito population, but we cannot be completely be isolated."
Mosquito-borne virus worries CDC
Chikungunya was originally identified in East Africa in the 1950s. Then about 10 years ago, chikungunya spread to the Indian Ocean and India, and a few years later an outbreak in northern Italy sickened about 200 people. Now at least 74 countries plus the United States are reporting local transmission of the virus.
The ecological makeup of the United States supports the spread of an illness such as this, especially in the tropical areas of Florida and other Southern states, according to the CDC.
The other concern is the type of mosquito that carries the illness.
Unlike most mosquitoes that breed and prosper outside from dusk to dawn, the chikungunya virus is most often spread to people byAedes aegypti and Aedes albopictus mosquitoes, which are most active during the day, which makes it difficult to use the same chemical mosquito control measures.
These are the same mosquitoes that transmit the virus that causes dengue fever. The disease is transmitted from mosquito to human, human to mosquito and so forth. A female mosquito of this type lives three to four weeks and can bite someone every three to four days.
Shaffner and other health experts recommend people remember the mosquito-control basics:
-- Use bug spray if you are going out, especially in tropical or wooded areas near water.
-- Get rid of standing water in empty plastic pools, flower pots, pet dishes and gutters to eliminate mosquito breeding grounds.
Three more people in Colorado have been diagnosed with the plague after coming in contact with an infected dog whose owner contracted a life-threatening form of the disease, state health officials said on Friday.
In all, four people were infected with the disease from the same source, the Colorado Department of Public Health and Environment said in a statement.
Last week the department said a man in an eastern Colorado county whose dog died of the plague had been diagnosed with pneumonic plague, a rare and serious form of the disease.
The man remains hospitalized, but authorities have not released his condition.
The three people in the latest reported cases had "mild symptoms" and have fully recovered after being treated with antibiotics, the department said, adding that they are no longer contagious.
Two of the patients in the new cases contracted pneumonic plague, the department said.
Pneumonic plague is the only form of the disease that can be transmitted person-to-person, usually through infectious droplets from coughing.
The bacteria that causes plague occurs naturally in the western United States, primarily in California, New Mexico, Arizona and Colorado, according to the U.S. Centers for Disease Control and Prevention.
The infected canine in Colorado likely contracted the disease from prairie dogs or rabbits, which are the primary hosts for fleas that carry the bacteria.
When an infected animal dies, the fleas spread the disease when they find another host.
Colorado has seen a total of 12 cases of humans infected with the plague over the last decade, said Jennifer House, the department's public health veterinarian.
"We usually don't see an outbreak like this related to the same source," House said.
Colorado had not had a confirmed human case of pneumonic plague since 2004, she said.
It’s been nine months since the government shutdown, and some D.C. area hospitals are reporting a surprising development: Babies. Lots of them.
Sibley Memorial Hospital in Washington, D.C., has seen an additional three births per day in July, according to spokesman Gary Stephenson.
“We’re at near-capacity right now,” said Stephenson, joking that some furloughed workers “apparently found ways to amuse themselves.”
Virginia Hospital Center in Arlington delivered 99 more babies in April, May and June than they did in the same stretch last year, according to spokeswoman Maryanne Boster.
Both hospitals stopped short of crediting the two-week shutdown in October 2013 for the spike in births, stressing that the apparent link was purely anecdotal. But it’s not the first time a local baby boom has been blamed –- albeit anecdotally –- on an event nine months prior.
“It’s just so appealing to think, ‘Oh, it’s a full moon,’ or ‘it’s nine months after a blackout or Hurricane Sandy,’” said Dr. Marjorie Greenfield, chief of obstetrics and gynecology at University Hospitals Case Medical Center in Cleveland. “But there’s a lot of natural fluctuation.”
Some days Greenfield has 20 women in labor, she said. Other days, there are four.
“There are so many things that play into whether someone gets pregnant,” she said, explaining that a small proportion of furloughed couples would be fertile –- not to mention eager to conceive -– during the two-week shutdown.
“It’s such a sexy topic,” she said of the big event-baby boom link. “It just doesn’t appear to be real.”
But other OBs say they not only see an uptick in births nine months after unusual events like blizzards and blackouts, their patients say those events are why they got pregnant.
“I can say that I've definitely seen spikes after things like hurricanes, blackouts and blizzards,” said Dr. Jennifer Ashton, ABC News’ senior medical contributor and a practicing OB/GYN. “I’m not aware of any hard data on this, but anecdotally, many obstetricians will ask their patients about the events nine months prior, and many women will say 'Yes, we conceived during the blackout.'"
Ashton said it’s definitely possible that the link is coincidental, and said there tend to be seasonal fluctuations in birth rates as well.
Boster of Virginia Hospital Center said they expect to see the baby boom continue through the summer months “after the long, snowy winter.”
(CNN) -- In the future, a test of your sense of smell may help doctors predict your risk of developing Alzheimer's disease, according to new research presented at the Alzheimer's Association International Conference in Copenhagen, Denmark, this week.
In two separate studies, scientists found that people who were unable to identify certain odors were more likely to experience cognitive impairment. The researchers believe that brain cells crucial to a person's sense of smell are killed in the early stages of dementia.
Researchers say this information could help doctors create a smell test to detect Alzheimer's earlier. Early detection means early intervention and treatment to slow the progression of the disease. Doctors today can only diagnose Alzheimer's disease once it has caused significant brain damage.
"In the face of the growing worldwide Alzheimer's disease epidemic, there is a pressing need for simple, less invasive diagnostic tests that will identify the risk of Alzheimer's much earlier in the disease process," Heather Snyder, director of medical and scientific operations for the Alzheimer's Association, said in a statement.
More than 35 million people worldwide live with dementia today, according to a new report. By 2050, that number is expected tomore than triple to 115 million.
On Thursday, 3-year-old cancer patient Wyatt Schmaltz was sworn in as the nation’s youngest special sheriff deputy from his hospital room in Indianapolis.
In April, Wyatt was diagnosed with aggressive, stage 4 neuroblastoma and has undergone several rounds of chemotherapy. Soon, he’ll undergo surgery to remove a tumor from his abdomen and he will also undergo a stem cell transplant.
As a tribute to his courage throughout his treatments, an Indiana sheriff and a state trooper visited Wyatt at his room in Riley Hospital for Children at Indiana University Health, giving him the powers of a sheriff deputy – as well as a badge and uniform. Terry Stoffel, a sheriff for Huntington County, noted that the title is an official designation.
"We have given Wyatt all the powers of a real sheriff deputy, which are to carry out the orders of the sheriff. Right now, his only orders are to get better,” Stoffel said.
According to doctors at Riley Hospital, such acts of kindness can really help to make children well again.
"Gestures like this really aid the healing process for our patients," said Dr. Michele Saysana, a pediatrician with Riley Hospital for Children at IU Health. "It brought tears to our team members’ eyes to see officers, who are sworn to protect and serve, travel to pay tribute to one of our patients."
After being sworn in, Wyatt asked: “What else do you have?”
A girl believed to be “cured” of HIV at birth now has detectable levels of the virus, health officials said today.
The unnamed girl, dubbed the “Mississippi baby” after being born to an HIV-positive mother in 2010 and quickly treated with an intense dose of antiretroviral medication, showed no signs of the virus for roughly four years, according to the National Institute for Allergy and Infectious Disease. But a recent round of tests revealed detectable levels of HIV in her blood as well as antibodies to the virus and a decreased T-cell count -- all signs of the infection.
“Certainly, this is a disappointing turn of events for this young child, the medical staff involved in the child’s care, and the HIV/AIDS research community,” NIAID director Dr. Anthony Fauci said in a statement. “Scientifically, this development reminds us that we still have much more to learn about the intricacies of HIV infection and where the virus hides in the body.”
The case of the Mississippi baby made headlines across the globe after being published in the New England Journal of Medicine. Dr. Hannah Gay, the University of Mississippi Medical Center pediatrician who treated the infant at birth, was listed as one of Time magazine’s most influential people of 2013.
Gay's decision to give the newborn antiretroviral medication in the days before it was confirmed that she was in fact HIV-positive was controversial, since there was only a 25 percent chance that the girl would contract the virus from her mother.
The girl continued treatment for 18 months before her mother stopped taking her to her clinic appointments. Five months later, when she went back for a check-up, she surprised doctors with undetectable levels of the virus.
At first, Gay and her colleagues said the baby had been “functionally cured” of the virus, but later revised their language to “remission” to better convey that there was a chance the virus could rebound, they said at the time.
Although the girl's positive test results have been described as a disappointment, experts say her case still shows tremendous progress in treating the virus that causes AIDS.
“The fact that this child was able to remain off antiretroviral treatment for two years and maintain quiescent virus for that length of time is unprecedented,” Dr. Deborah Persaud, professor of infectious diseases at the John Hopkins Children’s Center in Baltimore, said in a statement released by NIAID. “Typically, when treatment is stopped, HIV levels rebound within weeks, not years.”
Persaud is one of the two pediatric HIV experts involved in the ongoing analysis of the case.
“This virus is amazingly recalcitrant,” said Fauci. “It’s in reservoirs, except we don’t know every place in the body where the reservoir is going to be.”
NIAID and the National Institute of Child Health and Human Development announced today that they would provide funding to analyze the unique case and will take the new findings into account during a new clinical trial.
As hearing aid technology has improved, so has health reporter Kathleen Raven's confidence.
When she was 5 years old, she found out she had a hearing problem. Complications during her birth led to damage in her inner ear.
"I couldn't hear water dripping from a faucet. I couldn't hear crickets on a summer night," she tells NPR's Kelly McEvers. "I couldn't hear sirens, couldn't hear fire alarms in our school fire drills, so I did a lot of watching other people."
The diagnosis was moderate to severe loss of high- and low-frequency hearing. When it comes to speech, certain sounds are out of range for her. Sounds like "ch," "sh" and "th" blend together.
Raven says she reads lips "religiously," but when she can't see a person's lips, she can understand maybe every third word — that is, without a hearing aid.
She got her first hearing aids — a large, clunky set — back when she was 5 in 1993.
"They were about 2 inches long and very thick, and they connected to a very large ear mold inside my ear," she says. "They call them flesh-colored, but they're not the color of anyone's flesh." Her young classmates teased her.
But the technology kept changing. Every few years, her parents would shell out $4,000 to $5,000 on each new device. By the time she got to high school, she had her first completely inside-the-ear hearing aid. That changed everything.
"I just became more confident walking into crowds. I didn't try to hide, I didn't arrange my hair to cover my ears. I started being more talkative, going out with my friends more," says Raven. "I didn't realize how much that fear had impacted me until I got completely in-the-ear hearing aids."
She went on to college and started pursuing her dream of reporting.
"I encountered a few raised eyebrows along the way," she says. "Why do you want to make a living of hearing people when that's a challenge for you?"
She pushed past the skeptics and became a reporter. Today she writes about oncology forBioPharm Insight.
As years passed and the technology progressed, Raven thought her hearing had maxed out. But with each upgrade, she discovered more sounds. Two years ago, she received her latest pair, which cost $7,000.
When her audiologist put them in her ears, she heard an unfamiliar noise. "I just happened to smack my lips together, like you're tasting something," she recalls. "It's just such a simple sound, but it was earth-shattering."
Her audiologist put on Beethoven, and she heard new instruments and trills. "It was like seeing the world in 3-D, or hearing the world in 3-D for the first time," Raven says.
These latest hearing aids are basically invisible. Even still, now she tells people about her hearing loss.
"Five years ago, I still was not ever telling people unless it was absolutely necessary. And now I do work it into conversation in the first five minutes or so," she says. If she needs to ask someone to repeat something, she'll just add, "I have a hearing problem."
"That phrase was impossible for me to say for the first 20 years of my life," Raven says. "Now I think it's very important for hearing loss to be accepted for younger people, of course, and also for older people."
Every working breastfeeding mother has had it happen at least once: You're on a break, ready to pump, when you discover you forgot a crucial piece of equipment.
Maybe it's a valve, a piece of tubing or a storage bag. You find yourself wondering if you can store milk in a water bottle or use butter as a nipple cream because there's no time to run home. What can you do?
Workers at Johns Hopkins Hospital can now purchase breastfeeding equipment from a vending machine -- believed to be the first of its kind.
The machine, which was installed last month, stocks pump accessories, storage bottles, breast pads and nipple cream, among other supplies for nursing mothers.
It's the brain child of Meg Stoltzfus, Lifespan Services Manager for the Office of Work, Life and Engagement at Hopkins.
"I worked and pumped as well, so I've made it sort of a mission to help other moms," she said.
Stoltzfus was walking through an airport last year when she noticed what a large variety of items are sold in vending machines. It occurred to her that a vending machine would be the perfect way to provide pumping equipment for mothers at the hospital, who often work unusual hours and may need equipment when the hospital gift shops are closed.
Stoltzfus worked directly with a manufacturer to design a machine that specializes in pumping gear. It was installed last month in a nursing mother's room in the hospital's Nelson building.
As an added bonus, the equipment is sold at a discount because it is an employee benefit. Customers swipe a credit or debit card to purchase items.
"I tried to brainstorm the kinds of things people forget," or don't have time to purchase after work, Stoltzfus said.
Stoltzfus believes that the vending machine is the first of its kind. Representatives from the two major breast-pump companies -- Medela and Ameda -- said they had not seen one before. Nor had other work life professionals who attended a recent conference hosted by Hopkins.
Hopkins -- the hospital, university and other affiliates -- has 14 dedicated nursing-mothers' rooms equipped with hospital grade pumps, so women don't have to lug a pump to work. The rooms also have microwaves and refrigerators to sterilize equipment and store milk.
"It ties into our mission of retaining wonderful employees," Stoltzfus said.
She said she might add another machine at an additional Hopkins location if this one catches on, and she said other institutions have expressed interest in following suit.
Should more places have these vending machines available to the public? Comment below!
At home in Lisbon, a gay couple invited friends over to a birthday celebration, and at the end of the evening shared a surprise — an ultrasound image of their baby, moving around in the belly of a woman in Pennsylvania being paid to carry their child.
“Everyone was shocked, and asked everything about how we do this,” said Paulo, who spoke on the condition that neither his last name nor that of his husband, João, be used since what they were doing is a crime in Portugal.
While babies through surrogacy have become increasingly common in the United States, with celebrities like Elton John, Sarah Jessica Parker and Jimmy Fallon openly discussing how they started a family, the situation is quite different in Portugal — as it is in most of the world where the hiring of a woman to carry a child is forbidden. And as Paulo and João have discovered, even bringing home a baby born abroad through surrogacy can be complicated.
In an era of globalization, the market for children crosses national borders; witness the longtime flow of Americans who have gone overseas to adopt babies from South Korea, China, Russia and Guatemala.
Other than the United States, only a few countries — among them India, Thailand, Ukraine and Mexico — allow paid surrogacy. As a result, there is an increasing flow in the opposite direction, with the United States drawing affluent couples from Europe, Asia and Australia. Indeed, many large surrogacy agencies in the United States say international clients — gay, straight, married or single — provide the bulk of their business.
The traffic highlights a divide between the United States and much of the world over fundamental questions about what constitutes a family, who is considered a legal parent, who is eligible for citizenship and whether paid childbirth is a service or exploitation.
In many nations, a situation that splits motherhood between the biological mother and a surrogate carrier is widely believed to be against the child’s best interests. And even more so when three women are involved: the genetic mother, whose egg is used; the mother who carries the baby; and the one who commissioned and will raise the child.
Many countries forbid advertising foreign or domestic surrogacy services and allow only what is known as altruistic surrogacy, in which the woman carrying the baby receives payment only for her expenses. Those countries abhor what they call the commercialization of baby making and view commercial surrogacy as inherently exploitive of poor women, noting that affluent women generally do not rent out their wombs.
But while many states, including New York, ban surrogacy, others, like California, welcome it as a legitimate business. Together, domestic and international couples will have more than 2,000 babies through gestational surrogacy in the United States this year, almost three times as many as a decade ago. Ads galore seek egg donors, would-be parents, would-be surrogates. Many surrogates and intended parents find each other on the Internet and make their arrangements independently, sometimes without a lawyer or a formal contract.
The agencies that match intended parents and surrogates are unregulated, creating a marketplace where vulnerable clients yearning for a baby can be preyed upon by the unscrupulous or incompetent. Some agencies pop up briefly, then disappear. Others have taken money that was supposed to be in escrow for the surrogate, or failed to pay the fees the money was to cover.
Surrogacy began in the United States more than 30 years ago, soon after the first baby was born through in vitro fertilization in England. At the time, most surrogates were also the genetic mothers, becoming pregnant through artificial insemination with the sperm of the intended father. But that changed after the Baby M case in 1986, in which the surrogate, Mary Beth Whitehead, refused to give the baby to the biological father and his wife. In the wake of the spectacle of two families fighting over a baby who belonged to both of them, traditional surrogacy gave way to gestational surrogacy, in which an embryo is created in the laboratory — sometimes using eggs and sperm from the parents, sometimes from donors — and transferred to a surrogate who has no genetic link to the baby.
But thorny questions remain: How much extra will the surrogate be paid for a cesarean section, multiple births — or loss of her uterus? What if the intended parents die during the pregnancy? How long will the surrogate abstain from sex? If she needs bed rest, how much will the intended parents pay to replace her paycheck, and cover child care and housekeeping?
“The gestational carrier has to agree to follow medical advice, but there has to be some level of trust,” said Andrew W. Vorzimer, a Los Angeles surrogacy lawyer who advises on many arrangements that have gone awry. “Once everyone goes home and the doors are closed, there’s no way to really monitor what’s going on.”
Since the Baby M case, the common wisdom has been that the main risk for parents is the surrogate’s changing her mind. But Mr. Vorzimer, who has tracked problem cases in the United States over the years, said it was the reverse: Trouble most often starts with the intended parents. One intended mother decided, well into the pregnancy, that she could not raise a child that was not genetically hers. Another couple, after a divorce, offered the surrogate mother money to have an abortion.
Over the decades, Mr. Vorzimer said, there have been 81 cases of intended parents who changed their minds and 35 in which the surrogate did — 24 of them traditional surrogates who both provided the egg and carried the baby.
Surrogacy remains controversial, even in the United States, despite the rapid proliferation of clinics, doctors and agencies. When all goes well, supporters say, the arrival of a baby to parents with no other path to a biological child is an unparalleled joy.
Opponents tend to focus on the cases in which the surrogate suffers health problems or is abandoned by the intended parents, or in which the fetus has serious defects. Abortion politics hang heavily over the issue: Often, surrogacy involves twin or triplet pregnancies, with the possibility of selective reduction.
Critics sometimes draw an analogy to prostitution, another subject that raises debate over whether making money off a woman’s body represents empowerment or exploitation.
In Canada, as in Britain, payment for surrogacy is limited to expenses.
“Just like we don’t pay for blood or semen, we don’t pay for eggs or sperm or babies,” said Abby Lippman, an emeritus professor at McGill University in Montreal who studies reproductive technology. “There’s a very general consensus that paying surrogates would commodify women and their bodies. I think in the United States, it’s so consumer-oriented, so commercially oriented, so caught up in this ‘It’s my right to have a baby’ approach, that people gloss over some big issues.”
Germany flatly prohibits surrogacy, with an Embryo Protection Act that forbids implanting embryos in anyone but the woman who provided the egg. Ingrid Schneider of the University of Hamburg’s Research Center for Biotechnology, Society and the Environment said it is in children’s best interest to know that they have just one mother.
“We regard surrogacy as exploitation of women and their reproductive capacities,” Dr. Schneider said. “In our view, the bonding process between a mother and her child starts earlier than at the moment of giving birth. It is an ongoing process during pregnancy itself, in which an intense relationship is being built between a woman and her child-to-be. These bonds are essential for creating the grounds for a successful parenthood, and in our view, they protect both the mother and the child.”
With all that is known about adopted children’s seeking out their biological parents, other European experts say, it is wrongheaded to create children whose relationship with the woman who provided the egg or carried them will be severed.
Emotional and Financial Costs
The restrictions in many countries have been a boost for American surrogacy. For overseas couples, the big draw is the knowledge that many states have sophisticated fertility clinics, experienced lawyers, a large pool of egg donors and surrogates, and, especially, established legal precedent.
“We chose the United States because of the certainty of the legal process,” said Paulo, an engineer and scrub nurse. “Surrogacy is very secretive in Portugal. People don’t talk about surrogacy, and it’s hard to get any information. In the United States it is all clear.”
But it is not cheap. International would-be parents often pay $150,000 or more, an amount that rises rapidly for those who do not get a viable pregnancy on their first try. Prices vary by region, but surrogates usually receive $20,000 to $30,000, egg donors $5,000 to $10,000 (more for the Ivy League student-athlete, or model), the fertility clinic and doctor $30,000, the surrogacy agency $20,000 and the lawyers $10,000. In addition, the intended parents pay for insurance, fertility medication, and incidentals like the surrogate’s travel and maternity clothes.
Because surrogacy is so expensive in the United States, many couples travel to India, Thailand or Mexico, where the total process costs half or less. But complications have arisen — as in the case of a couple stuck in India for six years, trying to take home a baby boy, whom genetic testing had found not to be related to them, apparently because of a mix-up with the sperm donation.
Four years ago, according to Stuart Bell, the chief executive of Growing Generations, a Los Angeles surrogacy agency, only about 20 percent of its clients came from overseas, but now international clients are more than half. Other agencies report the same trend.
“Anyone who can afford it chooses the United States,” said Lesa A. Slaughter, a fertility lawyer in Los Angeles.
Some lawyers who handle surrogacy tell of ethical problems with intended parents from abroad. Melissa Brisman, a New Jersey lawyer who handled Paulo and João’s surrogacy, had a prospective client from China who wanted to use five simultaneous gestational surrogates. She turned him down.
Mr. Vorzimer, in California, had an international client who wanted six embryos implanted.
“He wanted to keep two babies, and put the rest up for adoption,” Mr. Vorzimer said. “I said, ‘What, like the pick of the litter?’ and he said, ‘That’s right.’ I told him I wouldn’t work with him.”
Probably the most agonizing cases, though, are those in which the intended parents and the surrogate do not agree on what to do about a fetus with severe defects.
Heather Rice, an Arizona mother of three, said her first surrogacy was “an experience so great I knew I wanted to do it again.” She had a very different experience the second time, when, after two miscarriages, a routine ultrasound showed that the 21-week-old fetus had a cleft in his brain.
“Mom walked out of the room, left me lying there, and I thought: ‘This is not my baby. I should not be dealing with this by myself,' ” she said. “But I told Mom, ‘I’ll respect your decision, whatever you decide, because this is your baby.’ A couple days later, they called and told me they didn’t want their little boy so I should get an abortion.”
With only days left before an abortion would become illegal under Arizona law, Ms. Rice found herself unwilling to kill the fetus.
“I think my motherly instincts kicked in when they didn’t want him,” she said. “I told them I just couldn’t do it. Dad told me God was going to punish me for disobeying them.”
Ms. Rice found a woman whose child had the same condition who wanted the baby. And on the 28-week ultrasound, the brain looked somewhat better. When Ms. Rice called and told the intended parents that someone would take the baby, they said they had decided they wanted him after all. At the delivery, though, the mother did not show up.
“When I called, she said Dad had been in the waiting room all night,” Ms. Rice said. “I was crying. I said he has to come in; he’s the father; he should be here. He came in, he cut the cord. He took the baby. And that’s the last I ever heard from them.”
Ms. Rice said she had no idea how the baby was doing, or even whether his biological parents had kept him.
“I found them on Facebook, and there’s no trace of him, so I think they gave him up for adoption,” she said. “I don’t know where he is, and it kills me every day.”
Many women who have had a fulfilling surrogate experience go on to carry a second, or third, child for the same couple, finding pleasure in being pregnant and conferring the gift of a child and a continuing connection with another family, while earning money in the process. Kelly, a licensed practical nurse in Pennsylvania with two children who asked not to have her last name used to protect her privacy, delivered a baby, Nico, for two German men, Thomas Reuss and Dennis Reuther, in 2012, and is now pregnant with their twins, two more boys.
“I love being pregnant, but I don’t want to have any more children — oh, getting up in the middle of the night; oh, day care; oh, I’m done,” she said. “It’s great to see Thomas and Dennis with Nico, and how excited they are about twins. The money is nice, but we could manage without it, and it’s not why I’m doing this.”
Undeterred by Local Laws
For the Portuguese couple, the journey began when Paulo saw a television report about surrogacy, showing a gay couple who were unidentifiable in the shadows. The next day, he went to the television studio to ask how to find the two men. The producer would not share their names, but on rewatching, Paulo and João saw the name of the Connecticut fertility clinic.
Two years later, they were in a hotel in central Pennsylvania for the birth of their son, Diogo. His American passport had arrived. The bittersweet farewell dinner with the surrogate and her family was over, and the flight home was booked for the next day. All that was left to do was gaze at their sleeping baby, angelic in his white onesie, his starfish hands extended.
“It’s like a miracle,” said Paulo. “I cried when I saw the flight booking on the computer. I said: ‘Look, João. It’s not us two anymore. We are three.' ”
Getting to three was long, stressful and expensive, with problems at almost every turn — and one large hurdle remaining, as they apply for Diogo’s Portuguese citizenship.
After speaking to the Connecticut clinic, they chose a surrogacy agency that asked them to wire $100,000 up front. On the verge of sending the money, João decided that was too much. Without telling Paulo, he went back to his online research, and discovered complaints against that agency. Their second agency did not work, either: After months of back and forth, the agency turned them down, apparently because of concerns over their finances.
“They wasted almost a year of our time,” Paulo said.
Even with an agency they praise as responsible and responsive — an agency owned by Ms. Brisman, the New Jersey lawyer — obstacles continued. Their first donor’s eggs did not produce a pregnancy. The second had a genetic disorder that did not show up in the initial paperwork. A third produced a good supply of eggs, but after the first embryo was implanted, the surrogate miscarried. Their next surrogate did not get pregnant on the first try.
Through it all, the bills mounted. João and Paulo said they planned to burn them so their son would never have to think about the price, which they acknowledged was hundreds of thousands of dollars.
They have also decided not to answer any questions about which of them is the father — embryos that were inseminated by each were implanted — unless Diogo is the one asking.
“The information belongs to him,” Paolo said.
In the end, their warm relationship with the woman who bore their child was about the smoothest part of the process. The night before they were to take Diogo home, she sent an emotional text: “I know I’m doing well because I haven’t cried yet,” she said. “But I know I will.”
João and Paulo, like most international couples using an American surrogate, want their baby to be a citizen of their home country. But many Chinese parents take a different tack, keeping the American citizenship automatically conferred on every baby born here. Some hope the baby will attend an American university or help the family to live and work in the United States. But for Chinese clients, too, overseas surrogacy carries a complication, making it difficult for the baby to get a hukou, or household registration card, granting access to local schools and hospitals.
And there is another issue in China: restrictions on the number of children per family. Some Chinese couples, particularly older couples, turn to American surrogacy for a second child, whose American citizenship might clear the family from scrutiny.
But most surrogacy agencies say they will work only with intended parents who cannot carry their own baby, as recommended by the guidelines of the American Society for Reproductive Medicine. So Chinese clients who seek an overseas surrogate to get around the one-child rule create a dilemma.
“We usually only take clients who have a medical need for surrogacy, but in December, we decided to bend that rule, for Chinese people, government officials, who would be in trouble if they break the one-child rule,” said Karen Synesiou, chief executive of the Center for Surrogate Parenting, in Encino, Calif. “We’re thinking of it as political surrogacy.”
Then, too, agencies and lawyers say, there has been a recent uptick in the number of clients seeking “social surrogacy” — that is, having someone else carry their baby so as not to damage their career, or their figure. And not all agencies follow the guidelines.
“We don’t feel like we should be the gatekeepers when it comes to that,” said Saira Jhutty, chief executive of Conceptual Options, a California agency.
Final Hurdles at Home
For all the intimacy of carrying a baby for someone else, there is no template for the relationship between intended parents and the woman who will bear their child. Most contracts contain a clause requiring confidentiality unless both parties agree otherwise. And most stipulate that there will be an abortion if the fetus has serious defects, or a reduction in case of triplets or quadruplets. While no court would force a woman to have an abortion, lawyers say, a surrogate who refused to honor the agreement, and proceeded to carry a baby to term against the intended parents’ wishes, could perhaps be made to pay the costs of rearing the child, under the legal concept of wrongful birth. As surrogacy spreads, lawyers say, litigation over such issues may erupt.
For those from abroad, getting an American-born baby home can involve tangled immigration problems. Some countries require a new birth certificate, a parental order or an adoption. Some will not accept an American birth certificate with two fathers listed as the parents. Occasionally, a baby can be denied entry into the parents’ home country.
But international law is catching up with social practice: On June 26, in a case involving two sets of children born to American surrogates, the European Court of Human Rights ruled that France had violated the European Convention on Human Rights, and undermined the children’s identity, by refusing to recognize their biological father as their legal parent, easing the way to French citizenship.
The decision will most likely smooth the path for Paulo, João and their son, who entered Portugal on his American passport. So far, efforts to register Diogo in Portugal have failed, because the Portuguese process requires that a mother be named. Meanwhile, they have been advised to seek a residence card for him.
“They told us to wait three months for an answer,” Paulo said in a recent email. “We still do not know how this will end.”
In an unusual and powerful educational session held on the last day of the American Society of Clinical Oncology Annual Meeting, three oncologists shared what they have learned from their personal experiences with cancer, and how what they have learned has improved their practices.
“It's very difficult to speak about these issues in a public forum,” said session moderator Teresa A. Gilewski, MD, an oncologist in the Department of Medicine at Memorial Sloan Kettering Cancer Center, who has organized and led several innovative sessions at ASCO meetings over the years. She thanked the speakers for being willing to share their personal stories with the ASCO audience despite the strong emotions their stories clearly triggered in all those in the room.
The first to speak, Andrew S. Artz, MD, MS, Associate Professor of Medicine and Clinical Director of Hematopoietic Cellular Therapy at the University of Chicago Medical Center, related how his three-week-old daughter displayed a tumor in her left eye, and a suspicious area in her right eye, first detected by his wife. They obtained an immediate referral to a pediatric ophthalmologist from the baby's pediatrician.
The diagnosis after genetic testing was that the tumor was advanced retinoblastoma due to a mutation (based on her young age and two unaffected older siblings). The baby's rare cancer was a shock; he noted that there was no history of cancer in his family.
“It was a drastic transformation for me,” said Artz of the experience with his baby. “I never realized how anxiety-provoking the word ‘suspicious’ was until you're faced with ‘suspicious’ yourself.”
Artz and his wife were offered three treatment options, one of which was immediate enucleation of the left eye, and one of which was an investigational intra-arterial chemotherapy treatment approach, which was initially discouraged by the specialists they consulted.
“Remember, I'm already at a university; these are my colleagues,” he said. While being at a major medical center was an advantage, it also presented a delicate balancing act in terms of seeking additional opinions on his daughter's cancer. Ultimately, he and his wife chose the investigational retinoblastoma treatment following systemic chemotherapy. The baby had a recurrence one year later, which was treated with intravitreal chemotherapy; and she is now fine, yet will continue to have a lifelong increased risk of cancer.
Artz said he has learned a great deal from his personal experience about how oncologists can better help cancer patients cope: “To us it's a stage; but patients want to tell you about how it was diagnosed,” he said. In short, they want to tell their story to the oncologist. “That initial experience [with a patient] paints a canvas of who you are.”
Now, in his practice, he said, “I am more humble and more patient-centric; I am more willing to offer non-cancer related advice [on caregiving and caregivers, for example]. In addition, “I ask for feedback from patients, and I schedule more time for new patients.”
He offers this advice to oncologists: “Don't try to walk in a patient's shoes, just make the shoes fit better.” From his own experience, Artz has also developed specific suggestions for oncologists on interacting with cancer patients and their families (see box, next page).
In the summer of 2006, the late neurosurgeon Kelvin A. Von Roenn, MD—known for his dedication to training young residents in the art and science of neurosurgery—began to show serious and ominous physical symptoms. “I thought I knew a whole lot about grief until I experienced it myself,” said his wife, Jamie H. Von Roenn, MD, Professor of Medicine at Northwestern University's Feinberg School of Medicine and ASCO's Senior Director of Education, Science, and Professional Development.
Her husband had fatigue, nausea, a decrease in appetite, renal failure, and a bilateral ureteral obstruction; his diagnosis was undifferentiated small cell carcinoma of the renal pelvis. His blood urea nitrogen (BUN) level rose to 100, and he had dialysis and chemotherapy and underwent a nephrostomy. His wife knew too well that his prognosis was poor.
“He was kind of a stubborn ‘I can do anything’ kind of guy,” she said. She told his oncologist, “He wants it straight.” The treating oncologist told the Von Roenns that Kelvin (who had brain metastases) had perhaps six months to a year to live. As an oncologist, “I knew it couldn't be that long, but I wanted to believe it,” said Jamie Von Roenn; her husband died in October 2006 at the age of 56.
At the time of diagnosis, the Von Roenns had been married for nearly 28 years; their three children were 14, 16, and 22.
After his diagnosis, the Von Roenns, who were in the habit of going out on a date every Saturday night, sat on their bed and cried. “That night was the only time he cried,” Jamie Von Roenn remembered. “He wasn't up to going down and talking to the kids, so I did.”
Through her personal experience with her husband's incurable cancer, Jamie Von Roenn said she has learned many lessons or had ones she already knew reinforced. The first was that “even in an excellent hospital, it's stunning to me how terrible the care can be... if I wasn't there, he would not have been OK.”
The second was that most patients want the truth about their disease: “It undermines the hope people have when you don't tell them the truth,” she said, because it prevents them from making the most of the time they have left.
The Von Roenns chose hospice care at home, which she calls “good in the midst of bad.” Kelvin Von Roenn was cared for on the first floor of their home. “The most frightened I ever saw him was when he was tied in a wheelchair and we carried him downstairs,” she said.
During his last days, she and her husband went through what she calls the “five things” people need to say to each other when someone is dying: “I forgive you, forgive me, thank you, I love you, and goodbye.” One evening each of their children went in and talked to their father and went through the five things with him.
“We had our last days as a family,” said Jamie Von Roenn. Her husband's elderly mother managed to come to see him, since he could not go to her. Her husband and she planned his funeral; “It makes a huge difference to know what someone wants,” she said. “He was determined in his last weeks of life to help me with financial things,” an area he had handled. When their financial advisor cried, Jamie Von Roenn decided, “This is the person who cares,” the one she wanted to turn to for help with money issues.
Perhaps the biggest lesson she learned was how to deal with grief personally after her husband's death, which she said has given her an increased appreciation for helping families deal with grief: “The signs and symptoms of grief are emotional, physical, behavioral, and cognitive.”
The cognitive symptoms include preoccupation, confusion, and an inability to concentrate. She described the major tasks of grief as:
Accepting the reality of the loss;
Experiencing the pain;
Adjusting to an environment in which the deceased is missing;
Withdrawing emotional energy from the deceased and reinventing it; and
Writing a new story for one's life.
“As grief decreases, acceptance increases,” she said. She defined acceptance as “a sense of inner peace and tranquility that comes with the letting go of a struggle to regain what has been taken away — The only way out of this is resilience; that's the way we restart our lives.”
When Alyssa G. Rieber, MD, was 21 and a first-year medical student at the University of Alabama School of Medicine, she was diagnosed with Stage II Hodgkin lymphoma. At the ASCO meeting, she told the audience that this personal experience has given her a valuable perspective on treating the patients she sees today as Assistant Professor in the Department of General Oncology, Division of Cancer Medicine, at the University of Texas MD Anderson Cancer Center.
While a medical student, Rieber underwent four months of chemotherapy and then radiation, managing to continue on with her classes.
Unmarried at the time of diagnosis, Rieber learned how it feels to be a patient. Her mother, who did not cook, “started cooking like crazy,” Rieber remembered, in order to fill her daughter with nutritious food. “She would cook and I would throw food away,” Rieber said. She lost her appetite and had a metallic taste in her mouth. “I lost my hair, and everybody was concerned.” She resorted to wigs, “which are always too hot and itchy, and you end up wearing a hat anyway,” she remembered.
Rieber, now married with two young daughters, said that today when she interacts with families as an oncologist she tries to bring “honesty, empathy, encouragement, and hope.” She noted that “being able to talk to the person [oncologist] as someone who's gone through this is very helpful,” and that “Sometimes hope is all we have to offer to get them through the day.”
She said her experience as a cancer patient has helped her better understand the following:
The family response to a loved one's diagnosis of cancer brings shock, fear, and anxiety for everyone, and coping is different for everyone;
Family members have a heightened sense of their own mortality;
There may be a concern among some family members that cancer can be “caught,” especially among children (who need a careful explanation on their own level that cancer is not infectious);
The time to treatment seems extremely long to families, who have a sense of urgency; this requires taking the time to give an explanation of the steps needed to determine the best treatment before therapy can begin;
The family has concerns about the cancer patient's physical changes, such as weight loss, which can lead to battles over nutrition—wanting to feed the patient when he or she has no appetite and cannot eat. “I tell the patient, ‘Drink a shake,’ and I tell the family, ‘Back off,’” Rieber said;
The end of treatment doesn't necessarily mean a return to normalcy: “Just because treatment is over, that doesn't mean patients are back to ‘normal.’ Many people don't just bounce back,” Rieber said;
The end of treatment does not mean the end of worry, and of “the anxiety that never goes away.” The cancer survivor may feel that “every little lump is cancer until proven otherwise. The patients will have that forever.”
LITTLE ROCK, ARK. A south Arkansas woman celebrated her 116th birthday Friday with cake, a party and a new title - she's now officially the oldest confirmed living American and second-oldest person in the world, the Gerontology Research Group said.
Gertrude Weaver spent her birthday at home at Silver Oaks Health and Rehabilitation in Camden, about 100 miles southwest of Little Rock. This year's festivities included the new award from the Gerontology Research Group, which analyzed U.S. Census records to determine that Weaver is the oldest living American, rather than 115-year-old Jeralean Talley, who was born in 1899.
The research group, which consults with the Guinness Book of World Records, found that the 1900 Census listed Weaver as 2 years old - putting her birthday in 1898, said Robert Young, the research group's database administrator and senior consultant for Guinness.
That makes Weaver the second-oldest person in the world behind 116-year-old Misao Okawa of Japan and the 11th oldest person of all time, he said.
"Normally, 116 would be old enough to be the world's oldest person," Young said. "There's kind of heavy competition at the moment."
Weaver was born in southwest Arkansas near the border with Texas, and was married in 1915. She and her husband had four children, all of whom have died except for a 93-year-old son. Along with Census records, the Gerontology Research Group used Weaver's 1915 marriage certificate, which listed her age as 17, to confirm her birth year, Young said.
Although no birth record exists for Weaver, she celebrates her birthday each year on July 4 and did the same this year. At her 115th birthday party last year, Weaver was "waving and just eating it all up," said Vicki Vaughan, the marketing and admissions director at Silver Oaks.
"Most people want to know, `Well, can she talk?'" Vaughan said. "Her health is starting to decline a little bit this year - I can tell a difference from last year, but she still is up and gets out of the room and comes to all of her meals, comes to activities. She'll laugh and smile and clap."
Weaver first stayed at the Camden nursing home at the age of 104 after she suffered a broken hip, Vaughan said. But Weaver recovered after rehabilitation and moved back home with her granddaughter, before returning to the nursing home at the age of 109.
Weaver cited three factors for her longevity: "Trusting in the Lord, hard work and loving everybody."
"You have to follow God. Don't follow anyone else," she told the Camden News this week. "Be obedient and follow the laws and don't worry about anything. I've followed him for many, many years and I ain't tired."
Pregnancy, or the desire to become pregnant, often inspires women to take better care of themselves — quitting smoking, for example, or eating more nutritiously.
But now many women face an increasingly common problem: obesity, which affects 36 percent of women of childbearing age. In addition to hindering conception, obesity — defined as a body mass index above 30 — is linked to a host of difficulties during pregnancy, labor and delivery.
These range from gestational diabetes, hypertension and pre-eclampsia to miscarriage, premature birth, emergency cesarean delivery and stillbirth.
The infants of obese women are more likely to have congenital defects, and they are at greater risk of dying at or soon after birth. Babies who survive are more likely to develop hypertension and obesity as adults.
To be sure, most babies born to overweight and obese women are healthy. Yet a recently published analysis of 38 studies found that even modest increases in a woman’s pre-pregnancy weight raised the risks of fetal death, stillbirth and infant death.
Personal biases and concerns about professional liability lead some obstetricians to avoid obese patients. But Dr. Sigal Klipstein, chairwoman of the committee on ethics of the American College of Obstetricians and Gynecologists, says it is time for doctors to push aside prejudice and fear. They must take more positive steps to treat obese women who are pregnant or want to become pregnant.
Dr. Klipstein and her colleagues recently issued a report on ethical issues in caring for obese women. Obesity is commonly viewed as a personal failing that can be prevented or reversed through motivation and willpower. But the facts suggest otherwise.
Although some people manage to shed as much as 100 pounds and keep them off without surgery, many obese patients say they’ve tried everything, and nothing has worked. “Most obese women are not intentionally overeating or eating the wrong foods,” Dr. Klipstein said. “Obstetricians should address the problem, not abandon patients because they think they’re doing something wrong.”
Dr. Klipstein is a reproductive endocrinologist at InVia Fertility Specialists in Northbrook, Ill. In her experience, the women who manage to lose weight are usually highly motivated and use a commercial diet plan.
“But many fail even though they are very anxious to get pregnant and have a healthy pregnancy,” she said. “This is the new reality, and obstetricians have to be aware of that and know how to treat patients with weight issues.”
The committee report emphasizes that “obese patients should not be viewed differently from other patient populations that require additional care or who have increased risks of adverse medical outcomes.” Obese patients should be cared for “in a nonjudgmental manner,” it says, adding that it is unethical for doctors to refuse care within the scope of their expertise “solely because the patient is obese.”
Obstetricians should discuss the medical risks associated with obesity with their patients and “avoid blaming the patient for her increased weight,” the committee says. Any doctor who feels unable to provide effective care for an obese patient should seek a consultation or refer the woman to another doctor.
Obesity rates are highest among women “of lower socioeconomic status,” the report notes, and many obese women lack “access to healthy food choices and opportunities for regular exercise that would help them maintain a normal weight.”
Nonetheless, obese women who want to have a baby should not abandon all efforts to lose weight. Obstetricians who lack expertise in weight management can refer patients to dietitians who specialize in treating weight problems without relying on gimmicks or crash diets, which have their own health risks.
Weight loss is best attempted before a pregnancy. Last year, the college’s committee on obstetric practice advised obstetricians to “provide education about possible complications and encourage obese patients to undertake a weight-reduction program, including diet, exercise, and behavior modification, before attempting pregnancy.”
An obese woman who becomes pregnant should aim to gain less weight than would a normal-weight woman. The Institute of Medicine suggests a pregnancy weight gain of 15 to 25 pounds for overweight women and 11 to 20 pounds for obese women.
Although women should not try to lose weight during pregnancy, “a woman who weighs 300 pounds shouldn’t gain at all,” Dr. Klipstein said. “This is not harmful to the fetus.”
Dr. Klipstein also noted that obesity produces physiological changes that can affect pregnancy, starting with irregular ovulation that can result in infertility.
Obese women are more likely to have problems processing blood sugar, which raises the risk of birth defects and miscarriage. There is also a greater likelihood that their baby will be too large for a vaginal delivery, requiring a cesarean delivery that has its own risks involving anesthesia and surgery.
The babies of obese women are more likely to develop neural tube defects — spina bifida and anencephaly — and to suffer birth injuries like shoulder dystocia, which may occur when the infant is very large.
High blood pressure, more common in obesity, can result in pre-eclampsia during pregnancy, which can damage the mother’s kidneys and cause fetal complications like low birth weight, prematurity and stillbirth.
It is also harder to obtain reliable images on a sonogram when the woman is obese. This can delay detection of fetal or pregnancy abnormalities that require careful monitoring or medical intervention.
Ronnie and Donnie Galyon are eagerly awaiting a major milestone this Saturday. Even though it’s not the conjoined twins’ birthday, the duo plans to celebrate turning 62 years, 8 months and 7 days old with a big block party.
The reason for the celebration? The date means they will have lived longer than the original “Siamese Twins,” Chang and Eng Bunker, who became famous as a sideshow act in the 1800's.
“Put it this way -- I’m stoked,” Ronnie Galyon, 62, told the Denton Daily News.
Ronnie and Donnie Gaylon were born in 1951 and live with their younger brother, Jim Galyon, and his wife in Beavercreek, Ohio. The Galyon twins are joined from the breastbone area to the pelvis and spent their first months on Earth in the intensive care unit.
“They weren’t even expected to live the first day, let alone get out of the hospital, let alone live 62 years,” said Jim Galyon. “This has been a life-long goal to meet and beat the Bunker twins. It means the world to them.”
After growing up, the pair performed in carnival sideshows and circuses until they retired in 1991, according to the Associated Press. The Galyon twins lived on their own after retirement, although they moved just a few houses down from their brother so that he could help them. The twins moved in with their younger brother after they became deathly ill following a viral infection and were in the intensive care unit with various health problems, including blood clots in Ronnie’s lungs.
With the help of the community and the Christian Youth Corps, Jim Galyon was able to build an addition on his house and make it handicap accessible. He and his wife now care for his brothers 24 hours a day.
“[They] have their own totally different personalities,” said Jim Galyon. “Donnie can be very serious and reserved; Ronnie is very happy-go-lucky.”
While the duo is excited for the party on Saturday, they’re really anticipating their next birthday. This October the twins will turn 63, breaking the record for the oldest pair of conjoined twins, according to Guinness World Records.
The twins have been excited about breaking the official record for years.
“It’s what me and Donnie always dreamed about, and we hope to get the ring, because we’ve dreamed about getting this since we were kids,” Ronnie Galyon told the Denton Daily News.
As the Galyon twins plan to make history, their family is working on compiling a history of the twins’ former life on the road. They’re asking anyone who might have seen Ronnie and Donnie Galyon in their circus days to can contact the Galyon family at Worldsoldestconjoinedtwins@gmail.com.
When Bethany Townsend snapped herself on holiday with two of her colostomy bags visible, she didn’t expect the photo to be seen by more than 9 million people.
But since her photo went viral, hundreds of other people who live with Crohn’s disease are sharing photos of themselves with their colostomy bags on show.
When Joseph Hendy shared his story, people commented on his photo saying what an inspiration to others he was, adding: “I hope everybody with the same illness reads your story and takes the same positive attitude as yourself.”
AnneMarie said that the campaign made her feel brave enough to share her own photo. She wrote on Facebook: “By seeing these posts by so many brave people who have gone through the same, it has inspired me to take my very first photo of me and my stomach.”
Tina, shown in the middle here, said: “It’s really great to see so many people sharing their personal and difficult experiences publicly. An inspiration to all. Well here’s my pic, Hope it helps someone somewhere.”
Laura said she was proud to join the campaign, saying: “We have suffered in silence and been hiding behind this horrible condition for long enough!! Proud to be a part of it! Get ur belly out people!!!!”
Chances are, if you have been a nurse for more than six months, you have been exposed to bullying or disruptive behavior. Research shows that more than 82% of nurses have been a target of bullying or have witnessed it. Over 60% of new nurses who experienced bullying are planning to leave their jobs. The frightening part of these statistics is that bullying is underreported!
Defining Bullying
Bullying is not an isolated incident. It is deliberate, rude, inappropriate, and possibly aggressive behavior of a coworker(s) to another coworker. The behavior is repetitive in nature, and may be overt or covert. It can also reflect an actual or perceived imbalance or power or conflict.
Bullying and disruptive behavior has been recognized as a threat to a nurse’s well-being and a threat to the safety of our patients. When a care team cannot get along, errors are made, patients feel the tension, and patient outcomes suffer.
The paradox of bullying in nursing is that we all joined this marvelous profession because we are caring individuals. We want to show our compassion and be a healing presence to others. So how is it that this behavior is so prevalent in nursing? Research shows that the behavior continues because nurses are afraid of retaliation, normalize the behavior, don’t like conflict, and don’t really know what to do.
Here are 3 steps you can take to address this uncaring behavior in a caring way:
Stop and breathe!
Separate yourself from the behavior for a moment and realize that YOU are not the cause.
Diffuse the situation.
Do not react. Sometime reacting too fast can cause you to behave unprofessionally as well. As calmly as possible, ask to talk in private. If the behavior continues, be prepared to be the one to walk away.
Address the behavior.
Find a private place to openly discuss the behavior and address the conflict.
Two open ended discussion starters can be:
“When you yelled at me in front of the patient (or our co-workers), I felt humiliated. It was unprofessional and now the patient’s trust in the healthcare team has eroded. Was that your intent? Can we agree that in the future, if you have a problem with me, you will address it with me privately?”
“Are you OK? Help me to understand the situation. I’ve noticed a conflict between us and I think it’s affecting the way we work, can we talk about it?”
In a perfect world, these 3 steps can alleviate and resolve the conflict between nurse co-workers. However, be prepared that it may take further discussion and possibly, include your unit supervisor or nurse manager. By addressing uncaring behavior, you are standing up and choosing not to be a victim.
If you see someone else being bullied, don’t be a passive bystander. Stand next to the person and use supportive phrases while helping the person being bullied. This is especially if they are not able to speak for themselves at that moment. Most importantly, and most difficult to do: Stay calm, be confident, and always behave with integrity. Take the higher road.
Have you dealt with nurse bullies in the past? How did it go? Let us know in the comments.
WASHINGTON (AP) — Federal health regulators have approved a first-of-a-kind set of robotic leg braces that can help some disabled people walk again.
The ReWalk system functions like an exoskeleton for people paralyzed from the waist down, allowing them to stand and walk with assistance from a caretaker.
The device consists of leg braces with motion sensors and motorized joints that respond to subtle changes in upper-body movement and shifts in balance. A harness around the patient's waist and shoulders keeps the suit in place, and a backpack holds the computer and rechargeable battery. Crutches are used for stability.
ReWalk is intended for people who are disabled due to certain spinal cord injuries.
The device was developed by the founder of Israel-based Argo Medical Technologies, who was paralyzed in a 1997 car crash.
They’re just 12 miles and two train stops away, yet NewYork-Presbyterian Hospital and University Hospital, Newark, exist in “two different worlds,” says Terence Wrong, executive producer of ABC’s "NY Med."
The show, an eight-episode mini-series, returns Thursday night. In previous seasons it featured one or two top-tier hospitals – Baltimore’s Johns Hopkins Hospital in 2000 and 2008, Boston’s Brigham and Women’s and Mass General hospitals in 2010 and NewYork-Presbyterian Hospital and the city's Lutheran Medical Center in 2012. This year, however, it's turning its HD lenses on a premier hospital in one of the wealthiest zip codes in the world along with one that, while well-regarded, is located in a city that’s had nearly 7,000 shootings in the past decade alone.
The decision to examine the disparity is, in part, dramatic. “You really want to change tempos and speeds on the audience to have an alchemy in the show,” Wrong tells U.S. News.
Yet there’s a far larger idea at work, too.
“It is a tale of two cities,” he says. “The mainstream audience hasn’t really had life in the inner-city thrust in their face since 'The Wire' on HBO. Rather than demonize that world – because it is violent, people do have problems that they don’t necessarily have in Manhattan – what comes through to us is the extraordinary humanity of the patients we meet there and the way they bond and the way the nurses and doctors bond with them.”
The show, he insists, isn’t a typical medical or hospital show, with gratuitous gore or doctors hooking up or an unrelenting stream of life-and-death situations.
Produced through ABC’s news division, "NY Med" captures individual human dramas, Wrong explains, allowing it to paint an intimate and illuminating portrait of modern American health care. Issues range from the practical – “Who’s bearing the costs when a disadvantaged community uses the ER for primary care?" Wrong offers. "Does that impact the hospital’s bottom line?” – to the profound: “the individual will to live, connections and bonds between families and people and strangers,” he describes.
The first episode opens with a woman with a sunburn being rushed to a hospital by ambulance; – viewers soon see that the skin on her legs has bubbled to at least the size of tennis balls. The cameras cut to another patient, a man in the cardiac unit whose aorta begins to rip just as he’s being visited by cardiologist and TV star Dr. Mehmet Oz. Also on the same episode: a teen who was shot multiple times in Newark, a new female urologist helping insert a penile implant in a 73-year-old man, and a married father of three who’s about to have surgery for a tumor on his spine – and who has yet to tell his wife about it.
“Here’s a guy who doesn’t tell his wife that he’s got this life-threatening disease and they kind of capture that intimate moment where she gets through it,” says Dr. Philip Stieg, chief of neurosurgery at NewYork-Presbyterian/Weill Cornell Medical Center, who performs the operation. “Those are things that we as physicians, we have to deal with and help that family get through that.”
And throughout it all, the cameras keep rolling on these real-life patients, doctors and nurses.
Stieg, who says he was at first “skeptical” about participating in "NY Med," says he ultimately chose to take part because “neurosurgery has a story to tell.”
“There’s hundreds of thousands of neurosurgical procedures, and I’m hopeful that this small little vignette helps people understand that no matter how serious and critical the procedure may be, we have the technology to get you through that process,” he tells U.S. News. “That’s important for people to see. Let’s face it, at some point, all of us are going to be hospital patients.”
And that means the program doesn't merely show the drama of a complicated surgery or a patient fighting for his or her life, but the drama behind the drama: the new urologist struggling to set boundaries with her patients, a nurse struggling with her employers, and even doctors and nurses making mistakes during procedures. “Warts and all,” Wrong says.
“The cost of letting people see quality medical care is that, yeah, there will be warts and blemishes, because this is life,” he adds.
And that, in and of itself, has value.
“We do feel good that we can show the doctors and the nurses this way, and still so nobly,” supervising producer Erica Baumgart says. “One of the things that we sometimes hear from patients is that they want to participate in filming because it could help other people who have similar conditions get through what they can get through.”
New York state can end its three-decade HIV crisis by the year 2020, Gov. Andrew Cuomo said Sunday as he announced an ambitious plan to deliver a knockout blow to the epidemic by boosting testing, reducing new infections and expanding treatment.
The governor said the state is aiming to reduce new HIV diagnoses to 750 by the end of the decade - about the same number of tuberculosis cases seen in New York City each year - down from 3,000 expected this year and 14,000 new cases of the disease in 1993. If the state is successful, it would be the first time the number of people living with HIV has gone down since the crisis began with the first widely reported cases in 1981.
"Thirty years ago, New York was the epicenter of the AIDS crisis," Cuomo said. "Today I am proud to announce that we are in a position to be the first state in the nation committed to ending this epidemic."
To expand treatment, the state's Department of Health has negotiated bulk rebates with three companies producing HIV drugs. The state is also taking steps to make it easier to get tested, changing how HIV cases are tracked to ensure patients continue to receive treatment, and boosting access to "pre-exposure" drugs that can help high-risk people avoid infection.
Cuomo did not offer an estimate of the cost of the plan, but said it would end up saving the state more than $300 million per year by 2020 by reducing the amount the state pays for medical care for those with HIV.
Groups that have long advocated for HIV patients praised the governor's announcement, saying it shows that efforts to fight the disease are paying off, and that a scourge that once seemed unbeatable can be successfully fought.
"We have the tools and know-how to end the AIDS epidemic in New York, the only question is whether we have the political will," said Jason Walker, an organizer at VOCAL-NY, which advocates for low-income HIV patients. "Even without a vaccine or cure, Cuomo understands that we can dramatically reduce new infections below epidemic levels and ensure all people living with HIV achieve optimal health."
While the state's plan may sound overly optimistic, the number of new HIV cases in New York has dropped nearly 40 percent in the last 10 years because of better, faster tests; access to condoms; public outreach campaigns and other initiatives. Meanwhile, those with the disease are living longer thanks to significantly more effective treatments.
The goal of bringing the disease to below epidemic levels "is ambitious," said Mark Harrington, executive director of the anti-HIV organization Treatment Action Group, but "grounded in reality."
By Danielle Dellorto, Miriam Falco, and Jen Christensen
The Ebola epidemic isn't getting any better in Africa.
The World Health Organization reports there have been 759 cases, including 467 deaths in Guinea, Sierra Leone and Liberia since the outbreak began in March, according to a statement the organization released on Tuesday.
The World Health Organization has said "drastic action is needed" to stop the deadly outbreak in West Africa. It has sent teams of experts to help locals deal with the epidemic. WHO will meet this week to discuss how to contain it.
Relief workers on the ground said the epidemic has hit unprecedented proportions.
"The epidemic is out of control," said Dr. Bart Janssens, director of operations for Doctors Without Borders.
Complicating matters, the countries hit hardest by the epidemic have major medical infrastructure challenges. There is also a real sense of mistrust toward health workers from communities. In Sierra Leone and Guinea, WHO has said that community members have thrown stones at health care workers trying to investigate the outbreak.
In April, CNN Chief Medical Correspondent Dr. Sanjay Gupta traveled to Conakry, Guinea, to report on what was being done to treat patients and contain the outbreak.
"It took only moments to feel the impact of what was happening here," Gupta wrote after landing in Conakry. "There is a lot we know about Ebola, and it scares us almost as much as what we don't know."
Ebola outbreaks usually are confined to remote areas, making the disease easier to contain. But this outbreak is different; patients have been identified in 60 locations in Guinea, Sierra Leone and Liberia.
Officials believe the wide footprint of this outbreak is partly because of the proximity between the jungle where the virus was first identified and cities such as Conakry. The capital in Guinea has a population of 2 million and an international airport.
People are traveling without realizing they're carrying the deadly virus. It can take between two and 21 days after exposure for someone to feel sick.
Ebola is a violent killer. The symptoms, at first, mimic the flu: headache, fever, fatigue. What comes next sounds like something out of a horror movie: significant diarrhea and vomiting, while the virus shuts off the blood's ability to clot.
As a result, patients often suffer internal and external hemorrhaging. Many die in an average of 10 days.
Doctors Without Borders, also known as Médecins Sans Frontières, has been working to fight the epidemic since March. The group has sent more than 300 staff members and 40 tons of equipment and supplies to the region to help fight the epidemic.
Still, the group warns, it's not enough.
"Despite the human resources and equipment deployed by MSF in the three affected countries, we are no longer able to send teams to the new outbreak sites."
The good news is that Ebola isn't as easily spread as one may think. A patient isn't contagious -- meaning they can't spread the virus to other people -- until they are already showing symptoms.
Serious protective measures
Inside the isolation treatment areas in Conakry, doctors focus on keeping the patients hydrated with IV drips and other liquid nutrients. Health officials have urged residents to seek treatment at the first sign of flu-like symptoms.
There is no cure or vaccine to treat Ebola, but MSF has shown it doesn't have to be a death sentence if it's treated early. Ebola typically kills 90% of patients. This outbreak, the death rate has dropped to roughly 60%.
The outbreak will be considered contained after 42 days -- twice the incubation period -- with no new Ebola cases.
A huge thank-you to everyone who took our survey “Are You Way Too Stressed Out?”
A remarkable 3,312 of you took the time out of your busy day to complete the survey, and this high response rate highlights the seriousness of this issue to the nursing world.
The results of the survey reveal the dangerous levels of stress that RNs pervasively live with, both at work and in their personal lives. Lack of sleep, 12-hour shifts, night shifts, poor diets, unrealistic workloads, lack of authority at the workplace and unsupportive management are just some of the key contributors to the stress being experienced by RNs today.
RNs are neglected by a system that overworks, under-appreciates and marginalizes the experience of individuals who are the most connected to patients.
Respondents had the opportunity to answer the question, “What are some of the things that stress you out the most?” Many of you were brutally candid, and I cringe at what you continue to put up with on a daily basis. These five responses are representative of the thousands received.
“People who have never done your job telling you how to do it. People who have lost sight of the patient — the focus is the $$.”
“Not having the authority to take care of the things that need to be done, but being responsible for it.”
“Long hours (12-hr shifts), working nights, poor pay, poor benefits that are dependent on maintaining hours to prevent losing the benefits, lack of PTO to cover sick/vacation days.”
“Overwork with no relief in sight, working for $3 to $5 dollars less than average city wages …”
“Corporate chaos, lack of support, unrealistic expectations, being put in possible license jeopardy due to corporate greed and mismanagement.”
The system is broken! The very people treating patients are sick and in need of healing themselves. This is crazy.
The stress placed on RNs is eventually going to cause many of them to quit. Our nursing system is already grappling with an aging workforce and an aging general population. While the nation will need an increased number of RNs, we’re likely hurtling toward a nursing shortage. Stress leads to mistakes and errors, and hospital errors are already the third leading cause of death in the U.S. Put it all together, and we may be headed for a national healthcare crisis.
This is a report you will not want to miss. Download the full PDF report below and click through the SlideShare presentation, and share your own experiences with stress as an RN in the Reply section below. I want to hear from you!
A five-time national champion, Alysia Montano, was ready for another race on Thursday. But this race would be just a little different, since the former University of California star was 34-weeks pregnant.
“I’ve been running throughout my pregnancy and I felt really, really good during the whole process,” Montano said after the qualifying heat.
She finished last, but the crowd at Hornet Stadium still gave her a standing ovation. The 28-year-old ran the race in 2 minutes, 32.13 seconds. This comes about 35 seconds slower than her personal best of 1:57.34, which she ran in 2010 in Monaco.
Montano has been running all her life, and said she consulted with her doctor about her plan to continue running during her pregnancy, who encouraged the idea.
“That took away any fear of what the outside world might think ab out a woman running during her pregnancy,” Montano said. “What I found out mostly was that exercising during pregnancy is actually much better for the mom and the baby. … I did all the things I normally do … I just happened to be pregnant. This is my normal this year.”
A few weeks ago, senior vice-president Laszlo Bock took to Google’s official blog to publicly share the company’s employee demographics, revealing a predominately white male workforce and admitting a reluctance to come forward with the data earlier.
The announcement was deemed a groundbreaking disclosure, because U.S. companies are not obligated to make their workforce demographics public. However, citing that transparency is key to finding a solution, Mr. Bock wrote, “Simply put, Google is not where we want to be when it comes to diversity … our efforts, including going public with these numbers, are designed to help us recruit and develop the world’s most talented and diverse people.”
In Canada, many companies have come to realize the strategic importance of a diverse workforce and, much like Google, have initiated comprehensive diversity strategies. But developing and executing those strategies is no easy feat.
Financial institutions were among the first organizations to act on the long-term demographic and labour-market significance of Canada’s Employment Equity Act, which requires special measures and the accommodation of differences for four designated groups in Canada: women, aboriginal peoples, persons with disabilities and members of visible minorities.
“As a regulated organization, we looked at diversity from a compliance perspective at first,” said Norma Tombari, director of Global Diversity at the Royal Bank of Canada. “However, with the appointment of Gordon Nixon as CEO in 2001, came the revitalization of a very robust diversity strategy; what we refer to as our Diversity Blueprint.”
RBC has been recognized in recent years for its achievements in diversity and inclusion practices. Its 2013 Diversity and Inclusion Report shows RBC’s workforce is comprised of 64% women, 31% visible minorities, 4.6% people with disabilities and 1.5% aboriginal persons — numbers that are fairly representative of the general workforce in Canada.
So, how do companies reach this level?
“Education becomes key when you are managing a multicultural and multigenerational workforce,” Ms. Tombari said. “There will be unconscious bias and blindspots, as well as a lack of cultural understanding and awareness throughout all levels of the organization, so it is our job to put programs in place that counter those attitudes.”
RBC takes a multifaceted approach, offering employees various workshops and webcasts on raising cultural acumen, as well as access to self-assessment tools where employees can rate their own level of understanding.
“The goal is to provide learning that is focused on the topic of diversity and inclusion and the rest is about embedding it in the cultural landscape of an organization,” Ms. Tombari said.
Canada’s energy giant Suncor is at a different stage of the diversity and inclusion-implementation process. After merging with Petro-Canada in 2009, changes in corporate structure created a tidal wave of new systems and strategies.
“With so much change and turnover, some things — such as our diversity strategies — got pushed to the side,” said Kelli Stevens, a company spokeswoman.
The company’s 2012 diversity report shows Suncor’s workforce is comprised of 23% women, 11.1% visible minorities and 2.7% Aboriginal persons. “We don’t look at our current percentages and think that’s okay,” Ms. Stevens said. “We are, and always will be, trying to improve them.”
Suncor, similar to Google, faces the uphill battle of recruiting from a rather homogenous talent pool. “We are a male-dominated field,” Ms. Stevens said.
In 2011, women earned only 16.5% of degrees/diplomas categorized within the fields of architecture, engineering and related technologies, Statistics Canada data shows. In fields relating to mathematics, computer and information sciences, women earned only 27% of degrees/diplomas. However, out of those pursuing post-secondary education, women account for more than half at 58%.
Suncor is in the process of developing a strategy that makes those desires a reality. Part of that strategy is supporting various programs that work to broaden the talent pool.
In March 2013, the Suncor Energy Foundation approved a five-year, $1.5-million program aimed at helping Women Building Futures (WBF), an organization that specializes in encouraging and preparing women for careers in skilled trades, to refine its business model and expand its impact.
Suncor also provides funding for Actua, the Ottawa-based national science, technology engineering, and mathematics (STEM) program, to help develop and deliver STEM programs to Aboriginal youth across Canada.
“Many of the communities we have a strong presence in have a high representation of aboriginal people,” Ms. Stevens said. “We want to be reflective of where we work and build strong relationships with those communities.”
Echoed in both companies’ strategies is the hard fact that implementing a diversity strategy is not easy; it is a long-term commitment with results as well as challenges at all stages.
Susan Black, managing partner at Crossbar Group, and Keith Caver, North America practice leader for talent management and organizational alignment at Towers Watson, offer the following advice for corporations undergoing a significant change in workforce demographics:
Inclusion is about making the numbers count: “Companies tend to jump right into programs without clearly defining their goals,” Ms. Black said. “This is often the result of a disconnect in their understanding of their own issues. In an ideal world, having a 50/50 split between male and female employees would be considered success, however, companies really need to look at their corporate structure and their client base to determine if that is what is best for their organization.”
Don’t define diversity too narrowly: “Companies tend to frame all diversity efforts around the four groups and they end up leaving a lot of white space,” Ms. Black said. “As a result people get left out of the diversity conversation. We are all a part of diversity and the thoughts and opinions of everyone should be valued in an organization.”
Culture isn’t something you can change overnight: “It typically goes one of two ways,” she said. “Either organizations declare victory too soon or they fall prey to diversity fatigue. The fact is it takes a long time to change workplace cultures. Don’t rush the process.”
You must address cultural differences and unconscious bias: “It is not good enough to just have the people in place,” Mr. Caver said. “There is an array of information available about shifting demographics and leveraging human capital. There must be an unwavering commitment to educating and preparing leaders so companies are not held back by hidden biases.”
ESFP personality types are very compatible with many areas of nursing. As an ESFP, you’re full of energy and a zest for life. You genuinely enjoy being around people, and you are a true people-person. In fact, some people call your type the “parties,” as you always seem to be looking for a new social event to attend. When there, you can talk for hours and you enjoy being the center of attention. Other personality profiles refer to your type as the “Entertainer” or “Artisan.”
ESFP Overview: What is an ESFP Personality?
An ESFP is one of the main 16 personality types. An ESFP will have scored the following dominant characteristics on a personality assessment: Extroverted (E), Sensing (S), Feeling (F), and Perceiving (P). The breakdown and description of each of these dominant characteristics is listed below:
Extroverted (E): As an extrovert, you enjoy a lot of external stimulation. You love hanging with friends, meeting new people, or engaging in external things that stimulate your mind. When you’re isolated for too long at home, you’ll soon begin saying to yourself, “I’ve got to get out of this house!” In fact, you may say that after only one day alone at home!
You probably have a wide circle of friends, and you love getting together for a meal, hanging out, or just striking up a conversation with a random person. Because extroverts tend to enjoy talking and engaging in social situations, they often get labeled as “social butterflies.” You may have even been called a “people person” or “outgoing.” In fact, introverts sometimes get a bad rap due to extroverted people, as people often quip, “Why does that introvert keep to themselves so much? I wish they were more talkative and outgoing.”
You probably dislike writing or reading too much, and you’d much prefer to pick up the phone and make a call as opposed to writing an email. Some extroverts loath writing, although not all feel this way. Some extroverts make great writers, but most prefer face-to-face communication if given the choice. Some extroverts tend to have difficulty expressing their ideas in written form, as their minds are wired to work while engaging. ESFPs can spend a lot of time text messaging contacts, however, because they love to keep up with their friends and acquaintances.
Being an extrovert doesn’t mean that you dislike alone time, it’s just that it tends to suck the life out of you after a while. You get energized and feel most comfortable around other people, especially many friends or family members.
You think better while talking, as opposed to writing or thinking alone. In fact, some of your best solutions or ideas have probably come to you while talking to others. You also tend to blurt out the answer if asked a question. In contrast, introverts hate being put on the spot, and prefer to mull over a question before replying.
Sensing (S): As a sensing person, your mind tends to think of more rigid “here and now” concepts. You generally tend to think about the “what ifs” only rarely. You tend to notice minor details that other people may overlook. In fact, some people are quite shocked at the fact that you can sometimes make really keen observations. This can be a big benefit in nursing, as you may notice that a patient suddenly doesn’t look so well.
To illustrate how a sensing person things, consider an example of a large container sitting on the edge of a counter. You would probably look at the large container of fluid and think, “That’s an interesting color. I wonder what this fluid is?” You may also examine the lettering used for the logo, and so forth. You’d probably read the details on the packaging and think about those things.
This type of thinking is in direct contrast with people who have the “intuitive” characteristic. Using this same illustration, an intuitive person may look at the same container you looked at and think thoughts like, “That may fall down. Then it could make a mess. Someone could slip and fall and hurt themselves. We could even be sued.”
That’s not to say that sensing people can’t have moments of intuition, or that people with intuition won’t see more concrete details. But generally speaking, sensing people are very in-tune with details and facts, and tend to not think of the possible scenarios that could happen.
Feeling (F): As a person with the “feeling” characteristic, you have a strong inclination towards considering how things may affect people or society. When considering a decision, you tend to think of how other people may react, or how other people may be impacted by the consequences. As a result, people (or society in general) can be a big part of your decision making process. This can be a good characteristic to have as a nurse dealing with patients whose lives may be greatly affected by your actions.
Feelers have a very deep and empathetic heart to help people, and they genuinely care for others. If someone asks you how their new haircut looks, you’ll likely be very polite and try to focus on the positives to avoid hurting their feelings–even if the haircut looks terrible.
As a feeler, you also tend to have a strong need for happy relationships, both with yourself and people around you. If people aren’t getting along, it will tend bother you quite a bit. You’re a happy-go-lucky person who enjoys keeping in good standing with people. You also tend to have a natural affection for animals or pets.
This characteristic is in contrast to the “thinking” characteristic, in which people tend to make decisions based on logic, facts, or truth.
Perceiving (P): As a person with the “perceiving” characteristic, you generally like to live life in a care-free manner. You usually don’t like to make extensive plans, and you prefer to just “wing-it.” You tend to be very adaptable to any given situation. This adaptability and spontaneity gives you a reputation of being a fun and exciting person to hang around.
You are likely to live a somewhat disorganized life, at least internally. You probably have a relatively messy or unorganized home or office space, although this is not true for all ESFPs. This personality characteristic is in contrast to the “judging” type, in which people tend to live in a more organized and controlled manner.
You also tend to procrastinate with deadlines and tasks, but will get a burst of energy when something has to be done. Some ESFPs have a wild side, and are sometimes referred to as “daredevils.” You may enjoy activities such as skydiving, rollercoasters, surfing, or other similar activities that give you that “thrill.”
Nursing Career Possibilities for ESFPs
You are a fun and entertaining “people-person.” You like to live life in a fun-loving way. This can help you quickly and easily connect with patients. You also have the ability to focus on details, and you can easily empathize with other people’s problems. As you make decisions, you ponder how they may affect other people. This means you are likely to keep your patients best interests at heart.
For this reason, there are many areas of nursing that may appeal to you. Floor nursing, pediatric nursing, ER nursing, and other exciting areas may be of interest. For ESFPs who have a daredevil side, you may also enjoy flight nursing. Being a camp nurse is also a good possibility. If you have a strong faith, Parish Nursing may also be a good fit, as you’d love interacting with people on a spiritual level.
There are a few pitfalls you’ll want to avoid on the job. First, ESFPs tend to dislike having to do routine tasks. You like to be stimulated in your environment, and if you have to do dull tasks, you’ll get bored quickly. You also dislike having to read long documents or write reports.
Another area of frustration for ESFPs is working alone. You enjoy the company of people, and if confined to an empty office all day, you’d probably get very exhausted. You get energized talking and engaging with people. You enjoy team settings.
You dislike organizing things due to your spontaneous nature. You like to experience things in real time, and you don’t like to ponder the “what-ifs” in life. You also may struggle clocking in on time.
Possible Nursing Career Matches for ESFPs
Home Nursing/Private Duty Nursing
ER Nurse
Parish Nurse
Hospice Nurse
Travel Nurse
General Floor Nurse
Ambulatory Nurse
Pediatric Nurse
Flight Nurse
Camp Nurse
Oncology Nurse
Are You an ESFP? Share Your Input
What areas do you hope to work as an ESFP? What jobs have you loved? What jobs have you hated? Please consider sharing your experience in the comment section below, as this may help other ESFP nurses in their careers.
When Joanne Clavelle was 12 years old, she began working as a candy striper at a Vermont hospital.
It didn't take her long to realize that she had found what she was meant to do.
"I used to feed patients, change their water pitchers and make eggnog with real eggs," Clavelle says. "After a couple of years of being a candy striper, the nurses at the hospital sort of adopted me, and I moved into a volunteer aide position in the emergency department. I got to wear a white uniform with white stockings and shoes; I thought I was in heaven."
Clavelle was hired as an EKG technician at the same hospital when she was 16. She worked every weekend doing what she loved.
Her dedication to outstanding patient care caught the eye of three physicians at the hospital.
"The doctors had a scholarship program," Clavelle says. "They gave me a scholarship, which helped pay for me to go to nursing school at the University of Vermont.
Thirty-plus years later, Clavelle is still as passionate as ever about her career as a nurse and providing top-notch patient care. Five months ago, she was named senior vice president and chief clinical officer at Scottsdale Healthcare.
"I absolutely love my job here," she says. "I have the opportunity to create a nursing infrastructure that focuses on outstanding patient care and ensures that we maintain our Magnet designation."
This designation, Clavelle says, is given to the top 8 percent of hospitals in the country.
"It recognizes organizations like ours that create a supportive environment for nurses to practice and provide high-quality care," she says. "I am committed to creating a culture where nurses and other providers give the best care possible. That's what it's really all about."
When she is not working, Clavelle enjoys painting.
Watercolors are especially appealing to her, and she takes art classes whenever she can.
Clavelle also likes to spend time with her husband, their adult children and their 14-year-old dog.
Even though Clavelle has spent the past 36 years working in health care, she says things amaze her — in a good way — about her work.
"I was pleasantly surprised and proud to learn that our hospital has a forensic-nursing program, and we also have a wonderful military partnership with the United States Air Force," she says. "It's a unique model for graduate nurses in the Air Force to participate in a number of programs, including a nurse-transition program and critical-care and emergency-trauma-nursing fellowship."
Who's Who in Business 2014
Joanne Clavelle is one of 50 women in various fields profiled in "Who's Who in Business 2014," a publication of Republic Media. Find the full publication online at azcentral.com in July.
Ah, the dreaded night shift. Every nurse will have to encounter it at some point in his or her career. Some enjoy the more patient-based shift with its lack of administrators and clerical work, while others never can get into the rhythm of being a night owl.
If you’re a nurse on the night shift, chances are you have plenty of non-medical professional friends who won’t keep the same schedule as you. So how do you keep a normal social life while you work the night shift? Check out these five helpful tips:
1. Plan ahead with your non-work friends. If your shift is starting at 7:00 PM, for example, you could realistically have time to meet them for dinner an hour or so ahead of time. The night shift might remove some of the spontaneity of your social life, but it doesn’t have to remove time for fun and socializing.
2. Limit your caffeine intake. It can be tempting to consume cup after cup of coffee to get through those long shifts, but it’ll throw your sleep rhythm off even more and cause you to have to miss out on social functions with friends and family during days off.
3. Treat the switch to normal sleeping hours like jet lag. Take short naps at first to store up some energy and then power through the day until it’s time for bed. This will quicken your transition back to a normal sleep schedule. Try making time for non-work friends the day after you’ve adjusted back to normal sleeping hours.
4. Group your night shift days together. This will assure that you can have longer stretches of days off or daytime shifts. That leaves plenty of time for recreation, fun with friends, errands and time with family, but it’s also better for your overall health!
5. Get to know your coworkers! You’re spending so much time with them at odd hours, so you might as well establish trust, rapport and friendship. Try and bond with them socially and professionally. For example, if you like exercising, invite them to go on an early morning hike or to a workout class with you after the shift ends; if you are a coffee nut, see if they want to grab a cup at a nearby café. You can also bond professionally by trying to coordinate procedural training, or going to conferences and professional development events together.
The night shift doesn’t need to kill your mood, routine or health. Treat it seriously, plan accordingly with your shifts and keep a positive outlook so you can make new friends and keep up with those outside of your professional circle!
DETROIT — Technology originally designed for the U.S. military now has a second use: helping those with tremors eat and live better.
A high-tech spoon — fitted with a tiny computer and sensors such as those in a camera or cellphone — softens the effect of essential tremors by sensing their direction and strength and moving the device in the opposite direction.
"In some ways, it seems too simple to be true," said Dr. Kelvin Chou, a University of Michigan neurologist and essential tremors specialist whose patients helped test the device.
For essential tremor patients, simple daily activities — eating, applying makeup — can be impossible.
"Not being able to feed yourself or groom yourself — that takes a big emotional toll," said Anupam Pathak, CEO of Lift Labs, a California-based start-up company that makes the device.
The idea ignited after Pathak began as a doctorate student in engineering at the University of Michigan. He had been working on research to help stabilize military equipment for U.S. soldiers in the middle of combat, and over time, he began wondering whether the technology could help those whose hands tremble.
With funding from the National Institutes of Health, Pathak developed the LiftWare, a device that assesses movements thousands of times in a single second.
To test it, he turned to the university, where doctors at the U-M Health System treat 400 to 500 patients a year for hand shakes caused by essential tremor, a common movement disorder. It is estimated that 1 in 20 people worldwide have a degree of essential tremor.
Chou said the spoon worked surprisingly well for the 15 adults who tested it.
All had moderate essential tremor.
He said the results were "amazing," especially considering how socially limiting essential tremors can be. Patients often stop eating in front of others and no longer go out with friends and loved ones.
In the worst cases, they cannot feed themselves at all. Just 10% are candidates for surgery that treats the tremors.
"One of the worst things about essential tremor is that people feel like they have to be alone. This changes things for people," Chou said.
The device may not work for everyone with tremors. With many patients with Parkinson's disease, for example, the tremor improves when they are performing a task such as eating. However, those whose tremors interfere with eating stand to benefit from the device, Chou said.
The spoon and its advanced microelectronic technologies come with a hefty price tag: $295. Lift Labs and the International Essential Tremor Foundation have established a campaign to give the spoons to those with limited income.
Chou and Pathak said the same technology could be fitted with pieces to help those with tremors execute other daily activities, such as applying makeup or using hand tools. A fork and a soup spoon attachment will be available in the coming months, Pathak said.
Today's expectant moms and their doctors have decided it's not nice to fool Mother Nature. Rather than inducing labor, they're letting nature take its course, with the length of pregnancies in the U.S. on the upswing, according to a new study by the CDC.
The study released Wednesday tracks labor started through surgical or medical means during the years 2006 through 2012. The researchers found that induction rates at 38 weeks — once considered full-term gestation but now called an early-term gestation — declined for 36 states and the District of Columbia during this six-year period. Declines ranged from 5 percent to 48 percent.
Geography didn’t seem to matter. Thirty-one states and the District of Columbia posted declines of at least 10 percent. The researchers did find that trends in induction rates at each week from 35 weeks, considered late pre-term, to 38 weeks, varied by maternal age. At 38 weeks, though, induction rates declined for all maternal age groups under 40, dropping 13 percent to 19 percent for women in their 20s and 30s.
This is a sharp reversal of trends tracked from 1981 through 2006 in which the proportion of babies born at less than 39 weeks gestation increased nearly 60 percent, while births at 39 weeks or more declined more than 20 percent.
“We were surprised that the overall induction rate went down,” says lead researcher Michelle Osterman, a health statistician with the National Center for Health Statistics, which is part of the CDC.
And it is welcome news, too. “For years we were taught that the 37th or 38th week of pregnancy was full term, but we did not appreciate the neonatal outcomes,” says ob/gyn Dr. Nancy Cossler, vice chair for quality and patient safety at University MacDonald Women’s Hospital in Cleveland, Ohio.
“It was an ingrained part of our culture that 37 weeks is OK, but it’s not necessarily OK for the baby,” she says, citing issues such as hypothermia, feeding difficulties and respiratory distress among infants born early.
Historically, MacDonald Women’s Hospital had a rate of about 11 percent for labor induction for non-medical reasons among patients who were 37 to 38 weeks pregnant. Today, it’s nearly zero. In 2013, only one birth among the 37 to 38 week gestational age was done through induction. The patient had metastatic breast cancer, which is not among the usual listed criteria for medical induction, and needed to start chemotherapy and needed an early delivery, says Cossler.
Indeed, there is a big push nationally for longer-term births, such as the large-scale educational program called the 39-Week Initiative, supported by the March of Dimes and other groups. It seeks to end non-medically indicated deliveries prior to 39 weeks. Last year, the American Congress of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine even recommended the label “term” in pregnancy, be replaced with categories based on gestational age. Today, babies born at 39 weeks through 40 weeks and six days of pregnancy are considered “full term.” Babies born at 37 to 38 weeks are now considered “early term.”
“I think this study is very positive since several of us have now provided evidence that babies have better outcomes (with longer term births),” says Dr. Kimberly Noble, assistant professor of pediatrics at Columbia University.
In a study published in the journal Pediatrics of 128,000 New York City public school children, Noble and her colleagues found that compared to children born at 41 weeks, those born at 37 weeks had a 33 percent increased chance of having third-grade reading problems, and a 19 percent increased chance of having moderate math issues.
But doctors do worry that the pendulum could swing too far and patients may be afraid of induced deliveries.
Our study “can’t differentiate between induction done for medical reasons and induction done for convenience, and if your doctor says this baby needs to come out at 37 weeks because of a problem, you need to trust your doctor,” says Noble, citing issues such as maternal or fetal distress as a cause for earlier delivery. What patients and doctors shouldn’t do is schedule an earlier delivery because of a vacation or other issue. “We know that 39 weeks and beyond is good for the baby,” she says.
SAN FRANCISCO, USA - For decades, medical technology firms have searched for ways to let diabetics check blood sugar easily, with scant success. Now, the world's largest mobile technology firms are getting in on the act.
Apple Inc, Samsung Electronics Co and Google Inc, searching for applications that could turn nascent wearable technology like smartwatches and bracelets from curiosities into must-have items, have all set their sites on monitoring blood sugar, several people familiar with the plans say. These firms are variously hiring medical scientists and engineers, asking U.S. regulators about oversight and developing glucose-measuring features in future wearable devices, the sources said. The first round of technology may be limited, but eventually the companies could compete in a global blood-sugar tracking market worth over $12 billion by 2017, according to research firm GlobalData. Diabetes afflicts 29 million Americans and costs the economy some $245 billion in 2012, a 41 percent rise in five years. Many diabetics prick their fingers as much as 10 times daily in order to check levels of a type of sugar called glucose. Non-invasive technology could take many forms. Electricity or ultrasound could pull glucose through the skin for measurement, for instance, or a light could be shined through the skin so that a spectroscope could measure for indications of glucose. "All the biggies want glucose on their phone," said John Smith, former chief scientific officer of Johnson & Johnson's LifeScan, which makes blood glucose monitoring supplies. "Get it right, and there's an enormous payoff." Apple, Google and Samsung declined to comment, but Courtney Lias, director at the U.S. Food and Drug Administration's chemistry and toxicology devices division, told Reuters a marriage between mobile devices and glucose-sensing is "made in heaven." In a December meeting with Apple executives, the FDA described how it may regulate a glucometer that measures blood sugar, according to an FDA summary of the discussion. Such a device could avoid regulation if used for nutrition, but if marketed to diabetics, it likely would be regulated as a medical device, according to the summary, first reported by the Apple Toolbox blog. The tech companies are likely to start off focusing on non-medical applications, such as fitness and education. Even an educational device would need a breakthrough from current technology, though, and some in the medical industry say the tech firms, new to the medical world, don't understand the core challenges. "There is a cemetery full of efforts" to measure glucose in a non-invasive way, said DexCom chief executive Terrance Gregg, whose firm is known for minimally invasive techniques. To succeed would require "several hundred million dollars or even a billion dollars," he said.
POACHING
Silicon Valley is already opening its vast wallet.
Medtronic Inc Senior Vice President of Medicine and Technology Stephen Oesterle recently said he now considers Google to be the medical device firm's next great rival, thanks to its funding for research and development, or R&D.
"We spend $1.5 billion a year on R&D at Medtronic - and it's mostly D," he told the audience at a recent conference. "Google is spending $8 billion a year on R&D and, as far as I can tell, it's mostly R."
Google has been public about some of its plans: it has developed a "smart" contact lens that measures glucose. In a blog post detailing plans for its smart contact lens, Google described an LED system that could warn of high or low blood sugar by flashing tiny lights. It has recently said it is looking for partners to bring the lens to market.
The device, which uses tiny chips and sensors that resemble bits of glitter to measure glucose levels in tears, is expected to be years away from commercial development, and skeptics wonder if it will ever be ready.
Previous attempts at accurate non-invasive measurement have been foiled by body movement, and fluctuations in hydration and temperature. Tears also have lower concentrations of glucose, which are harder to track.
But the Life Sciences team in charge of the lens and other related research is housed at the Google X facility, where it works on major breakthroughs such as the self-driving car, a former employee who requested anonymity said.
Apple's efforts center on its iWatch, which is on track to ship in October, three sources at leading supply chain firms told Reuters. It is not clear whether the initial release will incorporate glucose-tracking sensors.
Still, Apple has poached executives and bio-sensor engineers from such medical technology firms as Masimo Corp, Vital Connect, and the now-defunct glucose monitoring startup C8 Medisensors.
"It has scooped up many of the most talented people with glucose-sensing expertise," said George Palikaras, CEO of Mediwise, a startup that hopes to measure blood sugar levels beneath the skin's surface by transmitting radio waves through a section of the human body.
The tech companies are also drawing mainstream interest to the field, he said. "When Google announced its smart contact lens, that was one of the best days of my career. We started getting a ton of emails," Palikaras said.
Samsung was among the first tech companies to produce a smartwatch, which failed to catch on widely. It since has introduced a platform for mobile health, called Simband, which could be used on smart wrist bands and other mobile devices.
Samsung is looking for partners and will allow developers to try out different sensors and software. One Samsung employee, who declined to be named, said the company expects to foster noninvasive glucose monitoring.
Sources said Samsung is working with startups to implement a "traffic light" system in future Galaxy Gear smartwatches that flashes blood-sugar warnings.
Samsung Ventures has made a number of investments in the field, including in Glooko, a startup that helps physicians access their patients' glucose readings, and in an Israeli glucose monitoring startup through its $50 million Digital Health Fund.
Ted Driscoll, a health investor with Claremont Creek Ventures, told Reuters he's heard pitches from potentially promising glucose monitoring startups, over a dozen in recent memory.
Software developers say they hope to incorporate blood glucose data into health apps, which is of particular interest to athletes and health-conscious users.
"We're paying close attention to research around how sugar impacts weight loss," said Mike Lee, cofounder of MyFitnessPal.
After decades of false starts, many medical scientists are confident about a breakthrough on glucose monitoring. Processing power allows quick testing of complex ideas, and the miniaturization of sensors, the low cost of electronics, and the rapid proliferation of mobile devices have given rise to new opportunities.
One optimist is Jay Subhash, a recently-departed senior product manager for Samsung Electronics. "I wouldn't be at all surprised to see it one of these days," he said. — Reuters
In a case weighing the government’s ability to require vaccination against the individual right to refuse it, a federal judge has upheld a New York City policy that bars unimmunized children from public school when another student has a vaccine-preventable disease.
Citing a 109-year-old Supreme Court ruling that gives states broad power in public health matters, Judge William F. Kuntz II of Federal District Court in Brooklyn ruled against three families who claimed that their right to free exercise of religion was violated when their children were kept from school, sometimes for a month at a time, because of the city’s immunization policies.
The Supreme Court, Judge Kuntz wrote in his ruling, has “strongly suggested that religious objectors are not constitutionally exempt from vaccinations.”
The lawyer for the plaintiffs, Patricia Finn, said she plans to appeal the decision, announced this month. On Thursday, Ms. Finn asked the district court to rehear the case.
Amid concerns by public health officials that some diseases are experiencing a resurgence in areas with low vaccination rates, the decision reinforces efforts by the city to balance a strict vaccine mandate with limited exemptions for objectors. Pockets of vaccination refusal persist in the city, despite high levels of vaccination overall.
State law requires children to receive vaccinations before attending school, unless a parent can show religious reservations or a doctor can attest that vaccines will harm the child. Under state law, parents claiming religious exemptions do not have to prove their faith opposes vaccines, but they must provide a written explanation of a “genuine and sincere” religious objection, which school officials can accept or reject.
Some states also let parents claim a philosophical exemption, though New York does not. Some parents refuse to have their children vaccinated because of a belief that vaccines can cause autism, though no link has ever been proved.
Two of the families in the lawsuit who had received religious exemptions challenged the city’s policy on barring their children, saying it amounted to a violation of their First Amendment right to religious freedom and their 14th Amendment right to equal protection under the law, among other claims. Their children had been kept from school when other students had chickenpox, their suit said.
The third plaintiff, Dina Check, sued on somewhat different grounds, saying that the city had improperly denied her 7-year-old daughter a religious exemption. She said the city rejected her religious exemption after it had denied her a medical exemption, sowing doubts among administrators about the authenticity of her religious opposition. But Ms. Check said the request for a medical exemption had been mistakenly submitted by a school nurse without her consent.
After the school barred her daughter, Ms. Check home-schooled her and then moved her to a private school that accepted her daughter without the vaccinations. State vaccination requirements cover public and private schools, but in New York City, private schools have more autonomy in handling exemptions.
Ms. Check said she rejected vaccination after her daughter was “intoxicated” by a few shots during infancy, which she said caused an onslaught of food and milk allergies, rashes and infections. Combined with a religious revelation she had during the difficult pregnancy, she said, the experience turned her away from medicine. Now she uses holistic treatments.
“Disease is pestilence,” Ms. Check said, “and pestilence is from the devil. The devil is germs and disease, which is cancer and any of those things that can take you down. But if you trust in the Lord, these things cannot come near you.”
In turning down all three families, Judge Kuntz cited a 1905 Supreme Court ruling that upheld a $5 fine for a Massachusetts man who disobeyed an order to be vaccinated during a smallpox outbreak, a case that helped establish the government’s right to require immunizations as a matter of public health.
Ms. Finn, the families’ lawyer, said that case should not be relevant. “There’s no way that court anticipated that children would be subjected” to the vaccines they must get today, she said.
In New York, the statewide mean religious exemption rate rose over the last decade, from .23 percent in 2000 to .45 percent in 2011, a 2013 study in the medical journal Pediatrics said.
New York City schools granted 3,535 religious exemptions in 2012-13, according to data from the state’s Health Department. Though city schools, public and private, have an overall immunization rate around 97 percent, according to the department, 37 private schools were below 70 percent. Health experts believe that above a certain immunization rate, outbreaks are limited because a disease cannot spread to enough people during its incubation period to sustain itself, a phenomenon known as “herd immunity.” For measles, which is highly contagious, that rate is believed to be 95 percent, according to Daniel Salmon, deputy director at the Institute for Vaccine Safety at the Johns Hopkins Bloomberg School of Public Health.
Though widespread vaccinations have practically eliminated diseases like measles and mumps from the United States, flare-ups have occurred. The 477 measles cases reported this year represent the worst year-to-date count since 1994, according to the Centers for Disease Control and Prevention.
Among the 25 people who contracted measles in New York City between February and April this year, two were school-age children unvaccinated because of parental refusal. When one of the children, who was being home-schooled, contracted the measles, city health officials barred that child’s sibling, who had a religious exemption, from attending school. The sibling eventually contracted measles as well. Health officials credited the decision to keep the second child out of school with stopping the spread of disease in that community.
Ohio, which granted more than three times as many religious and philosophical exemptions to kindergarten students last year as it did in 2000, is struggling to contain a measles outbreak that has recently spread to 339 Amish people who were largely unvaccinated, the state health department said.
Mr. Salmon said it can be difficult for states to balance an obligation to mandate vaccination with some leniency for families who have strong objections. Rules that force parents to articulate their beliefs and require public officials to educate them about the risks of exemption are states’ best defense against the spread of disease, he said.
Still, especially because parents who refuse vaccination tend to cluster geographically, it takes only a few unvaccinated children to start an outbreak, he said. At that point, even vaccinated children are at risk.
“Diseases have a way of finding our vulnerabilities,” Mr. Salmon said, “the kinks in our armor.”
We want to know what you think. Agree or disagree?
This fall, Duquesne University in Pittsburgh will become the first academic institution in the U.S. and globally to offer a dual degree in nursing and biomedical engineering for undergraduate students, according to a news release.
“Duquesne has pioneered the integration of clinical knowledge and patient care with engineering techniques in a single program, creating the first bachelor’s degree of its kind,” Provost Timothy Austin, PhD, said in the release.
The five-year program will provide students with a foundational body of knowledge that keeps patient care and practical application at the core of studies supporting innovations and technological advances.
The joint degree could prove a tremendous value to employers and patients, said John Viator, PhD, director of Duquesne’s biomedical engineering program.
By gaining actual clinical experience, students also will develop new perspectives with respect to a patient’s health and functional needs. “Engineers do not always fully appreciate the hospital culture and the clinical needs of patients,” Mary Ellen Glasgow, RN, PhD, FAAN, dean and professor of the School of Nursing, said in the release. “This dual degree gives our students both the engineering and nursing perspectives to solve real world clinical problems.”
In addition to learning engineering and nursing, students will benefit from class and clinical experiences that incorporate the Toyota Production System principles (used to address safety, cost and efficiency) and the American Association of Critical Care Nurses’ Synergy Model.
Job opportunities for biomedical engineers are expected to grow 27% between 2012 and 2022, and nursing careers are expected to expand by 19% in the same timeframe, according to statistics from the Bureau of Labor Statistics. With the combined knowledge and skills of the two disciplines, opportunities may be limitless for the “nurse engineer,” Viator and Glasgow predict.
“Our students will begin their careers with the preparation, knowledge and worldview usually seen in those with years of experience in the field,” Austin said in the release. “This exciting BME/BSN partnership illustrates Duquesne’s innovative academic programs and the university’s focus on preparing students with the knowledge and skills to serve others.”
A research effort underway at an area nursing home is testing out telehealth robots and other technology to enhance a patient’s ability to remain independent longer.
Students and faculty from the University of Cincinnati’s College of Nursing, as well as students from the colleges of medicine, engineering and allied health sciences, have partnered with Maple Knoll Village to develop innovative models using technology to help older adults stay independent and in their homes longer, said Tim McGowan, vice president of operations at Maple Knoll.
“The quicker we can develop the technology necessary to safely monitor them at home, the lower the cost of care will be and the quality of life for the patient returning home will improve,” McGowan said.
Every month more than a quarter-million Americans turn age 65. By 2015, for the first time in U.S. history, people age 65 and older will outnumber children under age five, according to the Council on Aging of Southwestern Ohio.
The partnership has opened a “smart house” on the Maple Knoll campus, formally called the Innovation Collaboratory House, inside an independent living unit for the UC students to conduct research and pilot new technologies.
Debi Sampsel, chief officer of innovation and entrepreneurship at UC, said the partnership developed in October 2012, and the smart house opened last spring for senior capstone classes in nursing and engineering.
Now hundreds of students are using the facility for education, research and translational practice.
“The house is about preparing them to come out into the community and hone in on their skills and techniques they’ll need in real positions,” Sampsel said. “We can start mirroring real life because they have to start thinking on their feet.”
A number of student-led projects are underway at the house, including the ability to control the temperature and lighting from a remote location, and motion detectors used to track patterns of activity in daily living to detect when an unexpected change in habit has occurred, said Megan Gresham, spokeswoman for Maple Knoll.
“Staff or family can be alerted if say they’re not getting out of bed at a certain time,” Gresham said.
Sampsel said students are also training on human simulators — with speech and movements controlled by a teacher in the next room — to learn the proper ways to take an IV, bathe a patient, take blood pressure and listen to the heart and lungs.
“This fits into our strategic plan to creatively leverage technology to change health care,” said Greer Glazer, dean of UC’s College of nursing.
After a public open house June 26, the UC students will start working with physicians on geriatric rounds at Maple Knoll. A large telehealth robot, called “Flo Bot,” will go along on the rounds and nurse practitioner students and college of medicine fellows will access the data remotely from UC.
A smaller telehealth system coined “Little Bot” will be used by students making rounds inside the independent living units of resident who have volunteered.
“I’m most appreciative for the resident support at Maple Knoll,” Sampsel said. “It really brings home what their (the students’) health care profession is going to be all about.”
Sampsel said the two entities are developing a formal agreement to be reached this summer.
Kevin Cischke left a music career after 25 years to pursue a new one in nursing, and it won’t bother him that he’ll be a man in a profession largely dominated by women.
As the face of the nursing profession slowly changes, Mr. Cischke, 45, is among the growing number of men signing up for the job. According to the U.S. Census Bureau, slightly less than 10 percent of the 3.5 million nurses in 2011 were men. That’s up from 1970, when only 2.7 percent of nurses were males.
For Mr. Cischke – who will receive a bachelor’s in nursing next year from Mercy College — nursing is in line with his interests. When introduced to nursing, the former organist and choir master for the Archdiocese of Detroit fell in love with it.
“A couple of my close friends who are nurses said I should look into this profession to see if it would interest me,” he said, during a break from his externship in the emergency room at Mercy St. Vincent Medical Center. “It was a whirlwind love affair that has not ended, and I don’t suspect that it will.”
Craig Albers, chief nursing officer and vice president of patient care services at Mercy St. Charles Hospital, said men in nursing offer an important component in the delivery of public health care.
“In the past, nursing was more of a pink collar profession and more of a career for women. A lot of times it’s seen as a profession for Caucasian women. Now, with large numbers of baby boomers retiring and seeking health care, we need a diverse workforce able to work with a diverse population,” said Mr. Albers.
A nurse himself since 1998, he began his college studies pharmacy. When he decided he needed more patient interaction, a professor suggested he look into nursing.
“I job shadowed an ICU nurse and the role really appealed to me. That’s what led me to the profession,” he said.
While also acknowledging the importance of racial diversity, Mr. Albers added, “Each of those different minorities bring a special perspective and skill set in how they work with and relate to patients.”
It was the patients who also attracted Mr. Cischke.
"I enjoy the patient-care side of things. I wanted hands-on patient care. That's what drives me, and the fact that I can continue to learn and grow fits my personality perfectly," he said.
He also liked contributing to the profession and addressing concerns of his male peers. In fact, when they discovered something missing in their nursing school experience, he led the way to establishing a local chapter of the American Assembly of Men in Nursing. The organization addresses issues that affect men in nursing. About 20 men and five women are members of the group.
"I continued to explore what the assembly had to offer, promote, and to accomplish and I realized that their goals aligned with what we needed to have at Mercy to support our male students," said Mr. Cishke, one of 116 male students in the nursing program.
The organization will also help groom male nurses for retiring baby boomers who increasingly use health care. Health professionals who deliver care to boomers must be on their toes.
"Our baby boomer population will be very informed and knowledgeable and Internet and computer savvy, and people going into the nursing profession will have to be extremely knowledgeable and confident and able to communicate with their patients because the patients are very knowledgeable," said Mr. Albers.
While male nurses' physical strength is also a plus for patient care, Mr. Albers said more men joining the field may pursue advanced fields in nursing, such as management, administration, business, and anesthetics. Those advanced career possibilities attracted Daniel Koehler to the profession.
"One of the great things about nursing is that once you are in it and have a job and have some experience after a few years, you can go into management, get a master's, or PhD," said Mr. Koehler, 32, who is in the nursing residency program at ProMedica Flower Hospital. "There are so many different avenues you can go into, so it was kind of a no-brainer that I picked this."
He received a bachelor's in nursing from Lourdes University in December. Eight years ago, he obtained a bachelor's in human biology from Michigan State University. He then worked in the restaurant and fitness businesses before going to nursing school.
He wasn't intimidated by the predominantly female profession, and in fact received positive responses from others.
"Most guys don't grow up thinking they want to be nurses," as many girls do, said Mr. Koehler, whose mother was a nurse in Germany. "With the guys I've met in the profession, I think less of that stigma now days."
Though slightly less than 10 percent of ProMedica's nurses are men and slightly more than 8 percent of the nurses in the Mercy health system are men, the idea that nursing is a woman's job stopped Roberta Pratte's father and grandfather, both medics in the military, from continuing in the profession. As a teenager, Ms. Pratte — a Mercy nursing professor — recalls hearing her grandfather speak fondly about nursing.
"Back then it wasn't something that men talked about or thought about. I sensed that they regretted that they were not allowed to follow their dream," said Ms. Pratte, an instructor at Mercy College. She has been a nurse for 33 years, and her mother was also a nurse.
Large numbers of nurses are expected to retire soon, adding to the already critical nursing shortage. That's why the profession is pushing to attract men and women into nursing. As a matter of fact, the American Assembly for Men in Nursing is campaigning to increase the number of male nurses by 20 percent by the year 2020, said Ms. Pratte. She also said the Institute of Medicine and the Centers for Disease Control and Prevention are reviewing how to fill nursing positions to ensure that the public gets proper care.
George Palo is 90. He's repeating himself quite a bit these days and he's just had to downsize to a retirement community. He really misses his late wife.
Soon, he will also miss his beloved dog, Max.
This last bit of news caused a roomful of nurse educators to moan a sad, sympathetic, "Ohhhh" at a meeting last week at the Independence Blue Cross building in Center City.
George is a fictional character, created along with two others to help nurses in training understand dementia and its traveling companions among the elderly: depression and delirium.
The nurses' emotional response to George's impending loss was a sign of the emotional power of narrative, which the National League for Nursing is harnessing to improve education about late-life medical problems. The group also is embracing a multimedia approach that includes the written word, audio recordings of the "patients" voiced by actors, simulations that include mannequins and live actors, and the latest addition: virtual animations of the patients and nurse avatars who make treatment decisions.
"Traditional-based teaching is really over for most of us," Elaine Tagliareni, the league's chief program officer, told the crowd of about 175 who had gathered for her group's Advancing Care Excellence for Seniors conference. The Independence Blue Cross Foundation is a sponsor. Using technology to improve care was a theme this year.
The nursing group wants to reach a new generation of students who are already accustomed to multimedia learning, may be taking classes online, and will work in a world where technology increasingly connects patients, doctors, and nurses who are not in the same room.
Medical and nursing schools have long used standardized patients: actors who portray certain medical conditions. Increasingly sophisticated mannequins have been playing a bigger role in medical education in recent years.
Drexel University's College of Nursing and Health Professions began using a virtual-patient program produced by Shadow Health last year. It is meant to reinforce classroom training. The University of Pennsylvania School of Nursing also is using a Shadow Health program to teach nurses how to take a health history and perform a physical exam.
Gregg Lipschik, director of life-support training and undergraduate curriculum at the Penn Medicine Clinical Simulation Center, said Penn sometimes uses a virtual program to review resuscitation techniques. It pairs computer simulation and mannequins to teach procedures such as bronchoscopies.
Lipschik said use of simulation had been growing since 1999, when an Institute of Medicine report recommended it to reduce medical errors and improve teamwork. "It's really boomed in the last few years," he said.
The nursing league began its Advancing Care program in 2009, Tagliareni said, because "care of older adults is not well integrated into nursing programs" even though 75 percent of the care nurses give is to people over 65. It's adding the new dementia cases to expand education on another neglected topic.
The patient profiles are purposely complicated - like real people - and they unfold over time in unpredictable ways. The death of George Palo's golden retriever is a calamity not only because George's grief adds to his thinking problems but because walking Max was a key way the man exercised and interacted with the outside world. The profiles are accompanied by teacher information.
Tagliareni said that the dementia patients may not end up in the virtual world but that other fictitious elderly characters like Millie Larsen and Red Yoder may be available this fall in the gamelike "vSim for Nursing" program developed by Wolters Kluwer Health of Philadelphia and Laerdal Medical.
An audience member said her students easily identified with the league's patients. "That's my Pop-Pop," one of them told her.
The group at the meeting saw a younger virtual patient named Stan and his virtual nurse, Dan. Stan had gone to the emergency room with stomach pain from a bowel obstruction. The student, who had access to test information and doctor's orders, had to use a menu of options to decide what Dan should say and do. The animation was primitive, but the decisions were complex. At the end of their 30-minute encounter, the student received a number score and a report on what had been done and should have been done.
Barbara McLaughlin, head of nursing at Community College of Philadelphia, did a pilot test of vSim, which costs $100 per student for two years of access, with her students last year. "They liked them [the scenarios] a lot because it gave them the opportunity to do the same experience over and over and correct their mistakes," she said.
Concerted effort is needed to reverse the ongoing rise in pertussis cases and deaths, especially among children and young people, according to the article in the Journal of Christian Nursing by Emily Peake, APRN, MSN, FNP-C, CLC, and Lisa K. McGuire, MSN, MBA-HCM, RN. "This effort begins with nurses and nurse practitioners and other primary care providers who educate patients and the public," they write. "The battle of pertussis is winnable through education, awareness, and vaccination."
Caused by infection with Bordetella pertussis bacteria, pertussis has been increasing in recent years. In the United States, average annual pertussis cases increased from less than 3,000 cases per year during the 1980s to 48,000 in 2012, including 20 deaths. Worldwide, there are an estimated 50 million cases of pertussis and 300,000 deaths. Pertussis is a major cause of death in infants worldwide.
Why is pertussis on the rise? "Ambivalence toward precautionary childhood vaccinations" is a key reason, along with the lack of well-child visits and appropriate boosters. The arrival of non-vaccinated immigrants may also be linked to new clusters of pertussis outbreaks, according to Peake and McGuire. They write, "Nurses should educate patients and the public that follow-up booster vaccinations at all ages are critical to maintain immunity to pertussis and other vaccine-preventable diseases."
Issues including vaccine availability and cost, literacy and language barriers, and lack of information all contribute to the lack of recommended vaccinations. Fear of vaccination and religious objections also play a role. Most states allow exemptions from vaccination based on religious reasons, and there's evidence that even non-religious parents are using these exemptions to avoid vaccinating their children.
Nurses should reassure parents that that recommended vaccines are safe. Current diphtheria-tetanus-pertussis vaccines do not contain the mercury-containing preservative thimerosal. Adverse events occur in only a small fraction of vaccinated children, and most of these are mild local reactions.
"Practitioners must build a trusting relationship with patients and reinforce the need for vaccinations through face-to-face contact, engaging parents to discuss concerns, and provide evidence-based research to guide recommendations and reassure patients of the safety of vaccines," Peake and McGuire write. Waiting rooms provide a good opportunity to present videos and other educational materials.
The World Health Organization is working to increase the percentage of infants who receive at least three doses of pertussis vaccine to 90 percent or higher, especially in developing countries. Closer to home, partnerships should be formed with service organizations, food banks, churches, hospitals and schools. "These groups can help identify those most likely not to be vaccinated and help them find free or low cost immunizations," the authors write. "Faith community nurses are in an ideal role to create and lead these partnerships."
Nurses can also advocate for policies aimed at making universal vaccinations available for adolescents and adults. Peake and McGuire conclude, "By using our resources and uniting, a global battle will be waged and won against pertussis and the children of tomorrow can breathe easier for a lifetime."
TRINITY, Fla. (AP) — Evan Wolin sat patiently in his slightly oversized cap and knee-length black gown, waiting his turn.
One by one, the teacher called his classmates to the stage. Then, finally, she read his name.
Evan burst from his seat, sped to the front and grabbed his diploma, a huge smile eclipsing his face. He thrust the paper into the air with an extra arm pump, as his mom, Jessica, tried not to cry while she captured it all on her phone.
He was so ready for kindergarten.
____
Nearly three years ago, when Evan first entered Longleaf Elementary's preschool program for children with developmental delays, few predicted that this day would come.
At 2 1/2 years old, he had barely begun walking, hadn't started talking and coped daily with many medical problems stemming from being born a micropreemie.
"On paper, his medical diagnosis had us thinking, 'Oh, my,' " recalled school speech pathologist Janice Whittaker.
Since he still sometimes used a feeding tube, some of the staff at Longleaf thought Evan might be better suited for a program at Cotee River Elementary, which had dedicated nurses on staff. But his mom, a special-education teacher, and dad, a school administrator, did not want their son in a medical unit.
"I knew developmentally I wanted him in the area school. I knew that he had more in him," Jessica Wolin said. "Although he wasn't speaking, although he wasn't eating, I knew he was very bright. . I always wanted him to be challenged."
Teacher Heather Goldstein, also a neighbor of the Wolins who remembered seeing Evan come home as an infant "with every tube connected to him," committed to making her classroom work for his needs.
"As soon as they told me, I went right online to research everything," she said. "I thought, if he is coming I want to make sure I have everything in place."
Before he arrived, Goldstein reorganized the furniture in her book- and toy-filled classroom to make it easier for Evan to navigate. She continued to learn about his medical demands and prepare for his academic requirements, communicating with his family to keep them informed on daily activities.
Jessica Wolin praised Goldstein's dedication, saying the teacher went above and beyond to make Evan feel at home in school and to help ensure his success. District special-education prekindergarten coordinator Kelli Boles never doubted it.
Goldstein, Boles said, exemplifies what the school district wants from its teachers in the program, which is federally funded and guaranteed to all eligible children with special needs ages 3 to 5. When other educators need training or classroom ideas, Boles sends them to Goldstein.
"She knows where the kids are, what they need to work on," Boles said. "She's the model of what I would like to see for all classrooms."
Goldstein's overriding philosophy is simple: Treat all kids like typical kids, set high expectations and then help them get there. She's taught her special-needs preschoolers to read and write that way, not to mention how to speak and socialize.
____
During a recent class day, Goldstein had Evan working with pattern blocks, where he would match colored plastic shapes to a design on a paper. She had him count yellow hexagons to figure out how many he needed to complete the pattern. Then she turned to another set of pieces.
"What do we call the blue?" she asked. "We used to call them diamonds, but now that you're going to kindergarten we have to call them ..."
"Rom," Evan said, looking up at Goldstein for affirmation.
"Rhombus," she said, completing the word.
"I love rhombus," Evan said cheerfully, placing them on the pattern and then sweeping them all away to start again. "I did it!"
"What do you get to do now?" Goldstein asked.
"Build a tower!" Evan shouted. He started to stack pieces, knock them down and repeat.
____
Goldstein refuses to take full credit for Evan's progress. Parents must participate actively, she said, and the child must be determined, too, in order for them all to find success.
That collaboration shone through for Evan, she said. "He amazes me every year."
His mom feels much the same.
When he was born at 24 weeks weighing 1.5 pounds, some people wondered whether he would even survive. She kept the faith through illnesses and surgeries for short-bowel syndrome, months in the hospital, feeding tubes, therapists.
Would he walk? Would he talk? Would he eat?
Now he races around at breakneck speed, bouncing from his pet hamster to his stash of toy cars, climbing on furniture and jabbering nonstop. He loves bacon and pancakes (and syrup and eggs), and though he's still small for his age, he loves to play with as much abandon as any 5-year-old.
In April, he was named Longleaf's pre-K student of the month.
Program coordinator Boles had nothing but good to say about Evan's progress, which includes his move to a traditional kindergarten class in the fall.
"He is like the poster child of why we do this, because early intervention works," she said, expressing hope that more families would enroll their eligible children in the classes.
Jessica Wolin, meanwhile, looks forward to Evan's next adventure. Sure, she's nervous about kindergarten, just like she was about so many other steps in her son's life.
But "he's done all those things. I want to be surprised by him. I want to see the next surprise."
School nurses today do a lot more than bandage skinned knees. They administer vaccines and medications, help diabetic students monitor their blood sugar, and prepare teachers to handle a student's seizure or asthma attack, among many other things.
"Chronic disease management is what school nurses spend most of their time doing," says Carolyn Duff, president of the National Association of School Nurses. "We do care for students in emergencies, but we spend more time planning to avoid emergencies."
And though school nurses see many students regularly, they don't always have the most up-to-date information about the students' health. School nurses must get permission from parents to communicate with a child's doctor. Once the doctor gives them a care plan for the child, they generally rely on the doctor and/or parents for updates and changes.
"When things change, we don't always get told in a timely manner," says Nina Fekaris, a school nurse in the Beaverton, Ore., school district. "It works, but it takes a lot of coordination."
At the same time, school-based health care is unfamiliar territory to many medical professionals, who operate in a health care universe largely separate from school clinics and other community-based medical services.
But schools and health care systems are trying to bridge that gap. In these projects, some funded by the Affordable Care Act, school health professionals gain access to students' electronic health records, specialists and other health system resources. The initiatives are up and running or on the drawing board in Delaware, Florida and Oregon, among other locations.
In Delaware, "lots of nurses expressed that they had difficulty communicating with providers" at Nemours Health System, which serves children around the state, according to Claudia Kane, program manager of the Student Health Collaboration at Nemours.
In 2011, Nemours got together with the Delaware School Nurses Association and the state Department of Education to develop a program that, with parental approval, gives school nurses read-only access to the electronic health records of more than 1,500 students who have complex medical conditions or special needs. That includes conditions such as diabetes, asthma, attention deficit hyperactivity disorder, seizure disorders or gastrointestinal problems.
Beth Mattey, a school nurse in Wilmington, says that now that she has access to the Nemours system, she can check the recent lab test results of a student who has diabetes. "It's helpful for me to monitor his [blood sugar levels] and work with him to make sure he's in better control," says Mattey, who is president-elect of the National Association of School Nurses.
When a student put a staple through his finger, Mattey was able to check to make sure he went to the doctor and got treatment. "Checking with him directly involves calling him out of class," she says.
Eventually, school nurses will be able to put information into the Nemours electronic records system as well, says Kane.
In the meantime, Nemours doctors, some of whom were initially skeptical about allowing school nurses access to health system medical records, are warming up to the arrangement. Kane says it encourages communication between physicians and school nurses, and eases the burden of routine tasks because Nemours doctors no longer have to fax over care plans or instructions to the school nurse every few months for students who are part of the program.
The Nemours Student Health Collaboration project is operating in all Delaware public school districts as well as half of charter schools and about one-third of private schools. Kane says Nemours plans to extend the program to school-based health centers next.
After six years of trying, scientists have discovered a way to genetically modify mosquitoes so they produce sperm that will only conceive male offspring.
Female mosquitoes are the ones who bite people and pass along malaria, so scientists think if they can significantly lower the number of female mosquitoes the rate of malaria will also go down. In their researchpublished in the journal Nature Communications, the researchers created a modified strain of mosquitoes that produced 95% male offspring.
When they introduced the strain to a five caged wild mosquito populations, the modified pests eradicated entire mosquito populations in four of them. There were too few females for the populations to survive. The researchers hope that this same scenario could happen in the wild, and malaria-carrying mosquitoes could die off.
Their findings are important because the scientists are the first to interfere in the sex ratios of mosquitoes, and their strategy could be successful in eliminating malaria, which remains a fatal disease in some sub-Saharan regions in Africa. Malaria prevention methods worldwide have brought down malaria mortality rates by 42%, but scientists are concerned over insecticide-resistant mosquitoes that pass along drug resistant malaria.
“The research is still in its early days, but I am really hopeful that this new approach could ultimately lead to a cheap and effective way to eliminate malaria from entire regions. Our goal is to enable people to live freely without the threat of this deadly disease,” said study author Roberto Galizi from the Department of Life Sciences at Imperial College London in a statement.
The parents of children with autism often have to cut back on or quit work, and once they reach adulthood, people on the autism spectrum have limited earning potential.
Those income losses, plus the price of services make autism one of the costliest disabilities – adding $2.4 million across the lifespan if the person has intellectual disabilities and $1.4 million if they don't, according to a new study published in the journal JAMA Pediatrics.
"We've known for a long time autism is expensive, but we've really never had data like this to show us the full magnitude of the issue," said Michael Rosanoff, associate director of public health research for the advocacy group Autism Speaks, which funded the research. "These are on top of the costs to care for a typically developing individual."
Jackie Marks knows the problem firsthand. The Staten Island, N.Y., mom has 13-year-old triplets, all on the spectrum and all with intellectual deficits.
Everything about their care costs more money, she says, from the diapers and wipes she still has to buy to the specially trained babysitters she has to hire every time she wants to go out. For karate classes, she has to pay for one-on-one lessons; the therapist helping with social skills costs $150 an hour per child.
"I enjoy my children immensely," Marks said. "I have a wonderful husband. That, at the end of the day makes it all worth it. But is it like a typical experience? No."
Marks quit her job with the state as a bank auditor to care for Tyler, Dylan, and Jacob. Her husband's job not only has to cover day-to-day needs, but he has to put away enough money to pay for both her and the boys after he retires. She hopes the boys will be able to work someday, but they'll never have the kind of earnings that will sustain them, she said, and will probably receive modest Social Security benefits once they turn 18.
Four things need to change to bring down the cost of autism for families and society, according to David Mandell, director of research for the Center for Mental Health Policy and Services at the University of Pennsylvania.
Adults on the spectrum need more job opportunities. There are many small success stories of individuals or small groups of people with autism who are employed, but "we need to be more creative about thinking about employment on a large scale," Mandell said.
Adult care must be improved so only people who really need expensive residential care get it, and everyone else can find support in their own community, he said. "I think in too many cases, these residential settings represent a failure of our society to provide community-based, cheaper options," he said. "More flexible, cheaper options would be a way to bring these costs down."
Families with autism need more opportunities to stay in the workplace. "Issues that face autism ultimately face all families," Mandell said. "If we had more family-friendly workplace policies, we might see substantial change in the way families were able to manage the work-life balance when they had children with (all kinds of) disabilities."
Society needs to take the long view, he said. Spending money diagnosing and helping young children on the spectrum will probably save money when they are older, by reducing disability and improving employability. "We often talk about the cost of care, and we don't spend much time talking about the cost of not caring," he said.
NUMBERS:
•Cost of supporting someone with an autism spectrum disorder plus intellectual disability: $2.4 million in the USA and 1.5 million pounds in the United Kingdom ($2.2 million in U.S. dollars)
•Cost of supporting someone with an autism spectrum disorder but no intellectual disability: $1.4 million in the USA and .92 million pounds in the United Kingdom ($1.4 million)
Another influenza season is in the books, and overall it caused less sickness and death than flu seasons in the recent past, according to a new report from the Centers for Disease Control and Prevention.
Between Sept. 29, 2013, and May 17, 2014, a total of 53,471 specimens sent to U.S. labs tested positive for a flu virus. Among them, 87% were influenza A viruses, and the most common of these were versions of the H1N1 virus that prompted the swine flu epidemic in 2009. The other 13% of the confirmed specimens were influenza B viruses.
The CDC findings, which were published Thursday in the Morbidity and Mortality Weekly Report, did not estimate a total number of flu deaths for the 2013-14 flu season. But based on records kept by doctors and hospitals, researchers concluded that flu activity in the last year resulted in “lower levels of outpatient illness and mortality” compared with years when the predominant strains were versions of the H3N2 virus.
At least 96 children died of the flu in the last year, laboratory tests confirmed. Those deaths were reported in 30 states, New York City and Chicago. In about half of these cases, the patients had at least one preexisting condition, such as a neurologic disorder or a pulmonary disease, that may have made them more vulnerable to the flu.
The most striking statistic in the report is the rate of hospitalization among people between the ages of 50 and 64. Over the course of the entire flu season, the cumulative hospitalization rate for these adults was 54.3 per 100,000 people. In the previous four years, that figure has been as low as 8.1 and it never topped 40.6.
The H1N1 and other A viruses were the predominant flu viruses through late March. Then influenza B viruses took over, with the region encompassing New York, New Jersey, Puerto Rico and the Virgin Islands particularly hard hit.
The report noted one human case of a H3N2 virus that was first spotted in pigs in 2010 and was identified in a dozen people the following year. The new case was a child from Iowa who had direct contact with pigs. The patient fully recovered, apparently without spreading it to relatives or anyone else, according to the CDC.
Lab tests show that last year’s flu vaccine was well-chosen. Fully 99.9% of the H1N1 samples tested were “antigenetically similar” to the flu strain used in the vaccine, as were 95.3% of the H3N2 samples tested. Some vaccines also protected against just one influenza B virus, which accounted for 73% of the B viruses that circulated last year. Of those, 99.7% were “antigenetically similar” to the strain in the flu vaccine. Other vaccines also protected against a second B virus, and those were a good match as well, according to the report.
The vaccine for the 2014-15 flu season will be based on the same four viruses, the CDC said.
PITTSBURGH — Trauma patients arriving at an emergency room here after sustaining a gunshot or knife wound may find themselves enrolled in a startling medical experiment.
Surgeons will drain their blood and replace it with freezing saltwater. Without heartbeat and brain activity, the patients will be clinically dead.
And then the surgeons will try to save their lives.
Researchers at the University of Pittsburgh Medical Center have begun a clinical trial that pushes the boundaries of conventional surgery — and, some say, medical ethics.
By inducing hypothermia and slowing metabolism in dying patients, doctors hope to buy valuable time in which to mend the victims’ wounds.
But scientists have never tried anything like this in humans, and the unconscious patients will not be able to consent to the procedure. Indeed, the medical center has been providing free bracelets to be worn by skittish citizens here who do not want to participate should they somehow wind up in the E.R.
“This is ‘Star Wars’ stuff,” said Dr. Thomas M. Scalea, a trauma specialist at the University of Maryland. “If you told people we would be doing this a few years ago, they’d tell you to stop smoking whatever you’re smoking, because you’ve clearly lost your mind.”
At normal body temperatures, surgeons have less than five minutes to restore blood flow before brain damage occurs.CreditUniversity of Pittsburgh Medical Center
Submerged in a frozen lake or stowed away in the wheel well of a jumbo jet at 38,000 feet, people can survive for hours with little or no oxygen if their bodies are kept cold. In the 1960s, surgeons in Siberia began putting babies in snow banks before heart surgery to improve their chances of survival.
Patients are routinely cooled before surgical procedures that involve stopping the heart. But so-called therapeutic hypothermia has never been tried in patients in which a penetrative wound has already occurred, and until now doctors have never tried to replace a patient’s blood entirely with cold saltwater.
In their trial, funded by the Department of Defense, doctors at the University of Pittsburgh Medical Center will be performing the procedure only on patients who arrive at the E.R. with “catastrophic penetrating trauma” and who have lost so much blood that they have gone into cardiac arrest.
At normal body temperatures, surgeons typically have less than five minutes to restore blood flow before brain damage occurs.
“In these situations, less than one in 10 survive,” said Dr. Samuel A. Tisherman, the lead researcher of the study. “We want to give people better odds.”
Dr. Tisherman and his team will insert a tube called a cannula into the patient’s aorta, flushing the circulatory system with a cold saline solution until body temperature falls to 50 degrees Fahrenheit. As the patient enters a sort of suspended animation, without vital signs, the surgeons will have perhaps one hour to repair the injuries before brain damage occurs.
After the operation, the team will use a heart-lung bypass machine with a heat exchanger to return blood to the patient. The blood will warm the body gradually, which should circumvent injuries that can happen when tissue is suddenly subjected to oxygen after a period of deprivation.
If the procedure works, the patient’s heart should resume beating when body temperature reaches 85 to 90 degrees. But regaining consciousness may take several hours or several days.
Dr. Tisherman and his colleagues plan to try the technique on 10 subjects, then review the data, consider changes in their approach, and enroll another 10. For every patient who has the operation, there will be a control subject for comparison.
The experiment officially began in April and the surgeons predict they will see about one qualifying patient a month.
It may take a couple of years to complete the study. Citing the preliminary nature of the research, Dr. Tisherman declined to say whether he and his colleagues had already operated on a patient.
Each time they do, they will be stepping into a scientific void. Ethicists say it’s reasonable to presume most people would want to undergo the experimental procedure when the alternative is almost certain death. But no one can be sure of the outcome.
“If this works, what they’ve done is suspended people when they are dead and then brought them back to life,” said Dr. Arthur L. Caplan, a medical ethicist at New York University. “There’s a grave risk that they won’t bring the person back to cognitive life but in a vegetative state.”
But researchers at a number of institutions say they have perfected the technique, known as Emergency Preservation and Resuscitation, or E.P.R., in experimental surgeries on hundreds of dogs and pigs over the last decade.
As many as 90 percent of the animals have survived in recent studies, most without discernible cognitive impairment — after the procedure, the dogs and pigs remembered old tricks and were able to learn new ones.
“From a scientific standpoint, we now know the nuts and bolts and that it works,” said Dr. Hasan B. Alam, chief of general surgery at the University of Michigan Medical Center, who has helped perfect the technique in pigs.
“It’s a little unsettling if you think of all the what ifs, but it’s the same every time you push into new frontiers,” he added. “You have to look at risk and balance it against benefits.”
Trauma accounts for more years of life lost than cancer and heart disease combined, and it is the leading cause of death in people up to age 44, according to the Centers for Disease Control and Prevention. Surgeons are eager for new techniques that would help better the odds in emergency situations. Black males are disproportionately victims of homicide, especially gun violence, and most of the patients likely to fit the study criteria in Pittsburgh are African-American males, according to officials at the medical center.
In order to obtain an exemption to federal informed consent rules, the hospital held two town hall meetings on the university campus, placed advertisements on buses, and made sure the news got in newspapers catering to minority readers.
Officials posted information about the study on a website,acutecareresearch.org, and conducted a phone survey in the neighborhoods most at risk for “involuntary enrollment” in the trial. Still, a taxi driver, grocery clerk and security guard — all African-American men approached at random — said they had never heard of the trial, though they work within a couple of miles of the hospital.
They also did not object. “I don’t have a problem with it, if it saves lives,” said Charles Miller, a 52-year-old security guard.
Just 14 people have so far requested “No E.P.R.” bracelets, according to the medical center.
Nearly a half-dozen trauma hospitals may join the trial and begin testing the hypothermia procedure on dying patients, including the University of Maryland Medical Center in Baltimore.
Dr. Scalea, who will head the effort there, said he hoped to receive final regulatory approval by the end of the year.
He recalled a recent stabbing victim who died on his operating table.
“He might have lived if we could have cooled him down,” Dr. Scalea said.
In the emergency department at Children's Medical Center in Dallas, pharmacists who specialize in emergency medicine review each medication to make sure it's the right one in the right dose.
It's part of the hospital's efforts to cut down on medication errors and dangerous drug interactions, which contribute to more than 7,000 deaths across the country each year.
Medication errors can be caused by something as simple as bad handwriting, confusion between drugs with similar names, poor packaging design or confusion between metric or other dosing units, according to the Food and Drug Administration. But they're often due to a combination of factors, which makes them harder to prevent.
At Children's in Dallas, there are 10 full-time emergency pharmacists, more than anywhere else in the country, and they are on call 24 hours a day. The pharmacists provide a vital safety net, according to Dr. Rustin Morse, chief quality officer and a pediatric ER physician.
"Every single order I put in," Morse says, "is reviewed in real time by a pharmacist in the emergency department prior to dispensing and administering the medication."
That may sound obvious, but Morse says doctors like him, are used to jotting down a type and quantity of drugs and moving on. If there's a problem, a pharmacist will hopefully catch it and get in touch later. But later won't work in the emergency room.
The extra review is particularly important at Children's because medication errors are three times more likely to occur with children than with adults. That's because kids are not "just little adults," says Dr. Brenda Darling, the clinical pharmacy manager for Children's Medical Center.
"They have completely different metabolic rates that you have to look at," Darling says, "so you have to know your patients."
On any given week, pharmacists at Children's review nearly 20,000 prescriptions and medication orders, looking at things like the child's weight, allergies, medications and health insurance.
There are also automatic reviews by an electronic medical record system designed to essentially "spell check" orders to prevent errors. You need both, says Dr. James Svenson, associate professor of emergency medicine at the University of Wisconsin, because the electronic medical record doesn't catch all errors.
Svenson co-authored a study in the Annals of Emergency Medicine that found that even with an electronic medical record, 25 percent of children's prescriptions had errors, as did 10 percent of adults'. Now his hospital also has a pharmacist in the emergency department 24 hours a day.
So why doesn't every hospital do this? The main reason, Svenson says, is money.
"If you're in a small ER, it's hard enough just to have adequate staffing for your patients in terms of nursing and techs, let alone to have a pharmacist sitting down. If the volume isn't there, it's hard to justify."
Hiring pharmacists is expensive, but Morse points to research showing prescription review can reduce the number of hospital readmissions, thereby saving money and lives.
"People do make mistakes," Morse says, and you need to make sure "a patient doesn't get a drug that could potentially stop them breathing because it's the wrong dose."
Want a healthy baby? You may want to roll her around in dirt.
For decades, parents have shielded infants from bacteria and other possible triggers for illness, allergies and asthma.
But a surprising new study suggests that exposure to cat dander, a wide variety of household bacteria — and even rodent and roach allergens — may help protect infants against future allergies and wheezing.
Interestingly, contact with bacteria and dander after age 1 was not protective — it actually increased the risk.
“It was the opposite of what we expected,” said Dr. Robert Wood, chief of the division of allergy and immunology at the Johns Hopkins Children’s Center and co-author of the study in the Journal of Allergy and Clinical Immunology. “We’re not promoting bringing rodents and cockroaches into the home, but this data does suggest that being too clean may not be good.”
The new findings may help explain some contradictions in research on the so-called hygiene hypothesis, which suggested that kids growing up in a super clean environment were more likely to develop allergies.
“This doesn't completely resolve the controversy, but it does add a big piece of the puzzle,” said Dr. Jonathan Spergel, a professor of pediatrics and chief of allergy at the Children’s Hospital of Philadelphia.
The hygiene hypothesis was developed after researchers noticed that farm kids were less likely to have allergies. Dirty environments, experts suggested, might be protective. The hypothesis seemed to explain why developed countries had skyrocketing rates of allergies and asthma.
“We’re not promoting bringing rodents and cockroaches into the home, but this data does suggest that being too clean may not be good.”
The theory “is that as we clean up our environment, our immune system moves away from being geared toward fighting bacteria and parasites,” said Dr. Maria Garcia Lloret, an assistant clinical professor of pediatric allergy and immunology at the Mattel Children’s Hospital at the University of California, Los Angeles. “It then has nothing to do and starts to react against things that are normally not harmful, like dust mites, or cat dander or cockroaches or peanuts.”
A chink in the hygiene hypothesis seemed to be the high rates of allergy and asthma in inner-city environments. But the new study may help explain the contradictions by showing that early exposure is crucial.
“It’s all about being exposed to the right bacteria at the right time,” Spergel said.
Wood and his colleagues followed 467 newborns for three years, screening them for allergies annually and testing the dust in the houses where they lived for allergens and bacteria. To the researchers’ surprise, kids who were exposed before their first birthday to mouse and cat dander along with cockroach droppings had lower rates of allergies and wheezing by age 3, compared to those who were not exposed so early on.
In fact, wheezing was three times as common among children who had less exposure to those allergens early in life.
The protective effect of early exposure to allergens was amplified if the home also contained a wide variety of bacteria.
The reason may be that “a lot of immune system development that may lead someone down the path to allergies and asthma may be set down early in life,” Wood said.
Researchers aren’t ready to try to translate the new findings into practical advice for parents. But, Lloret said, we now know that “strict avoidance of allergens from the beginning does not protect you, and early exposure in the right context may make the difference between disease and tolerance. You could say that this is the downside of cleanliness.”
The new findings may upend advice experts have been giving to parents on the topic of pets and newborns.
“Twenty years ago we used to tell parents to get the cats and dogs out of the house,” Wood said. “This shows that the younger the child is when you get a pet, the better.”
Do men and women feel pain differently? A new study finds an unexpected gender divide.
Researchers found that men tend to report feeling more pain after major surgeries than women, whereas women tend to report experiencing more pain after minor surgical procedures than men.
In the study, researchers found that men were 27 percent more likely to report higher pain ratings after a major surgery such as a knee replacement, while women were 34 percent more likely to report experiencing more pain after procedures that the researchers labeled as minor, such as biopsies. (The researchers differentiated between "major" and "minor" procedures depending on the intensity of pain that people typically expect to feel after a particular procedure.)
To conduct the study, the researchers interviewed 10,200 patients from the University Hospitals of the Ruhr University of Bochum, Germany, following an operation, over more than four years. About 42 percent of the patients were male and 58 percent were female.
Initially, the study authors didn't find significant differences between the genders in people's overall experience of postoperative pain. However, that changed when the researchers distinguished between different kinds of surgeries.
The researchers are not sure where these differences stem from; however, they speculate that a lot may depend on the kind of surgery a person is undergoing. For instance, procedures such as cancer-related biopsies or an abortion may take a particularly serious emotional toll on women, and therefore exacerbate their individual perceptions of pain.
"It could be anxiety," study author Dr. Andreas Sandner-Kiesling of Medical University of Graz, Austria, told CBS News.
"This is a very interesting study," Dr. M. Fahad Khan, an assistant professor in the Department of Anesthesiology at NYU Langone Medical Center, told CBS News. "Ten thousand patients in any type of study is a huge number, and it is really great to see studies on that number of patients because it can limit a lot of the bias that some studies have."
Khan noted he found it interesting that in women, even smaller procedures "can be fraught with the development of pain problems after the procedure," which many people may not expect when they go to the hospital for a simple biopsy, he said.
Sandner-Kiesling said he did not think the findings should change the way men and women are treated for pain. "Clinically, there is no relevance," he said.
According to certain popular cultural stereotypes, women are often considered to be tougher about dealing with pain than men, but is this really the case?
"Anecdotally, people will say that women have a higher threshold for pain and they are more tolerant to pain, just because of their life experience. And perhaps, emotionally, maybe they are stronger than men," Khan said. "However, medically, in my experience, we haven't really noticed much of a difference with regard to men and women in the development of problems with dealing with severe and chronic pain."
The new study is presented at this year's Euroanaesthesia meeting in Stockholm.
First up in this week’s news is a look at an article on humor and the mental health of senior citizens I found over at healthday.com. A new study from researchers at Loma Linda University in California looked at the effects of the stress hormone cortisol on aging patients’ memory and mental acuity. They studied the possibility that laughter might lower the effects of cortisol on the seniors.
Healing Power of Funny Videos
Two groups of senior citizens were shown a funny 20 minute video and then were tested on their memory and mental acuity as well as cortisol levels. This was then compared to tests on a group who did not see the video. The subjects who saw the funny video were found to score better on the memory tests and had lower cortisol levels suggesting that regular exposure to funny and humorous things can improve memory and mental state of seniors.
The study was presented recently at the Experimental Biology conference in San Diego. One of the authors summed up the research saying, “it’s simple, the less stress you have, the better your memory.” This doesn’t mean that we need to be comedians in the midst of our care for patients but it does point to the core nursing tenet that when we treat the whole patient we manage their overall health better.
Make sure your hospitals have access to humorous videos and movies in their in-house TV system. Maybe even share a suggested funny YouTube video of the day with your patients who wish to view it. When appropriate, you could even open up your patient interactions with a simple joke. Maybe “why did the chicken cross the road” will be a precursor to better patient interactions in the future.
Melvyn Amrine, of Little Rock, Ark., may not remember the details of his life since his Alzheimer's diagnosis, but he recently proved that his love for his wife transcends memory.
Melvyn was diagnosed with Alzheimer's disease three years ago and since then it hasn't been easy for his wife, Doris, CBS News reported. Melvyn at times doesn't remember details like whether he proposed to his wife, or vice versa. However a recent holiday prompted Melvyn to remember the most important thing.
On the day before Mother's Day, Melvyn went missing. Considering he normally requires assistance to do any walking, his family was alarmed and notified the police.
When police found Melvyn, he was 2 miles from his house and he was resolute in his goal, according to Fox 16. He was going to the store to buy flowers for his wife for Mother's Day, just like he had done every year since they had their first child.
Sgt. Brian Grigsby and Officer Troy Dillard were touched by Melvyn's determination, and decided to help the elderly man complete his mission by taking him to a store and even paying for the flowers.
"We had to get those flowers," Grigsby told CBS News. "We had to get them. I didn't have a choice."
Melvyn's flowers made a very sweet surprise for his wife of 60 years, Doris, as well as a reminder to the rest of us that love knows no obstacles.
"When I saw him waking up with those flowers in hand, it just about broke my heart because I thought 'Oh he went there to get me flowers because he loves me,'" Doris told Fox 16.
She added to CBS News: "It's special, because even though the mind doesn't remember everything, the heart remembers."
Despite new technology and evidence-based guidelines, medical mistakes happen too frequently and may lead to as many as 400,000 preventable deaths each year.
But two new programs, launched at the University of Virginia Medical Center, offer a new approach to patient safety that may prevent medical errors, WVTF PublicRadio reports.
This year the organization introduced a simulation lab in the pediatric intensive care unit. The "Room of Errors" features high-tech infant mannequins attached to monitors. When doctors and nurses enter the lab, they have seven minutes to determine what is wrong.
As part of a recent exercise, a doctor-nurse team worked together to spot 54 problems with the scenario, including the fact the ventilator wasn't plugged into the correct outlet, the heat wasn't turned on and the potassium chloride was programmed at the wrong concentration.
The interpersonal, team-based learning approach helps doctors and nurses improve their ability to make decisions together and communicate with one another, Valentina Brashers, M.D., co-director of the Center for Interprofessional Research and Education, an effort headquartered at UVa's Schools of Nursing and Medicine, told WVTF.
"Knowing that there are others that you can work to think with you and share with you their concerns as you work through difficult problems makes care provision a much more enjoyable and rewarding activity. It reduces staff turnover. It creates an environment where we feel like we're all in it together with the patient," she said.
The pilot proved so successful that the medical center intends to roll it out to the entire hospital.
In its quest to eliminate medical mistakes at the organization, UVa also launched a second patient safety initiative that calls for hospital administrators to meet each morning to talk about any problems that occurred in the previous 24 hours, according to a second WVFT article.
The "Situation Room" features white boards and monitors, where administrators review every new infection and unexpected death and then visit the places where the problems took place.
Sometimes the solutions are easy fixes, such as a receptionist who removed a mat that caused patients to trip at the entrance of an outpatient building. Others, caused by communication problems, are more complicated, Richard Shannon, M.D., executive vice president for health affairs, told the publication. To address it, Shannon wants to shake up the medical hierarchy where the physician sits at the top.
"The physician may spend 20 minutes at the bedside a day. The nurse is there 24/7 and has about 13 times more direct contact with the patient than does the physician," he told WVFT. "You can't have someone at the head of the pyramid who is absent a lot of the time."
Finally, to encourage better communication among caregivers, patients and families, Shannon now encourages healthcare professionals to make rounds in the afternoon, when visitors are on premises.
People who speak more than one language tend to score higher on memory and other cognitive function tests as they get older, but researchers haven’t been able to credit bilingualism as the definitive reason for their sharper intellects. It wasn’t clear, for example, whether people who spoke multiple languages have higher childhood intelligence, or whether they share some other characteristics, such as higher education overall, that could explain their higher scores.
Now, scientists think they can say with more certainty that speaking a second language may indeed help to improve memory and other intellectual skills later in life. Working with a unique population of 853 people born in 1936 who were tested and followed until 2008-2010, when they were in their 70s, researchers found that those who picked up a second language, whether during childhood or as adults, were more likely to score higher on general intelligence, reading and verbal abilities than those who spoke one language their entire lives. Because the participants, all of whom were born and lived near Edinburgh, Scotland, took aptitude tests when they were 11, the investigators could see that the effect held true even after they accounted for the volunteers’ starting levels of intelligence.
Reporting in the Annals of Neurology, they say that those who began with higher intellect scores did show more benefit from being bilingual, but the improvements were significant for all of the participants. That’s because, the authors suspect, learning a second language activates neurons in the frontal or executive functions of the brain that are generally responsible for skills such as reasoning, planning and organizing information.
Even more encouraging, not all of the bilingual people were necessarily fluent in their second language. All they needed was enough vocabulary and grammar skills in order to communicate on a basic level. So it’s never too late to learn another language – and you’ll be sharper for it later in life.
Maya Angelou was born Marguerite Annie Johnson in St. Louis, Missouri. Her parents divorced when she was only three and she was sent with her brother Bailey to live with their grandmother in the small town of Stamps, Arkansas. In Stamps, the young girl experienced the racial discrimination that was the legally enforced way of life in the American South, but she also absorbed the deep religious faith and old-fashioned courtesy of traditional African American life. She credits her grandmother and her extended family with instilling in her the values that informed her later life and career. She enjoyed a close relationship with her brother. Unable to pronounce her name because of a stutter, Bailey called her "My" for "My sister." A few years later, when he read a book about the Maya Indians, he began to call her "Maya," and the name stuck.
At age seven, while visiting her mother in Chicago, she was sexually molested by her mother's boyfriend. Too ashamed to tell any of the adults in her life, she confided in her brother. When she later heard the news that an uncle had killed her attacker, she felt that her words had killed the man. She fell silent and did not speak for five years.
Maya began to speak again at 13, when she and her brother rejoined their mother in San Francisco. Maya attended Mission High School and won a scholarship to study dance and drama at San Francisco's Labor School, where she was exposed to the progressive ideals that animated her later political activism. She dropped out of school in her teens to become San Francisco's first African American female cable car conductor. She later returned to high school, but became pregnant in her senior year and graduated a few weeks before giving birth to her son, Guy. She left home at 16 and took on the difficult life of a single mother, supporting herself and her son by working as a waitress and cook, but she had not given up on her talents for music, dance, performance and poetry.
In 1952, she married a Greek sailor named Anastasios Angelopulos. When she began her career as a nightclub singer, she took the professional name Maya Angelou, combining her childhood nickname with a form of her husband's name. Although the marriage did not last, her performing career flourished. She toured Europe with a production of the opera Porgy and Bess in 1954 and 1955. She studied modern dance with Martha Graham, danced with Alvin Ailey on television variety shows, and recorded her first record album, Calypso Lady in 1957.
She had composed song lyrics and poems for many years, and by the end of the 1950s was increasingly interested in developing her skills as a writer. She moved to New York, where she joined the Harlem Writers Guild and took her place among the growing number of young black writers and artists associated with the Civil Rights Movement. She acted in the historic Off-Broadway production of Jean Genet's The Blacks and wrote and performed a Cabaret for Freedom with the actor and comedian Godfrey Cambridge.
In New York, she fell in love with the South African civil rights activist Vusumzi Make and in 1960, the couple moved, with Angelou's son, to Cairo, Egypt. In Cairo, Angelou served as editor of the English language weekly The Arab Observer. Angelou and Guy later moved to Ghana, where she joined a thriving group of African American expatriates. She served as an instructor and assistant administrator at the University of Ghana's School of Music and Drama, worked as feature editor forThe African Review and wrote for The Ghanaian Times and the Ghanaian Broadcasting Company.
During her years abroad, she read and studied voraciously, mastering French, Spanish, Italian, Arabic and the West African language Fanti. She met with the American dissident leader Malcolm X in his visits to Ghana, and corresponded with him as his thinking evolved from the racially polarized thinking of his youth to the more inclusive vision of his maturity.
Maya Angelou returned to America in 1964, with the intention of helping Malcolm X build his new Organization of African American Unity. Shortly after her arrival in the United States, Malcolm X was assassinated, and his plans for a new organization died with him. Angelou involved herself in television production and remained active in the Civil Rights Movement, working more closely with Dr. Martin Luther King, Jr., who requested that Angelou serve as Northern Coordinator for the Southern Christian Leadership Conference. His assassination, falling on her birthday in 1968, left her devastated. With the guidance of her friend, the novelist James Baldwin, she found solace in writing, and began work on the book that would become I Know Why the Caged Bird Sings. The book tells the story of her life from her childhood in Arkansas to the birth of her child. I Know Why the Caged Bird Sings was published in 1970 to widespread critical acclaim and enormous popular success.
Seemingly overnight, Angelou became a national figure. In the following years, books of her verse and the subsequent volumes of her autobiographical narrative won her a huge international audience. She was increasingly in demand as a teacher and lecturer and continued to explore dramatic forms as well. She wrote the screenplay and composed the score for the film Georgia, Georgia (1972). Her screenplay, the first by an African American woman ever to be filmed, was nominated for a Pulitzer Prize.
Angelou was invited by successive Presidents of the United States to serve in various capacities. President Ford appointed her to the American Revolution Bicentennial Commission and President Carter invited her to serve on the Presidential Commission for the International Year of the Woman. President Clinton requested that she compose a poem to read at his inauguration in 1993. Angelou's reading of her poem "On the Pulse of the Morning" was broadcast live around the world.
Since 1981, Angelou has served as Reynolds Professor of American Studies at Wake Forest University in Winston-Salem, North Carolina. She has continued to appear on television and in films including Poetic Justice (1993) and the landmark television adaptation of Roots (1977). She directed numerous dramatic and documentary programs on television and directed a feature film,Down in the Delta, in 1996.
The list of her published works includes more than 30 titles. These include numerous volumes of verse, beginning with Just Give Me a Cool Drink of Water 'Fore I Die (1971). Books of her stories and essays include Wouldn't Take Nothing For My Journey Now (1993) and Even the Stars Look Lonesome(1997). She continued the compelling narrative of her life in the books Gather Together in My Name (1974), Singin' and Swingin' and Gettin' Merry Like Christmas (1976), The Heart of a Woman (1981), All God's Children Need Traveling Shoes(1987) and A Song Flung Up to Heaven (2002).
In 2000, Dr. Angelou was honored with the Presidential Medal of the Arts; she received the Ford's Theatre Lincoln Medal in 2008. The same year, she narrated the award-winning documentary film The Black Candle and published a book of guidance for young women, Letter to My Daughter. In 2011, President Barack Obama awarded her the nation's highest civilian honor, the Presidential Medal of Freedom.
Maya Angelou participated in a series of live broadcasts for Achievement Television in 1991, 1994 and 1997, taking questions submitted by students from across the United States. The interview with Maya Angelou on this web site has been condensed from these broadcasts.
How well can computers interact with humans? Certainly computers play a mean game of chess, which requires strategy and logic, and “Jeopardy!,” in which they must process language to understand the clues read by Alex Trebek (and buzz in with the correct question).
But in recent years, scientists have striven for an even more complex goal: programming computers to read human facial expressions.
The practical applications could be profound. Computers could supplement or even replace lie detectors. They could be installed at border crossings and airport security checks. They could serve as diagnostic aids for doctors.
Researchers at the University of California, San Diego, have written software that not only detected whether a person’s face revealed genuine or faked pain, but did so far more accurately than human observers.
While other scientists have already refined a computer’s ability to identify nuances of smiles and grimaces, this may be the first time a computer has triumphed over humans at reading their own species.
“A particular success like this has been elusive,” said Matthew A. Turk, a professor of computer science at the University of California, Santa Barbara. “It’s one of several recent examples of how the field is now producing useful technologies rather than research that only stays in the lab. We’re affecting the real world.”
People generally excel at using nonverbal cues, including facial expressions, to deceive others (hence the poker face). They are good at mimicking pain, instinctively knowing how to contort their features to convey physical discomfort.
And other people, studies show, typically do poorly at detecting those deceptions.
In a new study, in Current Biology, by researchers at San Diego, the University of Toronto and the State University of New York at Buffalo, humans and a computer were shown videos of people in real pain or pretending. The computer differentiated suffering from faking with greater accuracy by tracking subtle muscle movement patterns in the subjects’ faces.
“We have a fair amount of evidence to show that humans are paying attention to the wrong cues,” said Marian S. Bartlett, a research professor at the Institute for Neural Computation at San Diego and the lead author of the study.
For the study, researchers used a standard protocol to produce pain, with individuals plunging an arm in ice water for a minute (the pain is immediate and genuine but neither harmful nor protracted). Researchers also asked the subjects to dip an arm in warm water for a moment and to fake an expression of pain.
Observers watched one-minute silent videos of those faces, trying to identify who was in pain and who was pretending. Only about half the answers were correct, a rate comparable to guessing.
Then researchers provided an hour of training to a new group of observers. They were shown videos, asked to guess who was really in pain, and told immediately whom they had identified correctly. Then the observers were shown more videos and again asked to judge. But the training made little difference: The rate of accuracy scarcely improved, to 55 percent.
Then a computer took on the challenge. Using a program that the San Diego researchers have named CERT, for computer expression recognition toolbox, it measured the presence, absence and frequency of 20 facial muscle movements in each of the 1,800 frames of one-minute videos. The computer assessed the same 50 videos that had been shown to the original, untrained human observers.
The computer learned to identify cues that were so small and swift that they eluded the human eye. Although the same muscles were often engaged by fakers and those in real pain, the computer could detect speed, smoothness and duration of the muscle contractions that pointed toward or away from deception. When the person was experiencing real pain, for instance, the length of time the mouth was open varied; when the person faked pain, the time the mouth opened was regular and consistent. Other combinations of muscle movements were the furrowing between eyebrows, the tightening of the orbital muscles around the eyes, and the deepening of the furrows on either side of the nose.
The computer’s accuracy: about 85 percent.
Jeffrey Cohn, a University of Pittsburgh professor of psychology who also conducts research on computers and facial expressions, said the CERT study addressed “an important problem, medically and socially,” referring to the difficulty of assessing patients who claim to be in pain. But he noted that the study’s observers were university students, not pain specialists.
Dr. Bartlett said she didn’t mean to imply that doctors or nurses do not perceive pain accurately. But “we shouldn’t assume human perception is better than it is,” she said. “There are signals in nonverbal behavior that our perceptual system may not detect or we don’t attend to them.”
Dr. Turk said that among the study’s limitations were that all the faces had the same frontal view and lighting. “No one is wearing sunglasses or hasn’t shaved for five days,” he said.
Dr. Bartlett and Dr. Cohn are working on applying facial expression technology to health care. Dr. Bartlett is working with a San Diego hospital to refine a program that will detect pain intensity in children.
“Kids don’t realize they can ask for pain medication, and the younger ones can’t communicate,” she said. A child could sit in front of a computer camera, she said, referring to a current project, and “the computer could sample the child’s facial expression and get estimates of pain. The prognosis is better for the patient if the pain is managed well and early.”
Dr. Cohn noted that his colleagues have been working with the University of Pittsburgh Medical Center’s psychiatry department, focusing on severe depression. One project is for a computer to identify changing patterns in vocal sounds and facial expressionsthroughout a patient’s therapy as an objective aid to the therapist.
“We have found that depression in the facial muscles serves the function of keeping others away, of signaling, ‘Leave me alone,’ ” Dr. Cohn said. The tight-lipped smiles of the severely depressed, he said, were tinged with contempt or disgust, keeping others at bay.
“As they become less depressed, their faces show more sadness,” he said. Those expressions reveal that the patient is implicitly asking for solace and help, he added. That is one way the computer can signal to the therapist that the patient is getting better.
DURHAM, N.C. — Before scrubbing in on a recent Tuesday morning, Dr. Selene Parekh, an orthopedic surgeon here at Duke Medical Center, slipped on a pair of sleek, black glasses — Google Glass, the wearable computer with a built-in camera and monitor.
He gave the Internet-connected glasses a voice command to start recording and turned to the middle-aged motorcycle crash victim on the operating table. He chiseled through bone, repaired a broken metatarsal and drilled a metal plate into the patient’s foot.
Dr. Parekh has been using Glass since last year, when Google began selling test versions of its device to thousands of handpicked “explorers” for $1,500. He now uses it to record and archive all of his surgeries at Duke, and soon he will use it to stream live feeds of his operations to hospitals in India as a way to train and educate orthopedic surgeons there.
“In India, foot and ankle surgery is about 40 years behind where we are in the U.S.,” he said. “So to be able to use Glass to broadcast this and have orthopedic surgeons around the world watch and learn from expert surgeons in the U.S. would be tremendous.”
At Duke and other hospitals, a growing number of surgeons are using Google Glass to stream their operations online, float medical images in their field of view, and hold video consultations with colleagues as they operate.
Software developers, too, have created programs that transform the Glass projector into a medical dashboard that displays patient vital signs, urgent lab results and surgical checklists.
“I’m sure we’re going to use this in medicine,” said Dr. Oliver J. Muensterer, a pediatric surgeon who recently published the first peer-reviewed study on the use of Glass in clinical medicine. “Not the current version, but a version in the future that is specially made for health care with all the privacy, hardware and software issues worked out.”
For his study, published in The International Journal of Surgery, Dr. Muensterer wore the device daily for four weeks at Maria Fareri Children’s Hospital at Westchester Medical Center in New York. He found that filming rapidly drains the battery and that the camera — which is mounted straight ahead — does not point directly at what he is looking at when he is hunched over a patient with his eyes tilted downward.
He also had to keep the device disconnected from the Internet most of the time to prevent patient data and images from being automatically uploaded to the cloud. “Once it’s on the cloud, you don’t know who has access to it,” Dr. Muensterer said.
Google has yet to announce a release date for Glass, and the company declined to comment on how many of its testers were doctors or affiliated with hospitals. But “demand is high,” said Nate Gross, a co-founder of Rock Health, a medical technology incubator. “I probably get asked every few days by another doctor who wants to somehow incorporate Glass into their practice.”
And already, outside hospitals, privacy concerns have led some bars and restaurants to ban the devices. Legislators have proposed restrictions on the use of Google Glass while driving, citing concerns about distraction. Doctors, too, are raising similar concerns.
The Glass projector is slightly above the user’s right eye, allowing doctors to see medical information without turning away from patients. But the display can also be used to see email and surf the web, potentially allowing doctors to take multitasking to dangerous new levels, said Dr. Peter J. Papadakos at the University of Rochester Medical Center, who has published articles on electronic distractions in medicine.
“Being able to see your laparoscopic images when you’re operating face to face instead of looking across the room at a projection screen is just mind-bogglingly fantastic,” he said. “But the downside is you don’t want that same surgeon interacting with social media while he’s operating.”
Indeed, similar technology has not always had the smoothest results. Studies have found, for example, that navigational displays can help surgeons find tumors, but they can also induce a form of tunnel vision, or perceptual blindness, that makes them more likely to miss unrelated lesions or problems in surrounding tissue. And in aviation, pilots who wear head-mounted displays that show crucial flight information can lose sight of what is happening outside their windshields, said Dr. Caroline G. L. Cao, who studies image-guided surgery at Wright State University.
“Pilots can get so focused on aligning the icons that help them land the plane,” she said, “that they miss another plane that is crossing the runway.”
One doctor who does not allow the device in his practice, Dr. Matthew S. Katz, the medical director of radiation oncology at Lowell General Hospital in Massachusetts, said that security and distractions were primary concerns. A doctor wearing Glass could accidentally stream confidential medical information online, he said, and patients might not feel comfortable with their doctors wearing cameras on their faces.
Until Glass has been better studied in health care and equipped with safeguards, Dr. Katz said, doctors should be forced to check their wearable computers at the clinic door.
“From an ethical standpoint, the bar is higher for use in a medical setting,” said Dr. Katz, who is also an outside adviser for the Mayo Clinic Center for Social Media. “As a doctor, I have to make sure that what I’m doing is safe and secure for my patients — ‘First, do no harm.’ Until I am, I don’t want it in my practice.”
Bakul Patel, the senior policy adviser at the Food and Drug Administration’s Center for Devices, said the agency would regulate only those Glass software programs that function as medical devices, the same approach it takes on health applications on hand-held devices.
“The glasses have been on our radar and we’re excited about it,” Mr. Patel said.
Hospitals that are experimenting with Glass say they are doing so very carefully — obtaining patient consent before procedures, using encrypted networks, and complying with the federal regulation that protects patient privacy, known as Hipaa.
Medical software developers say they, too, have security and privacy in mind. Pristine, a company based in Austin, Tex., createdan app that lets emergency room nurses and doctors beam in specialists for consultations. The company plans to sell a customized version of Glass directly to hospitals. It erases Google’s software and configures the glasses with its own Hipaa-compliant programs.
Another company, Augmedix, which has done pilot tests of Glass at medical centers in the San Francisco area, said patients were informed that their doctors would be wearing the device. In a study of 200 cases, only two or three patients asked that their doctors remove it, said Ian K. Shakil, a co-founder of Augmedix.
Some hospitals see Glass as a relatively low-cost and versatile innovation, much like smartphones and tablets, which more than half of all health care providers use to get access to patient data and other medical information.
But hand-held devices are not very useful in the sterile world of surgery. Because Glass is voice-activated and hands-free, it may be particularly well suited for the surgical suite, where camera-guided instruments, robotics and 3D navigation systems have been commonplace for years.
Dr. Pierre Theodore, a cardiothoracic surgeon at the University of California, San Francisco, calls wearable computers “a game changer.”
“In surgery, Google Glass is incredibly illuminating,” said Dr. Theodore, who uses Glass to float X-rays and CT scans in his field of view at the operating table. “It helps you pinpoint what you’re looking for, so you don’t have to shift your attention away from the operation to look at a monitor somewhere else.”
At Indiana University Health, Dr. Paul P. Szotek, a Level 1 trauma surgeon, is developing an app for Glass for use by paramedics.
The app streams a live feed from the glasses to the closest emergency rooms, so that doctors can see accident victims at the scene and give paramedics potentially lifesaving instructions — like when to go directly to a Level 1 trauma center.
“Last year, I lost a lady on the table from a spleen injury that was absolutely survivable because she was taken to a local hospital and then the delay was over two hours to get her to me,” Dr. Szotek said. “With this wearable technology, we’ll be able to assess patients on the scene and decrease the mortality associated with trauma significantly.”
Dr. Szotek met with Google in March to discuss his software, called 1st Sight. He and other Glass-wearing surgeons recently founded a group — the International Society for Wearable Technology in Healthcare — that is holding its first meeting in Indianapolis in July.
At Duke, Dr. Parekh performs back-to-back surgeries on most days, wearing the Glass headset as he moves from one patient to the next.
About six years ago, he founded a charity with the goal of advancing foot and ankle surgery in India. He travels there every year with a team of expert surgeons to hold clinics and training sessions for local orthopedic surgeons.
In January, at a conference in Jaipur, Dr. Parekh performed surgery and used Glass to stream the procedure on his personal website. That day, the site drew in so many visitors from India and elsewhere that it crashed.
“I’ve been even more excited about Google Glass since then,” he said.
Everybody knows that the nursing profession has two different sides—it is both science and art. That said, nursing as a science is more apparent.
For example, if you are a nurse, you must know the patient-based nursing care plan (NCP). You must also know the disease mechanisms of all diseases, medications, and management from all sides. Nurses also need to be up to date on new policies, practices, and procedures. Moreover, they need to know how to manipulate new diagnostic equipment and machines.
The science of nursing is easily noticeable and it is very critical for each one to know.
What Is the Art?
Meanwhile, the art of nursing is more than a great deal of science. It is more than just knowing; it is doing. It bridges information from nurses to patients in a skillful way. It is the application of all the science known to nursing to give the utmost care the patient needs.
During your first year in the nursing profession, you are in the heat of the moment. You now belong to that bunch of young professionals who are enthusiastic and motivated in practicing their craft. Maybe many could attest that when you first become a nurse you see the art more than the science of it.
But it is sad to note that as time passes by the semblance of the nursing being an art bleeds out. At the drop of a hat, you get suffocated from the career you once loved.
The Human Touch
In the past 7 years that I have been a clinical instructor, I have seen so many changes in the healthcare arena and how nursing should be. But one thing remains: human nature.
Our patients’ needs have remained constant and relentless. As Maslow’s hierarchy of needs suggests, these include food, sense of belonging, warmth, compassion, self-actualization. These basic needs have been addressed in the same way since the dawn of science. However, the ways to meet them may have changed from time to time.
The art of nursing may have been in each person even before entering the profession. That innate capacity to respond to the needs of individual is already the art of nursing. In nursing school, this vivacity is awakened through constant interaction with the patients in various settings.
Nurses are called to perform relational work. Therefore, the motivation to keep that art in us should be continuously burning. We have the power to heal the sick. An effective nurse is one who gives nursing care independently and collaboratively with other healthcare teams.
The art of nursing comes in as a nurse independently does his or her job. The options s/he considers in taking a certain action and ultimately the action s/he does to respond to patient needs are the art of nursing.
It is in the nurses’ hands to promote positive changes in patients. Everyday we are faced with patients who are in different conditions. In this case, individualized nursing care is noteworthy. Knowledge is not enough. Compassionate care is paramount.
Where Is the Art?
In my experience, I have witnessed things in which nursing as an art is not manifested. I squirmed while hearing a nurse teaching pre-operative patients without compassion. Instead of comfort, fear is built within the patients. I have observed nurses, who are not well informed about a disease process, explain things to patients without using therapeutic communication. I have noted procedures done outside the context of the protocols and sterile technique.
Sadly, many of these incidents are from those who have been in the profession for so long. Science is applied, but where is the art in this perspective?
Clearly, nurses must be equipped with the science of nursing. But until the art of nursing is recognized as a necessary principle for patient care, nurses will likely to continue to demonstrate behaviors that make them good technicians. However, they will not necessarily be good nurses.
As a field grounded in compassion and direct patient care, the art of the nursing profession is more important than the science. And this is where the so-called calling comes into play.
Judge's notes: This team made a change for the greater good. The initiative benefits not just the hospital but their community and beyond. They used a scientific, research-based approach and gained support from multidiscipline teams, management and administration.
It started with a single question: "Why can't I recycle this?" In the main operating room, we perform approximately 1,500 cases per month, all requiring sterile instrumentation, sterile water, sterile saline, packaged sterile supplies and implants. All of our supplies are packaged in disposable recyclable material. Operating rooms across the country contribute the largest amount of municipal trash in a hospital, secondary only to food services. If we were able to recycle half of what we used, we could make a major impact not only to our landfills and community, but potentially our small part of the world.
Jennifer Pallotta, BSN, RN, CNOR, inpatient operating room, masterminded the project. She empowered all who chose to become involved. Together, Jennifer and I spearheaded this massive undertaking. We gathered nurses, technicians, anesthesiologists and the Environmental Services Department staff to help assist with our endeavor. Together, we would all make a difference.
Our first step was educating ourselves in the art of recycling. We did it at home; how difficult could it be? We spoke with our managers and gained support and buy-in, for without them this huge practice change would have never been achievable. We joined our hospital-based "Green Team" and educated ourselves on what would be required. We then began to educate the staff, slowly introducing the concept of recycling product from the operating room. Surgery and anesthesia chairmen were informed of our initiative via emails and introductions at committee meetings. It was imperative that we had the surgery and anesthesia staff as involved as the perioperative personnel. An area of concern would be the Environmental Services Department, for without them our study could be in jeopardy. We were amazed at the enthusiasm that they displayed when we began our educational process with them. We informed them that without their support, our study would surely fail. It was a priority for Jennifer and me to ensure that they were comfortable with the process, and truly understood what a driving force their support would be. By empowering the Environmental Service Department, we gained allies that would last much longer than our study.
We initiated a pilot program. Phase I we monitored and measured five operating rooms: ENT/gynecological, laparoscopic, orthopedic, robotic and neurosurgical procedures. We would do this for a period of one month, three times a week. We would base our results on the amount of trash (weight) that we produced, separating only red bag waste from regular trash.
Coincidentally, the end of Phase I coincided with our institution's signing a Memorandum of Understanding with the Environmental Protection Agency. Not only did we have buy-in and support from our managers, but we also received support from our president and chief executive officer, as well as our executive vice president and chief nursing and patient care officer. Once the one-month period was complete and we had our baseline statistics, the real fun began. We would need to educate staff on recycling of operating room supplies: What could be recycled as opposed to what could not be. What material was acceptable, and what we needed to watch out for. We began an educational program that consisted of in-services, posters, banners and giveaways. Jennifer and I made ourselves available at all times for questions and answers for whoever had concerns.
Phase II of our project began with the same five operating rooms, but the difference is that a recycling trash receptacle was now added. We learned from Phase I of our study that the majority of supplies placed into the red hazardous waste bag did not need to be there. A serendipitous moment came when we were able to remove the red bag receptacle from the operating rooms, and only have it available upon need. We were able to reduce our red bag waste by 50% percent; not only eliminating the financial cost of the bags, but also dramatically decreasing the cost of disposal.
During Phase II of our study we continued positive reinforcement, taking pictures of staff recycling to encourage the team. The staff members enjoyed seeing their photos displayed on the bulletin boards - all caught in the act of recycling. The staff began to take pride and ownership in the project, and began to realize that they were making a difference in something that they had full control over. Acts of positive peer pressure began to emerge. Recycling even caught on with our surgeons being more vigilant on where they disposed of their gowns and gloves; not wanting to contaminate the recyclable items.
The end of Phase II was celebrated amongst the staff. We held a party during our monthly staff in-service decorating the room, serving coffee and breakfast to the staff. We celebrated the fact that we as a team were able to increase our recycling by 34%, hence decreasing 34% of municipal waste that is dumped into our landfills. We cut our hazardous red bag waste by 50%, eliminating the cost of supplies of red bags as well as disposal fees. Our celebration ended with each registered nurse entering the operating suite with a 64-gallon blue recycling bin for each of the 22 operating rooms in the main operating arena.
This greening initiative was very exciting. The recycling bug caught on. In an age where hospitals need to remain conscious of the earth and be aware of the potential hazards that we can add to the environment, the act of giving back and being green is something that we all can do. By recycling in the operating room, we showed the rest of the medical center that it was certainly possible for them to participate and play a part in this new culture.
This was truly the start of a new era all arising from one simple question, "Why can't I recycle this?"
Wet snowflakes fell on that day after Christmas 1973 as she glanced out the window.
Nancy Whittaker just wanted to return a few presents with her boyfriend, but her parents worried about her making the 40-mile trip from Beatrice to Lincoln. Maybe it was best if they made the drive another day, after the weather improved.
I'll be fine, Nancy told them before sliding into the front seat. Nancy, 17 at the time, sat in the middle of the bench seat, with her 19-year-old boyfriend, Paul Cramer, on her right, and his college roommate behind the wheel.
Nancy, a pretty and popular senior at Beatrice High School, planned to attend college and follow her dream of becoming a nurse.
She wanted a career, but her greatest hope — one she had wished for since she was little — was becoming a wife and mother. She wondered if Paul might be the man she would marry someday.
Nancy and the two others set out on their trip that winter day 40 years ago, but they never arrived in Lincoln.
In the years that followed, Nancy would face tough obstacles reaching her dreams. Though she wouldn't fulfill them all, she would reach most, including motherhood. And through her faith, courage and perseverance she would inspire her children to achieve one dream that fell from her grasp.
Before Nancy left on the trip that day, she spoke with her dad about a Christmas present she'd given him.
It was her senior picture in a wooden frame. She reminded him to hang it in his office at work.
There was Nancy, with her blue eyes and long blond hair, smiling in the photo.
Her father promised he'd take it to work, and gave her a hug and kiss.
Be careful, he told her.
* * *
Nancy and the others stopped to fill the white two-door Dodge with gas before heading north out of Beatrice on U.S. Highway 77 — a two-lane road in those days.
Seven miles north of Beatrice, the Dodge trailed a truck near the tiny town of Pickrell about 2:20 p.m. Newspaper stories and a sheriff's report indicate the car moved into the opposite lane. Paul caught a split-second glimpse of the oncoming sedan. He instinctively braced himself against the dashboard with his right arm and threw the other across Nancy's chest.
The two cars collided head-on, according to news reports. The other car carried a 75-year-old Kansas man and his wife, who both died in the crash.
Nancy's head smashed against the dash, crushing the middle third of her face. She broke a hip, her pelvis and jaw. Paul broke an ankle, nearly severed a finger and suffered a concussion and chest injury. His roommate also was injured.
In an emergency room in Beatrice, Nancy remembers hearing voices and her family doctor exclaim, “Oh, my God.”
Her face throbbed with pain, and she couldn't see.
You've been in a car accident, her father told her, but you will be OK.
Why can't I see, she asked.
Doctors are taking good care of you, her dad replied. They will figure that out.
Within hours of the crash, doctors transferred her by ambulance to a Lincoln hospital. A nurse Nancy knew sat in the back with her during the drive. The previous summer Nancy had worked as a nurse's aide and the woman had trained her.
The nurse held her hand, and though Nancy still could not see, she felt peaceful, as if the Lord held her in His arms.
In Lincoln, Nancy underwent the first of what would be nearly a dozen plastic surgeries to reconstruct her face. The surgeon who performed the first eight-hour operation told Nancy's family her facial bones were so shattered that it was like “stringing pearls” together.
As she lay in her hospital bed a day or two after the crash, Nancy had a question for her mother.
It wasn't about her eyes, or her face.
Will I still be able to have babies someday?
Her mother leaned over her bed and gently told her yes.
Nancy was relieved, but soon would learn devastating news.
Within a week of the accident, doctors told her what she had feared: She was permanently and completely blind. Her optic nerves were dead because injuries had cut off their blood supply.
Nancy felt the Lord would take care of her, but she was scared, and her mind raced.
How would she get around? How would she pick out clothes? How would she put on makeup?
Could she still go to college? What would her boyfriend, Paul, say?
He was recovering at a Beatrice hospital, and soon after Nancy learned about her blindness, he phoned.
He told Nancy he had fallen in love with her months before, and her blindness didn't change that.
“I love you,” he told her on the phone that day, “not what you can see.”
* * *
Nancy remembers a psychiatrist in the hospital telling her she had two choices: Compare her life now to her life before the accident and feel miserable, or move forward.
Nancy picked her path.
After finishing her senior year of high school, she enrolled part time at Nebraska Wesleyan University in Lincoln and moved into a dorm with a friend. Paul was a junior at the school.
She majored in psychology, knowing that without vision, a nursing career simply wouldn't work.
Some textbooks were on reel-to-reel tape, and Nancy listened to them in a study lounge. When she had to write a paper, she dictated sentences to her mom, who typed them. Her professors read test questions to her after class.
Nancy's relationship with Paul grew stronger during their college years, and they married on June 4, 1977.
In May 1981, eight years after she began taking classes half time, Nancy graduated.
When her name was called at the ceremony, she linked arms with Paul and walked across the stage.
The audience rose to its feet and erupted in applause.
* * *
In spring 1986, Nancy heard the words she had longed for: You're pregnant.
She had accepted her blindness because she knew the Lord would bless her and Paul in other ways. A baby, she thought, was that grace.
Nearly two years earlier she'd had a miscarriage, and she and Paul prayed that they would be blessed with another baby.
That baby was born two months premature in October 1986. Paul Andrew was small — 4 pounds, 2 ounces — but healthy.
Nancy remembers hearing his loud cries for the first time, as tears streamed down her face.
Her husband described the baby to her: blue eyes, light hair, a long body.
She held her child on her chest, stroking his hair, cheeks, nose and lips, tracing the outline of his face with her fingers.
He was beautiful.
* * *
Caring for a baby challenges any mom, and Nancy faced extra hurdles.
Plus, soon she no longer had just one son.
Two years and two days after the birth of her first son, Nancy delivered a second healthy boy, Daniel Whittaker.
Keeping her boys safe at home was a big test. She vacuumed constantly to make sure there wasn't a coin or paper clip on the floor her boys could put in their mouths.
Organization was the key for other duties.
Changing diapers and cleaning messy bottoms became a snap because Nancy knew just where to reach for a clean diaper and a wipe.
Her husband marked foods with a label in Braille, making it easy for Nancy to find the applesauce or baby cereal in the kitchen of their Lincoln home.
As her boys got older, she reminded them that mommy couldn't see them, so they needed to tell her if they left a room, and she could follow the sound of their voices.
Nancy, who left a phone company job to raise her family, regularly walked with her sons and a guide dog to a park and their school five blocks from home.
Every couple of years, Nancy visited her sons' grade school and talked about life as a blind person.
How do you get dressed, students asked. How do you walk without bumping into things?
Her sons listened proudly. Those talks helped them realize that blindness didn't stop their mom. It was simply part of her life, and she dealt with it.
As they grew, Nancy's sons learned that mom sometimes needed help, and she wasn't too proud to receive it.
She knew her way around the house but sometimes cut her forehead on an open cupboard. Her boys would dab the wound with soap and water and place a bandage on it.
Nancy always put on her own makeup, but if she smudged her mascara, her boys cleared it with a Q-tip.
When her boys were older, she'd ask them to read the labels on her medicine bottles.
Her sons never complained about helping. Nancy realized they carried a tender and caring nature, and that filled her and her husband with pride.
* * *
Nancy is now 58 and works as a phone interviewer for a university research office in Lincoln. Paul is 60, and the pair — whose relationship flowed from a teenage romance — will celebrate their 37th wedding anniversary next month.
And their boys are grown now.
Paul Andrew, 27, and Daniel, 25, knew their mom had to give up becoming a nurse, and looking back, they realize she channeled her caregiver instincts into raising them.
Her sons were struck by her ability to raise them despite not just her blindness but also her chronic asthma and other medical problems stemming from her car crash injuries.
They joined their mother on dozens of medical appointments while growing up, and saw how the nurses and doctors helped her. Both sons also liked the satisfaction of helping their mom, and how something as simple as them tending to a cut on her forehead made her feel better.
All of those experiences seeped in over the years and led both sons, even as teens, to begin thinking of health care careers.
Though Nancy never reached her dream of becoming a nurse, her sons followed that path.
Paul Andrew graduated last year from the University of Nebraska Medical Center and is a nurse at Immanuel Medical Center in Omaha.
On Friday, Dan walked across the stage at a Lincoln auditorium and received his nursing degree from UNMC. A smile broke across Nancy's face as they called his name.
Afterward in the lobby, Dan weaved through the crowd and found his mother. The 6-foot-4 Dan leaned down and hugged her, as his brother stood close.
For parents, college graduation signals the step into adulthood, although in a mother's mind, the little child never quite disappears.
That's how it is for Nancy.
As the crowd began breaking up, Dan stepped close and told her he loved her.
She reached up and touched the back of his neck with her hand.
When Carrie Bilicki, RN, MSN, ACNS-BC, OCN, met a 60-year-old patient who had been diagnosed with aggressive endometrial cancer, she began to have a persistent — albeit unconventional — idea.
Bilicki, a cancer nurse navigator in Wisconsin at the time, recently had attended a lecture about a progressive treatment for this type of cancer that involved using a chemotherapy drug traditionally prescribed for ovarian cancer. The patient’s cancer had spread to nearby organs, and she had a poor prognosis. Bilicki convinced the physicians to try the alternative medication. Unfortunately, the patient faced another serious hurdle: The insurance company would not cover the cost of the medication because it was not the standard treatment. At that point, the woman seemed to face the unenviable choice between cancer treatment and financial ruin.
Although patients and providers would like to hope this type of extreme dilemma is the exception, the case may be representative of the near future for two reasons. First, as a 60-year-old, the woman was a baby boomer, and researchers predict the incidence of cancer will increase dramatically as this large segment of the population ages. According to a study published in the Journal of Clinical Oncology in 2009, the U.S. can expect a 67% increase in cancer incidence among older adults between 2010 and 2030.
Second, statistics suggest cancer treatment is becoming increasingly unaffordable, even for those with insurance who struggle to afford steep copayments. For example, The US Oncology Network — a national group of about 1,000 oncology physicians who treat more than 750,000 cancer patients per year — reported about half of the patients covered by a Medicare Part D plan have required copay assistance for oral chemotherapy for the past several years.
“My message to my peers is to know the financial resources available because there are hundreds of them,” Bilicki, who now is a clinical nurse specialist in breast services at Froedtert Center for Diagnostic Imaging in Milwaukee, Wis., said. “There are foundations, specialty organizations and websites that tell us where to get help. If a patient does not have an advocate to link them to that resource, they will never know it is available.”
What's new?
For many patients, the desire to find a way to afford medication is driven not only by the fact that they have cancer, but also because the treatment options available today have increased the odds of survival.
“By far one of the biggest advancements is more personalized medicine that targets cancer cells rather than traditional chemotherapy that did not differentiate between good and bad cells,” Kim George, RN, MSN, ACNS-BC, OCN, a cancer program consultant from Wichita Falls, Texas, said. “For example, now we can test biopsy tissue for specific tumor antigens and biomarkers and then prescribe treatments that target those antigens.”
The advancements in cancer treatment also are reflected in improved survival rates. According to the Surveillance Epidemiology and End Results Cancer Statistics Review 1975-2009, for example, the 5-year survival rate for breast cancer among women in the U.S. between 1975 and 1977 was 75%. Between 2002 and 2008 that number jumped to 90%. During the same time periods, the 5-year survival rate for both men and women with colon cancer has increased from 50% to 65%.
“Another major advancement has been the increase in availability of oral chemotherapy and biotherapy,” George said. “It has shifted the care setting. Years ago, the majority of cancer patients received IV infusions, and now more patients can take their medication orally at home. It is wonderful for convenience, and it is also less painful.”
However, George said, reimbursement is not always a given with oral chemotherapy. “A lot of oncology medications are given off-label, which means that the FDA has not approved a drug for a specific diagnosis, so it may not be covered by some insurance policies,” she said.
A little help can mean a lot
Point the way for patients who need assistance financing cancer treatments, by seeking resources such as the following:
• PatientAdvocate.org — Provides sources for copay assistance and answers questions about disability and insurance processes
• PatientResource.com — Features information on different types of cancer, newsletters and financial and advocacy resources
• CureToday.com — Provides an extensive list of national resources for advocacy, financial and pharmaceutical assistance
• RxOutreach.org — A nonprofit organization that helps low-income families who cannot afford the medication they need
• CDFund.org — Chronic Disease Fund — A nonprofit organization that helps patients obtain lifesaving medications
For a list of drug assistance programs from pharmaceutical companies, visit Cancersupportivecare.com/drug_assistance.html.
Point the way
The art of navigating the path to financial assistance for cancer medication is not simple, and organizations such as The US Oncology Network, based in The Woodlands, Texas, have hired professionals to help patients connect with funding resources and launched the OncologyRx Care Advantage pharmacy in 2006. Nurses in the network can refer patients to Care Advantage staff who help them apply for financial assistance.
“The types of drugs used to treat cancer today are definitely more expensive than when I started working in oncology almost 30 years ago,” said Lori Lindsey, RN, MSN, NP, OCN, a clinical services program manager with The US Oncology Network. “Multidrug regimens, including oral targeted therapies, can sometimes cost $30,000 for a round of treatment, although the use of these drugs has markedly improved outcomes and increased survival for some diseases.”
For patients who are uninsured, the best option is to apply directly to the drug manufacturer for patient assistance, said Meg Asher, a patient access coordinator/patient advocate lead at the Care Advantage pharmacy. “When we learn that a patient is without insurance, we notify the doctor’s office and send a manufacturer’s application to them for the patient’s use,” Asher said. “Under these circumstances, we will not be the dispensing pharmacy; the manufacturer has their own specified pharmacy that will service the patient.”
Even those who are insured under Medicare Part D often require assistance because the copayments can be thousands of dollars, Asher said. For these patients, the Care Advantage advocate team helps patients connect with various foundations that provide copay assistance in the form of grants. Some of the foundations assist patients who suffer from a specific disease, while others help those who are taking a specific drug for a disease.
While some facilities have staff trained to help patients find financial assistance, this is not always the case. For these patients, one resource is the Patient Advocate Foundation, a nonprofit organization with case managers who help patients with life-threatening illnesses to maintain financial stability.
“When I was a hospital nurse, I honestly didn’t know about a lot of the resources available to help patients after they left my care,” Pat Jolley, RN, the clinical director of research and reporting at PAF, said. “Many people have never had to ask for financial help in the past, and they are unaware that there are options. If they are newly diagnosed, we try to educate them about the likely expenses down the road to help identify potential problems. In my experience, when patients contact us saying they cannot afford one thing, it is usually just the tip of the iceberg.”
For example, PAF assisted a 62-year-old woman with breast cancer who was insured, but she was having difficulty scheduling her needed mastectomy because of outstanding medical bills. She was living on Social Security disability payments, and her insurance did not cover surgeries, scans or tests. The woman received a bill for $50,000 that included the cost of previous care and several office visits. By negotiating with the hospital and the providers, the PAF case manager was able to reduce the bill to a total of $950 and also facilitate the scheduling of her mastectomy.
Suffering in silence
For Bilicki, one of her personal goals is to encourage patients to consider the financial aspect of their cancer care before they decide to pursue a particular form of treatment. “Nobody wants to talk about their financial state, and I think far too often patients suffer in silence rather than saying that they are having trouble with copayments, so what I do is proactively tell them about some of the resources,” Bilicki said. “Just because they have insurance does not mean they will have resources to afford the costs, so I empower all patients right off the bat to proactively seek out assistance if they need it.”
After patients have been diagnosed with cancer, Bilicki encourages them to learn about the resources at the American Cancer Society, which has patient navigators trained to help people connect with financial resources. She also tells them about a group called Patient Resource LLC, which has a website and a patient magazine that includes national, state and local resources available for financial assistance. In the case of the woman with endometrial cancer who could not afford a medication that was not covered by her insurance, Bilicki helped her apply for the drug manufacturer’s patient assistance program. Based on her income and medical necessity, she qualified for full assistance. She was on the medication for 15 months, and, despite her initial grim prognosis, the cancer has been in remission for the past five years.
“I can always remember the tears and fear in their eyes when I first meet patients, and each time it feels like I’ve won the lottery when I help them secure the treatment they need, and they start smiling again,” Bilicki said. “Part of my big mission for my colleagues is to advocate for these patients so they do not miss out on options that can change their lives.”
A little help can mean a lot
Point the way for patients who need assistance financing cancer treatments, by seeking resources such as the following:
• PatientAdvocate.org — Provides sources for copay assistance and answers questions about disability and insurance processes • PatientResource.com — Features information on different types of cancer, newsletters and financial and advocacy resources • CureToday.com — Provides an extensive list of national resources for advocacy, financial and pharmaceutical assistance • RxOutreach.org — A nonprofit organization that helps low-income families who cannot afford the medication they need • CDFund.org — Chronic Disease Fund — A nonprofit organization that helps patients obtain lifesaving medications For a list of drug assistance programs from pharmaceutical companies, visit Cancersupportivecare.com/drug_assistance.html.
The single-use timer that will wholesale for about a dollar is designed to make a nurse’s life easier.In medicine, time isn't just money: it can mean the difference between life and death. Clot-busters must be given in the first hour of arrival in a hectic emergency room. Intravenous medications can spoil, and catheters that overstay their welcome invite infection.
The advance of technology translates into heavier, more complex workloads for the nurses on the frontlines of medical care. To ease the burden, biomedical engineer Sarah Sandock has invented a simple, inexpensive, single-use timer that could be worn like a wristwatch to tell a nurse when to administer a drug or unhook a medical device.
Sandock is a Milwaukee native who received bachelor's and master's degrees in biomedical engineering from Univ. of Wisconsin-Madison (UW-Madison) in 2012 and 2013.
In her first year at the UW, Sandock was inspired by bacteria that had been genetically engineered to create rhythmic pulses. She immediately thought of timing: "I thought, this is cool; you could grow your own timer instead of manufacturing one!"
When that brainstorm seemed impractical, she started thinking of possible uses for a cheap, disposable timer. "As I was in biomedical engineering, and most of my relatives are practicing physicians, I looked for applications in the health care space," she says.
Sandock participated in a Three-day Startup event, a program designed as a dry run for would-be entrepreneurs in Madison, and began to get serious about actually starting a company. She used a disposable-timer business as an academic exercise in two business school classes, "and halfway through, I became passionate about the project."
Sandock knew that one person's passion is nowhere near enough to start a company. Would nurses appreciate the idea? Would they ask for the timer and use it? She says the answer came pretty quickly when she followed nurses working in Madison, Milwaukee and elsewhere: "They asked me, 'Do you have them now? We can use them now.'"
The many technological innovations in health care have countless benefits, but Sandock contends they have not made nurses' lives easier. "They see this as a product that is geared to help them with their problems."
Sandock has working prototypes in hand and is focusing on getting the timers manufactured. She sees two key categories of initial demand for her product: medicines that must be delivered within a certain time window, and medical devices that must be removed or changed at a specific time point, often to avoid a hospital-acquired infection.
Sandock has one patent application filed but is reluctant to specify what technology underlies the inexpensive timers. Her company, Dock Technologies, has an office at the Madison co-working space 100state, and is working with people in the medical field to refine the displays for maximum utility in specific uses.
Dock Technologies has attracted investment from the Weinert Applied Ventures in Entrepreneurship (WAVE) class at the Wisconsin School of Business, several Wisconsin physicians and the National Collegiate Innovators and Inventors Alliance.
A single-use medical device that wholesales for about a dollar has to be accurate. And beyond that, the standard is pretty simple, Sandock says. "Does it save time? Does it make a nurse's life easier?"
A new "Charting Nursing's Future" brief from the Robert Wood Johnson Foundation details a series of programs designed by and for nurses that have “spurred the creation of work environments that foster healthcare quality and patient safety” 10 years after a landmark Institute of Medicine report.
The November 2003 IOM report, “Keeping Patients Safe: Transforming the Work Environment of Nurses,” concluded that “the typical work environment of nurses is characterized by many serious threats to patient safety.” The IOM offered a series of specific recommendations about how hospitals and other institutions needed to change to reduce the number of healthcare errors. Taken together, the recommendations constituted a fundamental transformation of nurses’ work environments.
The IOM report found that hospitals and other healthcare organizations did a poor job of managing the high-risk nature of the healthcare enterprise. Accidents were too common, and management practices did little to create a culture of safety.
“We’ve made important gains in the past decade, but we have a lot more work to do,” Maryjoan D. Ladden, RN, PhD, FAAN, senior program officer at RWJF, said in a news release. “Some of the changes needed are systemic and will require collaboration among nurses, doctors, educators, policymakers, patients and others.
“But nurses also have a critical responsibility to transform their individual workplaces, asserting leadership at the unit level and beyond to help identify and solve problems that affect patient safety.”
Among the initiatives highlighted in the brief, “Ten Years After Keeping Patients Safe: Have Nurses’ Work Environments Been Transformed?”:
• Transforming Care at the Bedside. The RWJF-backed TCAB initiative, developed in collaboration with the Institute for Healthcare Improvement, seeks to empower frontline nurses to address quality and safety issues on their units, in contrast with more common, top-down efforts. Evaluations of the program point to fewer injuries from patient falls, lower readmission rates and net financial gains.
• Quality and Safety Education for Nurses. Also backed by RWJF, QSEN seeks to improve patient safety by helping prepare thousands of nursing school faculty to integrate quality and safety competencies into nursing school curricula at the undergraduate and graduate levels.
• Nurse-patient policies. In some jurisdictions, policymakers have addressed patient safety through nurse staffing policies, focusing both on nurse-patient ratios and on the composition of the nursing workforce. To date, California is the only state to establish a limit on the number of patients a nurse may be assigned to care for in acute care hospitals. Other jurisdictions have policies intended to encourage lower ratios. Research on the impact of such efforts on patient safety has been mixed to date.
In addition, the IOM’s 2010 “Future of Nursing: Leading Change, Advancing Health” report gave new impetus to efforts to increase the share of nurses with baccalaureate degrees or higher, and various institutions have begun to address that recommendation through hiring requirements, tuition-reimbursement policies and more.
• Disruptive behavior on the job. Professional discourtesy and other disruptive behavior in the workplace is another barrier to patient safety, particularly given the growing importance of teamwork and collaboration. Noting the consequences of poor behavior can be “monumental when patients’ lives are at stake,” the brief highlights programs at Vanderbilt University Medical Center in Nashville, Tenn., and Johns Hopkins Hospital in Baltimore designed to deter such problems.
A blueprint for change
The CNF brief goes on to cite a series of initiatives by government agencies, professional associations, the public service sector and credentialing organizations, all designed to advance patient safety and transform nurses’ work environments toward that end. It concludes with an “emerging blueprint for change” that urges providers, policymakers, and educators to follow through on:
• Monitoring nurse staffing and ensuring that all healthcare settings are adequately staffed with appropriately educated, licensed and certified personnel;
• Creating institutional cultures that foster professionalism and curb disruptions;
• Harnessing nurse leadership at all levels of administration and governance; and
• Educating the current and future workforce to work in teams and communicate better across the health professions.
The brief also provides policymakers, healthcare organizations, educators and consumers with a listing of available tools to help in their efforts.
This issue of “Charting Nursing’s Future” is a publication of RWJF created in collaboration with the George Washington University School of Nursing in Washington, D.C.
When Karlina Zambrano was about 13 weeks pregnant, she found a leaflet in her medicaid packet for a program called the Nurse-Family Partnership. The nationwide program would provide a nurse at no charge, who would come to her house weekly or bi-monthly throughout the first two years of her baby’s life. The visits would provide education and resources.
“I thought ‘Why not? It’s more information, more research,’” said Zambrano, now mom to 4-month-old Anthony, who she says is the “most adorable chunk of awesomeness ever.”
Zambrano soon met nurse Gloria Bugarin, who has worked for the Partnership through the YWCA of Metropolitan Dallas since 2006.
The Partnership is provided to low income women pregnant with their first child. The goal is to improve pregnancy outcomes, child health and increase “economic self-sufficiency.”
“A lot of it, even though we’re all RNs, is social work,” Bugarin said. She sees many clients who are in abusive relationships and tries to help them find resources to be safe. Others need help finding work or transportation to jobs. And on top of that, they rely on Bugarin to help point them to good child care.
Together, Bugarin helped Zambrano, 27, work on getting her blood pressure down. After Anthony was born (healthy and to term), Bugarin helped her with breastfeeding, which Zambrano desperately wanted to do, but found difficult. And when Zambrano, who had a stack of library books about pregnancy on her table when Bugarin first met her, felt like she wasn’t doing enough “attachment parenting,” Bugarin gave her advice [any new mom could use.]ECHO “To calm me down, she said if you think about a day, you feed him often, you’re there when he cries, you change him. You do everything to make him happy. Each thing you do builds trust in you from him.”
Bugarin took this job after 14 years as an elementary school nurse. She saw a need for parenting programs and early interventions, thinking that could help the countless children she saw coming into school with behavioral problems and developmental delays.
She feels like there are success stories for sure.
In one instance recently, she had a mom who was in a violent relationship with the baby’s father. Bugarin provided her with resources and at at some point after, that mom decided it was time to leave. She’s now living with family and has a job watching her cousin’s 6-month-old so she can keep her baby with her during the day. “From our visits and her desire to have a better life for herself and her baby, she’s making better choices,” Bugarin said.
For Zambrano and her husband, the visits have been incredibly helpful as they don’t really have family nearby. “There was somebody there who would talk to me and answer my questions, who might not be in an extreme rush,” she said. “I can really just open up and speak to her.”
Bugarin will be at the organization’s annual Mother’s Day celebration later this week. Previous graduates will be there, and more than 300 have already RSVP’d, she said excitedly. She is also proud to say she has two clients graduating (which happens when their children turn two) soon. “It is exciting, but also a little sad because we develop a relationship,” she said. One is still continuing with her education and is in the 10th grade. The other is going to college to become a social worker.
“I’m hoping she’ll volunteer or apply to work” with us, Bugarin said.
It should be noted: If you buy a Boppy pillow at Babies R Us during the month of May, the Boppy Company will donate 5 percent of its proceeds in the form of pillows to the Nurse-Family Partnership. The company has donated nearly 10,000 pillows over the last five years. You can also donate directly here until May 11:www.DonateToNFP.org
Because the Affordable Care Act requires that individual and small-group plans include coverage for mental health care that is comparable to that for general medical care, many analysts expect the demand for mental health services to dramatically increase over the next few years. In California, finding enough mental health providers to meet the demand will be a challenge, as the federal Health Resources and Services Administration has identified 128 Mental Health Professional Shortage Areas in our state.
After documenting vacancy rates for mental health professionals in county-operated mental health programs and state hospitals, the California Mental Health Planning Council suggested that one way to address this shortage is to increase the recruitment and preparation of psychiatric/mental health nurse practitioners (PMHNPs) as primary mental health providers. Given the direction of health care service delivery in the US, perhaps the most important advantage PMHNPs offer is that they are educated in an integrative practice model that stresses connections between physical and mental health and emphasizes health promotion. This is especially critical in public mental health settings, where many patients struggle to get to any health care appointment, much less multiple appointments with multiple providers.
Using PMHNPs to address shortages and increase access to care in public mental health settings, however, faces a number of challenges. To help understand and address these challenges, we are collaborating with the California Institute for Mental Health (CiMH) to conduct a Robert Wood Johnson Foundation-funded study that will include case studies in five California counties with a history of using PMHNPs. The aim is to document best practices, identify unnecessary restrictions on NP practice and formulate strategies to remove these restrictions. By the conclusion of the study in 2015, we hope to have evidence-based information for key stakeholders – from public mental health care systems to state policymakers – about how PMHNPs can help increase access to mental health services in the state.
One thing the study will allow us to do is examine in more detail presumed barriers that have emerged both anecdotally and from prior research. To begin with, just as with primary care, there is a need to rapidly fill the pipeline by incentivizing existing and future students to work in public mental health. That’s why beginning in 2009, California’s Mental Health Services Act began funding educational stipends to PMHNP students at three schools of nursing, including UC San Francisco. The stipend requires that students “pay back” their stipend by working in a public mental health setting for the equivalent of a year of service for each year of stipend funding.
That’s a fine start, but many of our colleagues across the state are concerned that scope-of-practice laws and the lack of good practice models for PMHNPs in California appear to undermine the effort to prime the pipeline.
For example, UCSF School of Nursing faculty member Aaron Miller was educated in Oregon and says that the biggest difference between the two states is that, “In Oregon, NPs can practice without a collaborative agreement with a physician…and the scope-of-practice law in Oregon contains an explicit description of the NP’s scope of practice: assessment, diagnosis, creation of plan and treatment.” By contrast, he says, in California NPs must always have a collaborative agreement in place with a supervising physician, and in every setting they have to devise agreed-upon standardized procedures that define what the NP can do – essentially, the scope of practice. Moreover, at present, practice models in the state do not facilitate optimal billing for PMHNP services.
Ebony Anderson, one of our former stipend students, says these limitations have dampened her willingness to strike out into independent practice as a psychiatric mental health nurse practitioner.
Thus, even as many in the state recognize that NPs can provide high-quality care and organizations are starting to utilize NPs’ full scope of practice, a number of factors may be erecting unnecessary obstacles to meeting the mental health needs of many Californians – especially in areas already short on qualified providers. These factors include reimbursement challenges, the effort involved in defining acceptable scope for each setting and finding physicians willing to provide NPs with the mandated level of supervision – and bill for services under their provider numbers, if appropriate.
Our charge, among other things, is to examine how and to what degree these factors affect the state’s ability to meet expected growth in demand for mental health services. Such research is the lifeblood of policy change. Our hope is that the results of our work will enable the state to fully leverage an educational system that is training PMHNPs to deliver outstanding care but, at least at the moment, sending them into a health care system that is not yet taking full advantage of their strengths.
To mark National Nurses Week, we asked new RNs about what every nurse needs to succeed. Five nurses from the DC/Maryland/Virginia region, all with two years or less of experience, answered the following question: What qualities or characteristics are most important to possess as a nurse, and why?
Hannah Hanscom, RN, BSN, CPN, clinical nurse, surgical care unit, Children’s National Health System, Washington, D.C.
As a pediatric nurse, I believe there is no one quality or characteristic that is most important to being a nurse. Nurses must be passionate about caring for children and their families and be able to think critically and on their feet. But we also must be able to communicate effectively and efficiently with the family, patient and interdisciplinary team. We must be compassionate and able to stay calm when escalating care is needed. Although there is no one quality or characteristic that is most important for nursing, having a passion for the field, for caring for those in need, for educating others and for continuing your own education ties all the other qualities together. Nursing is not just a job or a career. Being a pediatric nurse is in many ways a calling; it is something that comes from the heart and is a lifestyle you must be passionate about.
Shannon Levin, RN, med/surg unit, Novant Health Haymarket Medical Center, Gainesville, Va.
Nursing is more complex than ever. Nurses are managing new technologies, constant advances in best practices and more and more patients with multiple morbidities. Nurses must be organized multitaskers, with quick critical thinking skills. But a nurse who possesses empathy for his or her patients is the best kind of nurse. Nurses with genuine empathy understand that we often see patients and their families at one of the most difficult times. Most of our patients are experiencing some level of physical and emotional pain and often feel anxious and fearful about their hospitalization. An empathic nurse cares enough to identify and understand his or her patient’s feelings. The nurse listens to his or her patient’s medical history and current symptoms and eases his or her fear by explaining the need for hospitalization, the plan of care and ordered procedures. These actions help build trust and ultimately are the foundation of a successful nurse-patient bond and remarkable care.
Rachel Nugent, RN, emergency department, Carroll Hospital Center, Westminster, Md.
It takes many characteristics to be a nurse. I believe the most important characteristics to possess are empathy, compassion, hope, patience and good communication skills. Being empathetic for patients and also for their families shows true compassion. Nurses must give patients a sense of hope when they may be at the lowest point in their lives. Nurses smile, and with that smile, a positive perception is given to patients and their families. Patience with not only yourself, but with patients, family members, doctors and coworkers is a must. Nurses must know when to speak up for themselves or their patients and when to intervene - especially when they suspect something may be wrong. Nurses advocate for their patients when they are in dire need. And, finally, one of the most important parts of communication is that nurses must always be great listeners, even after a long 12 hour shift.
To be successful, flexibility is the single most important attribute a nurse should have. Throughout nursing school you are taught many skills to prepare you. However, there are some things that cannot be taught, yet are essential to becoming a nurse. As with most things in life, having the right balance is equally as important. Being flexible, yet having the ability to stay focused, is critical to ensure you are providing excellent care to your patients.
Mandy Ward, RN, emergency services, Novant Health Prince William Medical Center, Manassas, Va.
There are quite a few qualities that are important to possess as a nurse, but I would have tosay the most important one would be compassion. Compassion is listening to a patient, showing him or her sincere concern, being kind and showing empathy. Our patients look to us to help them when they are most vulnerable. It is up to us to help them when they need it, and we can start by showing them compassion and that we truly care about them. Compassion alone isn’t enough; but, by showing compassion, it makes a big difference for those that we take care of.
While 12-hour weekend shifts for nurses are typical, it’s not common to do it while also attending medical school full-time. But that’s what Mazvita Ethel Simoyi did during her first year at the University of Virginia School of Medicine, commuting every weekend to a hospital in Washington, D.C. to help pay for her education.
Now set to earn her M.D. degree from UVA this month, Simoyi laughed when asked how she endured the relentless schedule of work, schoolwork and commuting.
“I honestly do not know how I did it,” she said. “Necessity makes you rise to the occasion.”
Working Toward a Lifelong Dream
Simoyi knew she wanted to be a doctor from the time she was 5 or 6, when her father, Dr. Mike Simoyi, a general practitioner in Zimbabwe, brought her to his clinic to observe a tubal ligation. “I stood on a stool in the operating room, looking at him make the incision,” she said.
As she got older, she helped direct patients at the clinic where her father worked with her mother Regina, a nurse. The time she spent there deepened her commitment to medicine.
“The patients [at my parents’ clinic] are very, very grateful for the help they receive,” she said. “My father is also very involved in public health, and educating people at a time when HIV and AIDS was beginning to get a lot of attention. That’s why I wanted to be a doctor – so I could help people and share my knowledge with them.”
To continue her path toward becoming a doctor, Simoyi came to the U.S. from Zimbabwe at age 17 to attend college. After beginning as a biology/pre-med major at Butler University, she transferred to Howard University in Washington, D.C., earning a nursing degree in 2007. She went into nursing so she could earn a living while taking the remaining pre-requisite classes for medical school and “ensure that medicine was 100 percent what I wanted to do.”
After three years working as a nurse, she entered UVA’s School of Medicine in 2010. But she wasn’t quite done with nursing.
Full-Time Medical Student, Part-Time Nurse
During her first year as a med student, Simoyi worked weekends on a medical/surgical/oncology inpatient unit at Providence Hospital in Washington, D.C. She would leave Charlottesville around 5 p.m. Thursday or Friday for Washington, staying with her sister Nyasha or friends from Howard University when she wasn’t at work. She would return to Charlottesville around midnight Sunday to get some sleep before waking up at 7 a.m. Monday to begin another week of med school classes.
During her second year as a medical student, she worked part-time in Charlottesville as a hospice nurse. She continued working as a nurse until November 2012, when she was no longer able to work weekends due to her medical school clerkship.
“Time management was what really saved me,” she said.
Her commitment both to her education and her jobs impressed her classmates and faculty. “I was blown away by her work ethic,” said Chad Lane, a member of her medical school class.
As a part-time pharmacist during his time in medical school, Simoyi’s residency adviser, Dr. Shawn Pelletier, knows firsthand how tough her balancing act was. “It’s a lot of work,” he said. “While other people are studying or relaxing, you’re spending time working to pay tuition.”
The intelligent way Simoyi approached her dual responsibilities helped her do both successfully, said her adviser, Dr. Christine Peterson. “She knew exactly what she wanted to do. She’s very grounded and very realistic,” Peterson said. “She found nursing jobs that would mesh with the enormous amount of hours required for her studies.”
Simoyi also believes the extra hours she put in as a nurse helped with her medical school class work. “When I was reading information from a textbook, I could translate it to my patients. It helped solidify the concepts because I could apply it right away instead of waiting two years [to begin my clerkship],” she said.
When Simoyi did a four-week rotation in transplant surgery with Pelletier, he saw that “she already had the textbook answers, had digested that and had moved onto the next step.” In some cases, the only reply Pelletier had to her questions was: “That’s a good question – we’re trying to figure out the answer to that.”
While her nursing work left her less time to spend outside of class with her fellow students, Simoyi said she very much enjoyed her time at UVA. Her classmates were very welcoming and inclusive, and she appreciated that she was part of a large group of students who had taken non-traditional journeys to medical school.
“I was happy to see how many people had taken different paths, like IT and working as financial advisers,” she said.
Giving Back to Zimbabwe
This summer, Simoyi will begin a surgical residency at Baystate Medical Center in Springfield, Massachusetts. She chose surgery because she likes to work with her hands, figure out what’s wrong with a patient and quickly see results.
“You fix an artery, and you get to see the effects of your work immediately,” she said.
While she’s not sure whether she will end up practicing medicine in the U.S. or Zimbabwe, Simoyi definitely wants to give back to Zimbabwe. “I want to have some impact in Zimbabwe, even if I’m not there physically. I want to do something to make health care better, either in education or through standards of care for patients.”
Her classmates and teacher believe she is primed to succeed in whatever challenge she takes on next.
“Surgery is physically demanding and it requires mental toughness,” classmate Pranay Sinha said. “You have to be tough to go through what she has gone through.”
National Nurses Week traditionally is a time to recognize the crucial contributions registered nurses (RN) make to individuals' health and the U.S. health care system; this year, it's also a time to sound a note of urgency about the future, as projections signal the need to fill about 1.1 million RN jobs by 2022.
The 2014 National Nurses Week theme is "Nurses: Leading the Way," emphasizing nurses' roles in improving the quality of health care; participating as key members of collaborative, performance-based health care teams; and continually advocating to ensure patients remain the focal point of health care. National Nurses Week takes place May 6-12, ending on the birthday of Florence Nightingale, the founder of modern nursing.
"All nurses are leaders, whether they are in direct patient care, administrative roles, or meeting consumers' needs in new roles such as care coordinators or wellness coaches," said ANA President Karen A. Daley, PhD, RN, FAAN. "This week, we acknowledge nurses' vast contributions, as well as the need to develop the nursing workforce to meet our growing needs and improve the health of the nation."
As nurses assume more leadership roles in a system that is transforming its focus to emphasize primary care, prevention, wellness, chronic disease management, and coordination of care, a confluence of factors is driving the need for a huge increase in the number of RNs. About 11 million individuals have gained better access to health care through private health insurance marketplaces and the expansion of Medicaid under the Affordable Care Act; Baby Boomers are projected to swell Medicare rolls by 50 percent by 2025; and 53 percent of nurses are over age 50 and nearing retirement, according to a National Council of State Boards of Nursing survey.
The U.S. Bureau of Labor Statistics projects 1.1 million jobs for nurses between 2012 and 2022 – more than 500,000 each for newly created jobs and replacements for retiring nurses. Registered nurse is ranked second in projected new job growth among all occupations from 2012 to 2022, with 527,000 new jobs, according to the Bureau of Labor Statistics. To achieve that level of growth, ANA recommends four actions:
Increase funding for federal Nursing Workforce Development Programs (known as Title VIII of the Public Health Service Act, which marks its 50th anniversary this year). Funding generally has stayed level in recent years for these programs that assist in educating, training, and placing new nurses in areas of need.
Recruit more nursing professors and increase incentives. Nursing faculty salaries generally are lower than what many faculty members could earn in clinical practice (an average of $68,640 compared to more than $91,000 for nurse practitioners). Many nursing professors also are nearing retirement age – nearly 3 of 4 are over age 50 – and will need to be replaced.
Ensure an adequate number of clinical training sites so nursing students can fulfill educational requirements.
Encourage hospitals and other employers to hire new nursing graduates now to benefit from mentoring from experienced RNs, and to mitigate the impact of the projected exodus of seasoned RNs in the coming years.
Wherever health care is provided, a nurse is likely to be there.
Tuesday marks the start of National Nurses Week, an annual opportunity for communities to recognize the full range of nurses’ contributions. This year’s theme, “Nurses: Leading the Way,” recognizes nurses as leaders in the field.
Nurses are being honored as leaders who improve the quality of health care. Nurses practice in diverse roles, such as clinicians, administrators, researchers, educators and policymakers.
Lizeth Martinez, a registered nurse at Valley Baptist Medical Center in Harlingen, said every nurse is different.
“We each have our scope of practice and me, personally, I always try to be there for my patients,” Martinez said. “From what I have seen I am very fortunate to work with the people that I do.”
Martinez, who was born and raised in Brownsville, is currently working on a graduate degree in nursing at the University of Texas at Brownsville and should be finished by next year.
She said that in the two and half years that she’s been a nurse she has gained a lot of experience.
“I love being a nurse,” Martinez said. “As nurses we care in a different way, in a compassionate and holistic manner promoting health and healing.”
However, being a nurse is not without its challenges, said Martinez, who mainly works with wound care and diabetes patients.
“I think the most challenging thing about being a nurse is the emotional aspect because we see a lot of patients that are chronically ill,” Martinez said.
Garett Byrd, a pediatric registered nurse at Harlingen Medical Center, has worked in the nursing field for nine years.
Byrd, whose parents were nurses, said the profession has changed a lot during that time.
“Over the years I’ve noticed an increase in accountability and technology,” Byrd said. “The nursing profession has moved towards a more evidenced based practice. Were not doing things just to do them, were researching and going by the research.”
He said the community should keep one thing in mind.
“The community needs to remember that we’re human beings too, and we’re here because we care,” Byrd said.
Both Martinez and Byrd said nurses are leaders in the health profession.
“I think we are leaders. The profession is so amazing because there are so many things you can do, so many fields you can go into,” Martinez said.
“As nurses were able to provide and coordinate care and think those aspects of leadership position.”
Karen A. Daley, president of the American Nurses Association, agrees.
“All nurses are leaders, whether they are in direct patient care, administrative roles or meeting consumers’ needs in new roles such as care coordinators or wellness coaches,” Daley said.
“This week, we acknowledge nurses’ vast contributions and how they are leading the way in improving health care and ultimately, the health of the nation.”
Nurses are leading initiatives to increase access to care and improve outcomes by focusing on primary care, prevention, wellness, chronic disease management and the coordination of care among health care providers and settings.
These are areas in which nurses excel given their education and experience, the ANA said.
According to the ANA, nursing is the nation’s largest health care profession, with nearly 3 million employed professionals and is projected to grow faster than all other occupations.
The federal government projects that more than 1 million new registered nurses will be needed by 2022 to fill new jobs and replace nurses who leave the profession.
Demand for nursing care will grow rapidly as Baby Boomers swell Medicare enrollment by 50 percent by 2025 and millions of individuals obtain new or better access to care under the health care reform law, the ANA said.
National Nurses Day is celebrated annually on May 6th to raise awareness of the important role nurses play in society. This day also marks the beginning of National Nurses Week, which ends on May 12th, the birthday of Florence Nightingale. Nightingale is considered the founder of professional nursing due to her pioneering work during the Crimean War of 1853-1856 and her establishment of the first secular nursing school in London.
Here are five ways to say 'thank you' to a nurse who has touched you or a loved one this year:
Say it with caffeine: Nurses work long and late hours. A gift card to a coffee shop is a practical and much appreciated token of thanks.
Say it out loud, Facebook style: Consider a big social media shout-out on your Facebook page. Tag your nurse friends, but make it public to all.
Say it with soles: On their feet for long shifts, the quest for the perfect pair of nursing shoes can be eased with a gift certificate to a local or online nursing supply store.
Say it with a letter: Handwritten thank-you notes are still an excellent way to share your feelings and boost the recipient's day.
Say it with food: Every workplace enjoys a thoughtful basket of food from a grateful customer. Just make sure to include enough for the team.
As a nursing student, I have had the privilege of observing many nurses in different units; pediatrics, maternity, the burn unit, hospice, medical surgical, ICU, CCU, wound rounds, and psychiatry. I’ve realized from these experiences that school nurses are by far the most unappreciated and de-valued. As I gathered information on the role of school nurses, and shadowed an elementary school nurse for my senior capstone project, I discovered the challenges faced by school nurses.
Contrary to popular belief, the school nurse’s role is critical to the well-being of students’ health and academic achievements. The scope of practice for the school nurse includes supervision of school health policies and procedures; promotion of health education; health services; competence of interventions; facilitation of health care screenings; making referrals to other healthcare providers; patient advocacy and maintenance of the appropriate environment to promote health. This role requires the nurse to be knowledgeable and competent in various skills and interventions. School nurses provide care, support and teaching for diabetes, asthma, allergies, seizures, obesity, mental health, and immunizations to all students (Beshears & Ermer, 2013). The role of the school nurse as defined by the National Association of School Nurses is as follows: “a specialized practice of professional nursing that advances the well-being, academic success and lifelong achievement and health of students” (Board, Bushmiaer, Davis-Alldritt, Fekaris, Morgitan, Murphy &Yow, 2011).
Clearly, it is not just about Band-Aids and ice packs but still 25% of US schools have no nurse present and 16% of students have a medical condition that warrants a skilled professional (Taliaferro, 2008). One in every 400 children under 20 years is diagnosed with diabetes; 10% of students nationwide have asthma; prevalence of school allergies have increased drastically; 45,000 students are diagnosed with seizures each year; obesity rate has tripled among children 6 to 11 years, and more than tripled for children 12 to 19; and one in five students have mental health issues (Beshears & Ermer, 2013).
Despite having laws allowing disabled children to attend school, increasing the workload on the nurses, there are no laws that mandate a nurse to student ratio. The national recommendation for nurse to student ratio is 1:750 but on average some nurses are responsible for up to 4,000 students (Resha, 2010). Nwabuzor (2007) mentioned that parents and stakeholders cannot truly advocate for more school nurses because most of them do not comprehend the role, responsibilities, and advantages of having a school nurse. The major reason for the school nurse shortage is the lack of legislation on school nursing; not enough funding, and no laws forcing schools to hire nurses. Therefore, many educational facilities have opted to hire unlicensed assistive personnel (UAP) instead.
Yes, it is likely more cost effective to hire UAP’s instead of Registered Nurses but that does not make it acceptable. It is my belief that we have different titles and scopes of practice for a reason. I find it mind boggling that some schools do not have school nurses. How is it that some parents are comfortable with sending their children to a school without a nurse? Is it that they don’t inquire about the presence of a school nurse? Or could it be that maybe they assume that every school has a full-time nurse? I wonder if some parents are aware of the nurse to student ratio at their child’s school. Yes, there are budget cuts due to many reasons but why do these schools say they don’t have enough funding to hire a school nurse but they have six assistant coaches for any one of the sports? So yet my question remains unanswered: what is the priority?
References
Beshears, V., & Ermer, P. (2013). SCHOOL NURSING: It's Not What You Think!. Arkansas
Nwabuzor, O. (2007, February). Legislative: "Shortage of Nurses: The School Nursing Experience." Online Journal of Issues in Nursing Vol12 No 2. doi:10.3912/OJIN.Vol12No02LegCol01
Resha, C., (2010, May 31) "Delegation in the School Setting: Is it a Safe Practice?" OJIN: The
Online Journal of Issues in Nursing Vol. 15, No. 2, Manuscript 5. doi:
Nursing continues to be one of the fastest-growing occupations in the nation, as nurses make up the majority of the health care industry workforce. In fact, recent projections from a January 2014 report published in the Bureau of Labor Statistics (BLS) Occupational Outlook Handbook estimate the job growth to be 19 percent faster than the average occupation through 2022.
Besides a strong job market, a degree in nursing can be even more rewarding than you may think. A nurse usually has a flexible schedule and the option to work in a variety of establishments, from hospitals to schools, home care facilities and even government agencies. Few professions can provide the same number of options in terms of where to work, areas to specialize in, or degrees to use. The range of nursing specialties is almost as varied as the personalities of the nurses themselves. So no matter what kind of person you are, you’ll have a place in nursing.
However, the industry has changed over the years and this has led to a higher demand of registered nurses. Patient treatments have become more complicated, and with an increased workload, nurse positions require even more critical thinking skills.
Brenda McAllister, the national director of nursing of the Brown Mackie College system of schools, knows first-hand how the industry has changed. "I have watched the industry grow over the years as nurses become more involved than just taking vital signs, giving medications and bathing patients,” she says. “There is a more team-oriented approach which has developed in hospitals, and this naturally makes it a more rewarding career option. As a result, more and more nursing programs are in demand.”
Nurses must be able to work through problems that don't have a standard cookie-cutter solution. If a life-threatening problem occurs, the nurse must take action within their scope of practice to save a patient. Nurses must have the ability to think on their feet and assure patient safety.
On the other hand, nurses continue to go the extra mile to help their patients. Many people, especially the elderly, are reluctant to take medicine prescribed by a doctor other than their regular doctor. "Nurses will sometimes even call a patient's regular doctor to explain their current health care needs," McAllister says. "Usually a word from that trusted source will help the patient comply. It’s an additional step, but all the more rewarding when you help a patient out.”
In addition, there are a lot of things a nurse can do other than work at a hospital. In fact, not all aspects of nursing require physical, hands-on care. One employment option, which appeals to those who don't necessarily want to touch every patient physically, is to become a care manager or care coordinator. This position involves managing outpatient care to make sure needs are met and health is maintained when a patient leaves a medical facility.
The home health care coordinator's job is broadly based on patient education. Good health assessment skills and good nursing skills are necessary elements of care. These skills, plus teaching skills, continue to help keep the patient as independent as possible.
Another example would be a care coordinator's position at an insurance company, which is similar to one employed by a hospital. They work with an eye toward keeping treatment aspects in line with guidelines. A knowledge base is essential to perform the job. One must be able to be a manager, have a broad understanding of the body and a scientific background.
Even with attractive career options and expanding nursing programs, there is still a growing nursing shortage. Higher complexity of care, a growing geriatric population, expanding health and disease prevention services, and many other conditions regarding individual health demand more qualified nurses to fill an increasing variety of positions. So if this is a path you choose to follow, research your options and determine which fields and programs meet your needs to have a rewarding career in nursing.
Q. I have been a bedside nurse for over 25 years and love my career. Both of my daughters have also gone into nursing. What are the career options for us? I don’t think I’ll be bedside much longer and what do recent grads have to look forward to?
A. The outlook for all health care professionals is very good as long as you are open to working in many environments. Hospitals, nursing homes, home health and insurance companies are among the industries interested in speaking to nursing professionals and other health service providers. The OOH (Occupational Outlook Handbook) projects a 19 percent growth rate for nurses between 2012 and 2022 due to an increase in the interest in preventative care, an increase in chronic conditions and the baby boomers need for health care in the future.
I consulted Kathy Lind, Staffing Manger for Boston Children’s Hospital, to get more information on options for experienced nurses who may not want to stay bedside. “Nurses with significant experience who are ready to leave the bedside and who are not ready to retire have several options. There are roles that focus on care coordination or clinical documentation. These positions require the expertise of a seasoned nurse and can be great options for nurses looking to transition.”
The market for new nursing graduates looking for bedside hospital nursing roles is highly competitive. More experienced nurses are staying in these roles longer and the number of new grad hires has decreased. Networking your way into these hospitals continues to be one of the best ways to connect and be the first to learn of available opportunities. Recent graduates should talk to faculty and alumni of their nursing programs to build a network and to build out LinkedIn contacts.
Lind comments, ”For recent graduates, it’s important to remember that you may not land your first choice as your first job. The best thing you can do is keep your options open and maintain a positive attitude. If you have the chance to speak with a recruiter or hiring manager, approach the conversation as an opportunity to build a professional relationship and ask if it’s OK to contact them occasionally for updates via email. You can keep them updated on the status of your boards and if you’ve accepted a position elsewhere.”
Your first job will most likely not be your last job. Many staffing managers would agree with Lind’s comment: “You may need to consider extending your job search beyond your initial clinical specialty and geographic preferences. The best thing you can do as a new graduate RN is to secure a position and gain one to two years of valuable experience. At that point you can begin to think about applying for that dream job!”
By Janice Petrella Lynch, RN, MSN, and Tracey Boyd
In healthcare facilities, it takes a network of teammates to ensure the optimal health of patients who receive care. The most successful teams are those who acknowledge each other’s strengths and work together accordingly where there are weaknesses, inspiring one another along the way.
In honor of National Nurses Week, we asked nurses in New York and New Jersey to share the many ways in which their colleagues inspire them in their everyday lives to be better nurses, better teammates and better people. On the next few pages, we share their thought-provoking and heartfelt responses with you.
Benjamin Quinones, RN, coordinator of care, MJHS Home Care, Brooklyn, N.Y.
My network of team leaders helped me transition into nursing after 16 years as a paramedic. I didn’t get to be part of patients’ follow-up care or journey back to independence while working as a paramedic.
As part of MJHS Home Care, I see patients one-on-one, but with the support I get from my special colleagues, I’ve never felt alone. Most important, my team leaders have taught me that at the end of the day, it’s all about our patients.
Stephen R. Marrone, RN-BC, Edd, CTN-A, deputy nursing director, SUNY Downstate Medical Center, Brooklyn, N.Y.
When I was a high school volunteer in the ICU of a community hospital in Brooklyn, I watched the nurses care for patients and knew I wanted to be a nurse. As a nurse for more than three decades, I continue to be inspired by nurses every day, individually and collectively.
Individually, I see nurses work tirelessly to provide excellent care during difficult financial times, and I am determined to make sure they have the resources they need to provide safe care. I am inspired when I see younger nurses become leaders on their units and I know I have made a difference.
Several nurses have mentored and provided a springboard for me to elevate my practice and expand my scope of influence. They did so by recognizing potential in me that was hidden from myself. They helped me gain entry into higher levels of practice and a peer group that role-modeled leadership.
When I am having one of those days when I ask myself, “Why do I do this?,” I think of those nurses and the patients we care for and remember that I am privileged to be touched by others and to touch others’ lives every day.
Sylvie Jacobs, RN, BSN, CPAN, postanesthesia care unit, Mount Sinai Hospital, New York City The nurse who remains with me as the most inspiring is Patricia Liang. We worked side by side in the postanesthesia care unit for decades.
She was the go-to resource because she seemed to know what to do in every situation and could impart the information to staff in a kind and supportive way.
Liang was tiny in stature but relayed an enormous, quiet power, always in a respectful way. The new residents got away with nothing when Liang was around. She not only had a seemingly bottomless wealth of knowledge, but she also had an unfailing moral compass. When there was an ethical issue that needed to be resolved, we knew to ask Liang.
She was not a talkative person — she was usually focused on coordinating care — but you somehow felt her support and appreciation for your efforts. I always will remember her for not just being an outstanding nurse, but for also being an outstanding person.
Janice Wright, RN, BSN, staff nurse, 4C med/surg unit, Lutheran Medical Center, Brooklyn, N.Y.
I have been working at Lutheran Medical Center on a med/surg unit for the past four years. I have had the pleasure of working with an extraordinary group of nursing colleagues.
It is hard to single out one particular person because I truly can say my professional life has been enriched and my work ethics validated by each of the nurses with whom I work. I feel empowered and energized in my daily work because of my colleagues.
Mary Farren, RN, MSN, CWOCN, clinical nurse specialist, acute care, VNSNY, Queens, N.Y.
Nearly every morning for the past 10 years, I have been fortunate to have a chat with Marilyn Liota, RN, as we start our day around 7 a.m. Nearly every conversation begins with Liota saying: “Tell me what is good.” From there, we have gone off in many directions. What a way to open a conversation, and what a way to start the day.
I consider myself fortunate to have known Liota, worked under her leadership and guidance, and been a part of the special and historic “Marilyn Liota” years at VNSNY. Liota recently retired and I’m truly happy for her, yet underneath it all, I feel a touch of sadness, too. I will miss her so much.
So typical of a giving soul like hers, Liota’s next steps involve giving generously of herself to help others as a volunteer working with new immigrants for a nonprofit organization called “Literacy Nassau.”
When I think of the most influential person in nursing who has enriched my life, the answer rolls right off my tongue. Her name is Winnie Mele, RN. I have been blessed to work alongside her for 28 years, and still each new day brings a new experience.
Her style of leadership motivates and inspires all who know her to be successful in their careers. She gets out and circulates among the troops. No matter how dark the day, I always can count on her to make it a learning experience without being punitive.
We share the same vision and passion for nursing. There is never a day when she won’t sit and have coffee, share a story, sing a song or just listen. “Every patient, every time” is the mantra she taught me and her staff. I am a better person professionally and spiritually because of this special outstanding woman.
Compassion, honesty, fairness and loyalty are what I have taken from this extraordinary nurse who, throughout my career, has been my role model. Everyone should have someone like Mele in their life. I thank God for her every day.
Nydia White, RN, critical care unit, South Nassau Communities Hospital, Oceanside, N.Y.
I was 21 years old when I was a new RN on a med/surg floor. On that unit there was no such thing as being alone as a nurse — we worked together as a team. It was scary, overwhelming and exciting at the same time.
Lisa Williams, my first nurse manager, did more than just her job. If there was a sick call, she would take a section of patients. If we needed some extra hands, she would give bed baths. Williams exemplified confidence, leadership and teamwork with a touch of color and a twist of enthusiasm that would radiate to her staff.
The quality that amazed me most was her compassion for people. It wasn’t just about your abilities as a nurse; it was about tapping into the kind of person you were and helping you grow. She could sense if something was wrong, take you to the side and support you through the challenge.
Williams’ specialty was to identify a nurse’s potential and mentor her to be a better nurse and a better person. She encouraged me to be the charge nurse and join committees when I didn’t think I was ready, but she assured me I was. Now I am a critical care RN and even host a CCRN review class. I volunteer for many committees. I am a better person and nurse because of Williams, my first nurse manager, mentor and friend.
Erica Zippo, RNC-OB, BSN, C-EFM, staff nurse, labor and delivery, White Plains (N.Y.) Hospital
I was a new graduate nurse when I started working on the labor and delivery unit at White Plains Hospital. In nursing school, we heard that nurses eat their young, so the support, camaraderie and familylike atmosphere I felt on the unit was something I never expected.
My colleagues took me under their wings and enthusiastically shared their knowledge and individual experiences, most of which were things I had not learned in school. When observing my colleagues in action, I learned how to make a patient and his or her family feel comfortable, calm and welcome; how to complete an efficient history and physical while admitting a woman in labor; and how to make the delivery of every baby special despite the paperwork and nursing tasks.
This shared knowledge from my colleagues continues to enrich my professional life and has shaped me into the nurse I am today. My colleagues also have supported me in my personal life through many important moments, such as relationships, break-ups, moves, graduate school, marriage and the birth of my daughter. I am thankful for the positive influences of my strong, intelligent and caring colleagues.
Nurse researcher Linda H. Aiken, RN, PhD, FAAN, FRCN, has published a study that presents the latest in growing body of evidence to suggest a more highly educated nursing workforce saves lives.
“Our research shows that each 10% increase in the proportion of nurses in a hospital with a bachelor’s degree is associated with a 7% decline in mortality following common surgery,” said Aiken, professor of nursing and sociology and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania in Philadelphia. “More education, and particularly university education, enhances critical thinking. Professional nurses are called upon to quickly synthesize a large amount of clinical information about acutely ill patients, process this information in the context of scientific evidence, reach evidence-based conclusions, communicate salient information and their conclusions to physicians, and act in the absence of a physician at the bedside, which is most of the time.”
Aiken said the study, published Feb. 26 on the website of The Lancet, was designed to account for other possible explanations for lower mortality, including patient-to-nurse ratios, presence of physicians, availability of high technology and how sick the patients are on admission.
“After taking into account these other factors, nurses’ education is a very important factor in patient outcomes,” Aiken said.
The researchers combed through more than 420,000 patient records of discharged patients following common surgeries, such as knee replacements, appendectomies and vascular procedures.
This isn’t the first such finding for Aiken.
“In U.S. research, we have established a causal linkage between better-educated nurses and patient deaths by studying hospitals over time, showing that hospitals that actually increase their hiring of bachelor’s nurses have greater declines in mortality than hospitals that have not increased BSN employment over the same time period,” she said.
American Association of Colleges of Nursing President Jane Kirschling, RN, PhD, FAAN, said the fact Aiken publishes in such high-end journals as the Journal of the American Medical Association and The Lancet shows her findings stand up to rigorous scientific reviews.
The message for associate degree-prepared nurses, according to Kirschling, is to continue their education.
“We’re the largest single group of healthcare providers in the United States, and we’re there 24-7, 365 days a year for the care that’s provided,” Kirschling said. “That’s in hospitals, community settings and long-term care settings. So, we have to make that commitment as a discipline and as professional nurses to continue to expand our knowledge and our critical thinking skills, and we do that through advancing nursing education.”
Donna Meyer, RN, MSN, president, National Organization for Associate Degree Nursing, said that while the N-OADN supports higher-education initiatives in nursing, community colleges are crucial to meet the nursing care needs of the U.S. healthcare system. Community colleges graduate quality nurses representing 60% of the nursing workforce, according to Meyer, who is dean of health sciences at Lewis and Clark Community College in Godfrey, Ill.
“Community colleges provide entry points for students moving into the nursing profession to practice, [and] provide a pathway to higher education and advanced practice, research and faculty positions,” Meyer said. “Many community colleges are embedded in rural and-or medically underserved communities, and without them and the nursing graduates they produce, healthcare provider shortages would continue to impair access to care.”
Meyer said N-OADN is working with the National League for Nursing, AACN and the American Nurses Association to find ways to encourage students to continue their education. A-OADN also is working with the Robert Wood Johnson Foundation’s Future of Nursing: Campaign for Action to support recommendations in the Institute of Medicine report, “The Future of Nursing: Leading Change, Advancing Health.” The study supports the importance of IOM recommendations that 80% of the U.S. nursing workforce be bachelor’s-educated by 2020, Aiken said. Nurses should help their institutions use this strong evidence base to improve nurse staffing adequacy and facilitate the transition to a BSN workforce.
“There are now quite a few large, well-designed studies by different research teams and in different countries documenting the relationship between more BSNs in hospitals and better patient outcomes,” Aiken said. “These studies were mentioned in The Lancet article and include at least multiple studies in the U.S., research in Canada, Belgium, China and now in nine countries in Europe. That is a substantial evidence base, sufficient to guide policy and practice decisions.”
To hospital and other employers, this and other studies show that nursing education really does matter, Kirschling said.
Healthcare stakeholders need to “make the investment in our associate degree-prepared nurses by providing tuition support for them to go back to school … [and] to provide flexibility in the workplace” to allow them to continue their education, Kirschling said.
When Wally Winter, a nurse and retired Air Force lieutenant colonel, boards a plane at Albuquerque International Sunport today, he won’t touch ground for about two days.
When he does, he’ll pick up where he left off a few months ago, nursing those touched by one of the worst typhoons in history, which ravaged the Philippines last November.
Wally Winter is shown at his home in Bernalillo, wearing a T-shirt with the name of the organization for which he volunteers as a nurse, Project Hope. He leaves today for his second tour doing disaster relief nursing in the Philippines. (Adolphe Pierre-Louis/Albuquerque Journal)
The 65-year-old native Oklahoman, who now lives in Bernalillo, spent six weeks volunteering around last year’s Christmas holidays in a poor hospital on an island in the Philippines hit hard by the typhoon, and today he goes back. When he arrives the morning of March 26, he’ll serve two more months on the same island, called Panay, through a Virginia-based nonprofit organization called Project Hope, the same one he served with before.
It sends doctors, nurses, pharmacy technicians and social workers to areas around the world in need of relief.
“I think it brings me closer to God and helps me be more thankful,” said Winter, describing what made him want to serve the first time and then return. “I feel I have been richly rewarded and I’ve really never had any major challenge in life, nothing devastating that I’ve been up against.”
Not so for the people of Tapaz City, located on the island of Panay. It was hard hit by Super Typhoon Haiyan – one of the strongest storms recorded on the planet. It smashed the Philippines on Friday, Nov. 8, killing more than 6,200 people.
A few days later, Winter’s neighbor, also a registered nurse, who is from the Philippines, told him about Project Hope.
“He said, ‘What company is that?’ and he said, ‘I really want to serve. I really want to go,’” recalled Veronica Rodriguez-Jumalon, a surgical care nurse at Presbyterian Hospital who came to the U.S. from Cebu 20 years ago.
Winter sent in his application and was quickly accepted. His two-day journey began Dec. 18 and took him from Albuquerque to Dallas to Japan to Manila to Panay Island. Rodriguez-Jumalon, who spent the holidays with her husband and 17-year-old daughter, joined Winter’s team a month later.
Wally Winter and Veronica Rodriguez-Jumalon, top, at Tapaz District Hospital, taking a report from the local hospitalist and one of the Project Hope physicians. (Courtesy of Wally Winter)
The team consisted of 19 people, most from Massachusetts and California and ranging in age from 25 to 72. Many, including Rodriguez-Jumalon, stayed about three weeks and then had to return to jobs and family. Winter, who is unmarried and retired and does not have children, spent six weeks.
“I tried to simplify my life, so I can walk out the door at the last minute and I’m gone,” he said.
They worked in the 25-bed Tapaz District Hospital, which has broken windows and falling ceilings and no air conditioning. Locals, many who had never before seen a doctor, walked five miles to get care, Winter recalled during an interview in a Northeast Heights coffee shop a few days before his departure.
At the hospital, the team got to work, performing vaccinations, circumcisions and simple surgeries. They also educated more than 25 local health workers about tuberculosis, STDs, hepatitis, infection control and hand-washing techniques.
“At one point, we saw 600 patients in one day,” said Rodriguez-Jumalon. “We’d treat their coughs and colds; we did some wound care, and another doctor from Harvard brought an ultrasound machine … It’s really, really a poor area,” she added. “They had a wheelchair that was made of a garden chair with some tire(s) attached.”
Having survived the typhoon, many also had high blood pressure, she said.
Winter recalled a girl helping her father carry his comatose wife six miles on a hemp hammock to the hospital. The wife was revived with dextrose in the hospital, whose intensive care unit Winter described as a “broken-down little room,” and whose operating room had collapsed five years before.
At night, his team slept on air mattresses, four or five to a bedroom, or outside on the porch. They woke up at 4 a.m. so everyone could shower before heading to the hospital, where, besides caring for patients, they also painted the beds and walls and replaced mattresses.
“I saw how overwhelmed everybody was,” Winter said. “It was like, you don’t even know where to start.” The hospital had no clean water, so sometimes it was re-used, he said. In some parts of the town, there was no electricity, although the hospital did have it.
Tapaz District Hospital had a bed capacity of 25 patients but often took care of 35 or 40 at one time, with beds in the hallways and other spare floor space. (Courtesy of Wally Winter)
His service in Tapaz City seems like a natural extension of his work in the Air Force. His last deployment was to Iraq in 2005, and he oversaw nurses in a trauma center who medically evacuated those who had been hurt. During most of his military career, which took him through Iraq, Kuwait and Afghanistan during times of war and peace, he was an aeromedical evacuation nurse himself. “You saw those poor soldiers, they had no ears, no eyes – they had all been burned off – and you were there to hold their hand, tell them how much they are appreciated. You look at them and it just breaks your heart.”
After retiring from the Air Force, he worked at Rust Presbyterian and taught nursing at Apollo College and Grand Canyon University.
Going to the Philippines was quite a departure. “Project Hope picked that area because no one else wanted it,” he said. “We’d go into the far jungle areas and set up clinics,” intended for those too far away from the hospital, said Winter.
Project Hope pays for their flight – Winter’s ticket cost about $4,000 – housing, and meals, but otherwise doesn’t offer any salary.
A relative of the mayor of the town of Tapaz offered the volunteers a four-bedroom house to stay in. A cook prepared them meals including rice, vegetables mixed with cooked meat, lumpias (similar to eggrolls) and fried bananas. Winter used about $200 of his own money per month for other transportation costs and to buy food for people who had not eaten for days, he said.
Local soldiers escorted his team to the hospital every day because there had been a terrorist threat in the area, Winter said.
This time, Winter will return by himself, and will stay until May 29 in the same house. He will teach nurses some infant care and advance their skills in reading an EKG. He will also assess the work his team did during the first trip.
And, he said, “I’ll probably be able to sleep in the bed this time.”
Jumalon plans to return in June. “It’s not a long-term impact, but at least it makes impact to their lives,” she said of the work they are able to do. “It gives them hope.”
And, she added: “It’s a very rewarding, a very humbling experience as well. It made me realize how lucky we are over here with our health care.”
The following is a script from "The Health Wagon" which aired on April 6, 2014. Scott Pelley is the correspondent. Henry Schuster and Rachael Kun Morehouse, producers.
President Obama announced last week that more than 7 million people have signed up for Obamacare. But what went unsaid is that almost as many people have been left out. Millions of Americans can't afford the new health insurance exchanges. For the sake of those people, Obamacare told the states to expand Medicaid, the government insurance for the very poor. But 24 states declined. So, in those states, nearly five million people are falling into a gap they make too much to qualify as "destitute" for Medicaid, but not enough to buy insurance. We met some of these people when we tagged along in a busted RV called the Health Wagon -- medical mercy for those left out of Obamacare.
The tight folds of the Cumberland Mountains mark the point of western Virginia that splits Kentucky and Tennessee -- the very center of Appalachia -- a land rich in soft coal and hard times. Around Wise County, folks are welcomed by storefronts to remember what life was like before unemployment hit nine percent.
Teresa Gardner: The roads are narrow and windy curves. So it's not easy to drive the bus.
This is Teresa Gardner's territory. She can't be more than 5-foot-4 but she muscles "the bus" through the hollers, deaf to the complaints, of a 13-year-old Winnebago that's left its best miles behind it.
Teresa Gardner: Having problems seeing here.
Scott Pelley: You really can't see.
The wipers are nearly shot and the defroster's out cold.
Scott Pelley: There you go, you can see a little better now. I understand there's a hole in the floorboard here somewhere?
Teresa Gardner: Yes, it's right over there so don't get in that area.
The old truck may be a ruin but like most RVs it's pretty good at discovering America. Gardner and her partner, Paula Meade, are nurse practitioners aboard the Health Wagon, a charity that puts free health care on the road.
[How many patients do we have on the schedule today?
He was going to see what he can free up for us.]
The Health Wagon pulls up in parking lots across six counties in southwestern Virginia.
[Y'all come on in out of the rain.]
It's not long before the waiting room is packed.
[Hello Mr. Hank, how you doing?]
And two exam rooms are full. With advanced degrees in nursing, Gardner and Meade are allowed to diagnose illnesses, write prescriptions order tests and X-rays.
[Stick it out, ahhh.]
On average there are 20 patients a day, that's recently up by 70 percent. The Health Wagon is a small operation that started back in 1980. It runs mostly on federal grants and corporate and private donations.
[Blood pressure a bit high before?
Just when I get aggravated.]
Scott Pelley: Who are these people who come into the van?
Paula Meade: They are people that are in desperate need. They have no insurance and they usually wait, we say, until they are train wrecks. Their blood pressures come in emergency levels. We have blood sugars come in 500, 600s because they can't afford their insulin.
Scott Pelley: But why do they not see a doctor or a nurse before they become, as you call it, train wrecks?
Paula Meade: Because they don't have any money. They don't have money to pay for labs. They don't have money to go to an ER and these are very proud people. They, you know, you go to the ER, you get a $3,500 bill. And then what do you do? You're given a prescription, you can't fill it. That's why they're train wrecks. They have nowhere else to go.
Glenda Moore had nowhere to go but the ER when the pain in her leg became unbearable. Her job at McDonald's, making biscuits, didn't include insurance that she could afford.
Glenda Moore: The only doctor that would see me-- you had to have $114 upfront just to be seen.
Scott Pelley: What does $114 mean to your monthly budget?
Glenda Moore: Oh my gosh. That's half of my weekly pay. I make $7.80 an hour. My paycheck was about after taxes about $475 every two weeks.
The pain was from a blood clot. She needed Lovenox, a clot buster that cost about $500 for a full treatment.
[Paula Meade: Was she on Lovenox when she was discharged from the hospital?]
Paula Meade got the call from the ER, which didn't want to bear the cost. The Health Wagon had the drug for free and there was no charge for some stern medical advice.
Paula Meade: You are going to die if you don't quit smoking and it could be within a week. You need to stop now! OK?
She took the advice to stop smoking and took Lovenox but one day she felt so bad she went back to the ER.
Glenda Moore: And they did a CAT Scan and an X-ray and found the blood clot had went to my lung. But they also saw another mass on my lung. And then transported me to a bigger hospital. They found the lesions in my brain, so I was diagnosed with stage IV lung cancer and brain cancer.
Scott Pelley: What are the doctors telling you?
Glenda Moore: I start my treatment on Monday, the brain radiation, and he seemed very, I mean he seemed optimistic.
Scott Pelley: Are you hopeful?
Glenda Moore: I am. I have been. I don't know, I just feel very hopeful.
Hope, especially when the odds are long, has always been essential to survival in Appalachia. The recovery from the Great Recession hasn't arrived. In coal these days they just take the top of the mountain and you don't need many men for that. Around here a thousand were laid off in the last two years. Twelve percent of the folks don't have enough to eat. And we met them waiting for their number at Zion Family Ministries Church where a charity called Feeding America was handing out just enough to get through a week -- if you stretch. 1,654 lined up -- a parking lot of possibilities for the Health Wagon, Gardner and Meade. They've known these people and each other most their lives.
Scott Pelley: You've been together since 8th grade?
Paula Meade: Eighth grade. Yes.
Scott Pelley: Why do you do this work?
Paula Meade: Because somebody has to. You know, there's people here, you know, we always, we had dreams. We wanted to move away from here. We all, you know, we did. And then we come back and we saw the need. And actually there's a vulnerable population here that's different from the rest of America. I mean there are people, you can replicate this. But we're kind of forgotten. There's no one here to take care of 'em but us.
These patients would be taken care of in the 26 states that expanded Medicaid under Obamacare. The federal government pays the extra cost to the states for three years but Virginia and the others that opted out fear that the cost in the future could bankrupt them. So the health wagon patients we met have fallen through this untended gap.
[Do you have insurance?
No ma'am.]
Scott Pelley: Have any of you tried to sign up for the president's health insurance plan?
Voices: No--
Scott Pelley: Why not?
Brittany Phipps: I can't afford it.
Sissy Cantrell: I can't either.
Sissy Cantrell was laid off from a head start center. She's been suffering from migraines and seizures.
[I cry for no reason at all. OK.
Have you been seeing a counselor?
No.
OK.]
She came away from the Health Wagon with medication.
[I did want to ask you....]
Brittany Phipps works more than 50 hours a week, but that's two part-time jobs so there's no insurance for her diabetes.
Scott Pelley: So you're getting your insulin through the Health Wagon?
Brittany Phipps: I am now. Yeah.
Scott Pelley: And if that wasn't available, where would you get the insulin?
Brittany Phipps: I don't know.
Walter Laney's diabetes blinded him in one eye and threatens the other. The Health Wagon stabilized him and set him up with a specialist.
[Hey Walter, this is Dr. Isaacs, how's it going?
Pretty good.
How've you're sugars been?
OK.]
Walter Laney: They got my blood sugars back under control. Before this year, I was in the hospital three, four times and this year, I ain't been in none since I've been seeing them. If it hadn't a been for them, I don't think I'd be here today.
Outside the church where they were handing out food we met Dr. Joe Smiddy, a lung specialist who's the Health Wagon's volunteer medical director.
Joe Smiddy: This is a Third World country of diabetes, hypertension, lung cancer, and COPD.
Dr. Smiddy drives a second Health Wagon, a tractor-trailer X-ray lab.
Scott Pelley: I guess they taught you something about radiology and all of that in medical school. Did they teach you how to drive an 18-wheeler?
Joe Smiddy: I did have to go to tractor-trailer school. And it took a long time.
Scott Pelley: Was that harder than medical school in some ways?
Joe Smiddy: It was very difficult to get anyone to insure a doctor to drive a tractor-trailer. The insurance companies didn't believe me.
His X-ray screen is a window on chronic, untreated disease including black lung from the mines.
Joe Smiddy: We've seen coal workers pneumoconiosis, emphysema, COPD, enlarged hearts. There's 15 of the 26 had significant abnormalities here today.
Scott Pelley: Just today?
Joe Smiddy: Just today.
Scott Pelley: But when they leave your Health Wagon, they still don't have health insurance. How do they get treated for these things that you're finding?
Joe Smiddy: We negotiate. We can talk to the hospital system. We don't leave any patient unattended. We raise money for them.
Scott Pelley: You find a way.
Joe Smiddy: We will find a way.
They found a way to get Glenda Moore radiation for her brain cancer. But she'd been a smoker for 25 years. And she died three months after our interview.
Scott Pelley: You don't like this idea of receiving charity?
Glenda Moore: No. Oh, I hate it. My dad was in the military. And when he was diagnosed with cancer, he was taken care of. And I don't know, I just always assumed, you know, that's how it would work.
Scott Pelley: Do you think things would've been different if you'd had an opportunity to go to a doctor more often?
Glenda Moore: Oh, definitely. I know it would be different.
The outreach to all the people like Glenda Moore costs the Health Wagon about a million and a half dollars a year, a third of that is from those federal grants, and the rest from donations. Doctors volunteer and pharmaceutical companies donate drugs. But when we were with them...
[We got no electricity on the health side.]
...they sure could have used a new truck battery.
[There goes.Yay! ]
Teresa Gardner: Can we give you all a free flu shot for helping us?
Man: Need a free flu shot, Beaver? Nope. Ok.
Teresa Gardner and Paula Meade apply for grants. And travel to churches praying for donations and passing the plate.
Scott Pelley: Are there days you say to yourself, "I can't do this anymore."
Paula Meade: Oh, every day. Not every day. I shouldn't say every day. There are a lot of days you get frustrated because we're writing grants till 10:00 at night. We're begging for money. And you're almost in tears because we're like, "OK, what are we gonna do," because I've got a family too. It gets frustrating, it gets hard.
Scott Pelley: It's enough to wear you out, Teresa.
Teresa Gardner: We're pretty beat down by the end of the day on most days really. But we do get more out of it then we ever give.
Paula Meade: When you look at it practically, you think, "What in the world am I thinking?" But then I have that one patient that may come in and say, "Couldn't bring you anything, can't pay anything but here's a quilt I wanna give you." And I mean when they do that and they're so heartfelt and you just-- and they put their arms around you, "I don't know what I'd do without you..."
[You're doing a lot better.]
Paula Meade: It lets you think, "OK, I was put here for a purpose."
Teresa Gardner: And you can do it another day.
[You're a blessing to us.
Well thank you all. You're blessing us. ]
Teresa Gardner: It's them and that's what touches our heart.
This week in Virginia, there is a crisis at the capital where the new Democratic governor is demanding Medicaid expansion from the Republican House. But neither side will budge and now there's a threat of a government shutdown in that state. There's no shutting down the Health Wagon though. Gardner and Meade have raised money for a new truck and they hope to get it on the road in the spring.
When it comes to the cost and quality of hospital care, nurse tenure and teamwork matters. Patients get the best care when they are treated in units that are staffed by nurses who have extensive experience in their current job, according to a study from researchers at Columbia University School of Nursing and Columbia Business School. The study was published in the current issue of the American Economics Journal: Applied Economics.
The review of more than 900,000 patient admissions over four years at hospitals in the Veterans Administration Healthcare System is the largest study of its kind to link nurse staffing to patient outcomes. The researchers analyzed payroll records for each nurse and medical records for each patient to see how changes in nurse staffing impacted the length of stay for patients. Because length of stay is increased by delays in delivery of appropriate care and errors in care delivery, a shorter length of stay indicates that the hospital provided better treatment. At the same time, a shorter length of stay also makes care more cost-effective. The study found that a one-year increase in the average tenure of RNs on a hospital unit was associated with a 1.3 percent decrease in length of stay.
"Reducing length of stay is the holy grail of hospital management because it means patients are getting higher quality, more cost-effective care," says senior study author Patricia Stone, PhD, RN, FAAN, Centennial Professor of Health Policy at Columbia Nursing. "When the same team of nurses works together over the years, the nurses develop a rhythm and routines that lead to more efficient care. Hospitals need to keep this in mind when making staffing decisions – disrupting the balance of a team can make quality go down and costs go up."
While many hospitals rely on temporary staffing agencies at least some of the time to fill RN vacancies, the study found that it's more cost-effective for hospitals to pay staff RNs overtime to work more hours on their unit. RNs working overtime resulted in shorter lengths of stay than hours worked by nurses hired from staffing agencies, the study found.
Nursing skill also mattered, the study found. Length of stay decreased more in response to staffing by RNs than by unlicensed assistive personnel. Furthermore, the study showed that length of stay increased when a team of RNs was disrupted by the absence of an experienced member or the addition of a new member.
"This rigorous econometric analysis of nurse staffing shows that hospital chief executives should be considering policies to retain the most experienced nurses and create a work environment that encourages nurses to remain on their current units," says the senior economist on the study team, Ann Bartel, PhD, Merrill Lynch Professor of Workforce Transformation at Columbia Business School.
The researchers used the VA's Personnel and Accounting Integrated Data for information on each nurse's age, education, prior experience, VA hire date, start date at the current VA facility, and start date for the current unit at that facility. To assess patient outcomes, the researchers used the VA's Patient Treatment File for information on each patient including dates of admission and discharge for each unit and for the overall hospitalization, as well as age and diagnoses. The final sample accounts for 90 percent of all acute care stays in the VA system for the fiscal years 2003 to 2006.
More information: The paper is titled: "Human Capital and Productivity in a Team Environment: Evidence from the Healthcare Sector," and it was published in April 2014.
The National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care(the National CLAS Standards) are intended to advance health equity, improve quality, and help eliminate health care disparities by providing a blueprint for individuals and health and health care organizations to implement culturally and linguistically appropriate services. Adoption of these Standards will help advance better health and health care in the United States.
Health Equity & Culturally and Linguistically Appropriate Services (CLAS): How Are They Connected?
Health inequities in our nation are well documented, and the provision of culturally and linguistically appropriate services (CLAS) is one strategy to help eliminate health inequities. By tailoring services to an individual's culture and language preference, health professionals can help bring about positive health outcomes for diverse populations. The provision of health care services that are respectful of and responsive to the health beliefs, practices and needs of diverse patients can help close the gap in health care outcomes. The pursuit of health equity must remain at the forefront of our efforts; we must always remember that dignity and quality of care are rights of all and not the privileges of a few.
What is the history of the National CLAS Standards?
In 2000, the Office of Minority Health published the first National Standards for Culturally and Linguistically Appropriate Services in Health Care (National CLAS Standards), which provided a framework for all health care organizations to best serve the nation’s increasingly diverse communities. In fall of 2010, the Office of Minority Health launched the National CLAS Standards Enhancement Initiative in order to revise the Standards to reflect the past decade’s advancements, expand their scope, and improve their clarity to ensure understanding and implementation. With the enhancement initiative, the National CLAS Standards will continue into the next decade as the cornerstone for advancing health equity through culturally and linguistically appropriate services.
Legislating CLAS
State agencies have embraced the importance of cultural and linguistic competency in the decade since the initial publication of the National CLAS Standards. A number of states have proposed or passed legislation pertaining to cultural competency training for one or more segments of their state’s health professionals. At least six states have moved to mandate some form of cultural and linguistic competency for either all or a component of its health care workforce. Access the Legislating CLAS map.
The Bureau of Labor Statistics predicts that 526,800 new nursing jobs will need to be filled between 2012 – 2022. Many new nurses will need to be educated to fulfill that need, and as nurses continue to grow in number and importance to the medical field, the need for skilled nurse educators also goes up.
Entering the field of nursing is also challenging. Increasing competition for the most desirable jobs for practicing nurses and nurse educators can be intimidating. It is important for young nurses, especially students, to have role models that remind them how valuable and rewarding a nursing career can be. This list, presented in no particular order, is not intended as a ranking of these individuals. It is simply meant to honor 100 dedicated nurse educators who have succeeded in carving out a place for themselves in the changing nursing landscape.
Jacqueline Dunbar-Jacob PhD, RN, FAAN – Dean and Distinguished Service Professor of Nursing Professor of Psychology
Dr. Dunbar-Jacob is Dean and Distinguished Service Professor of Nursing at the University of Pittsburgh School Of Nursing. Since 1984, she has been a member of the faculty at University of Pittsburgh. Her primary teaching is primarily at the doctoral level and advisor to a number of doctoral students.
>University: University of Pittsburgh >More Details: Online Bio
Angelo Alonzo, PhD – Research Scientist Professor
Prior to joining the Yale University School of Nursing as a Research Scientist, Dr. Alonzo held an appointment in the Department of Sociology at Ohio State University and was a research sociologist at the National Heart, Lung and Blood Institute of the NIH. At Ohio State University he taught courses in medical sociology, symbolic interactionism and introductory sociology.
>University: Yale University >More Details: Online Bio
Rose O. Sherman-Professor
Rose O. Sherman is a professor at Florida Atlantic University and also the Director of the Nursing Leadership Institute, but has spent the majority of her career as part of leadership in a variety of Veterans Affairs medical centers. Additionally, she’s published many times a year in some of the most prominent nursing publications from around the world.
>University: Florida Atlantic University- Christine E. Lynn College of Nursing >More Details: Online Bio
Bobbie Berkowitz, PhD, RN, CNAA,FAAN- Dean and Professor
Bobbie Berkowitz is a professor of health policy and management at Columbia University in NYC. She also serves as senior vice president of the Columbia University Medical Center.
>University: Columbia University >More Details: Online Bio
Ida Androwich, PhD, RN, BC, FAAN – Professor of Nursing
Dr. Ida Androwich focuses her research on optimizing technology to improve nursing care. She has received several hundreds of thousands of dollars in grant money to collect data from hospitals and health groups to carry out this research and make the lives of patients better, as well as improve patient-nurse relationships better.
>University: Loyola university Chicago >More Details: Online Bio
Jeanne M. Geiger-Brown, PhD, RN, FAAN – Assistant Dean of Research, RES Professor,FCH
Jeanne Geiger-Brown teaches at the University of Maryland School of Nursing, primarily teaching Philosophy of Science courses. Her writing has been published in dozens of professional nursing and medical journals on topics such as working environments, nursing work schedules, and nurse performance.
>University: University of Maryland-Baltimore >More Details: Online Bio
Kathryn E. Artnak, PhD, RN, MA, CNS, CNE
Kathryn Artnak is a professor of nursing at Angelo State University. Her current courses include health policy, theory, and ethics, and her personal research includes work in subjects such as global initiatives in nursing, advanced care planning in certain populations, and clinical ethics.
>University: Angelo State University >More Details: Online Bio
Karen S. Kauffman, PhD, CRNP-BC – Chair and Associate Professor, FCH
Karen Kauffman is a chair and associate professor at the University of Maryland. She earned her PhD in Nursing in 1992, and has been conducting research and writing in the nursing community since then. She has been on several committees and planning boards, most centered on the care, treatment and study of Alzheimer’s disease.
>University: University of Maryland-Baltimore >More Details: Online Bio
Mary Louise Fleming, RN, PhD – Professor & Academic Coordinator
Mary Louise Fleming works at the School of Nursing at the University of California. She is academic Coordinator, associate clinical professor, and director of Nursing & Health Systems. She also focuses her research on improving care and services for the aging population with an emphasis on leadership in nursing homes and long term care settings.
>University: University of California – San Francisco >More Details: Online Bio
Mary E. Kerr, PhD, RN, FAAN – Dean of Frances Payne Bolton School of Nursing and Professor
Mary Kerr is an extremely accomplished nurse out of Cleveland, Ohio, serving as both the Dean of the Frances Payne Bolton School of Nursing and May L. Wykle Endowed professor. Her nursing interests include critical care nursing and neoscience nursing.
>University: Case Western Reserve University >More Details: Online Bio
Peter I. Buerhaus, PhD,RN, FAAN – Valere Potter Distinguised Professor of Nursing
Peter Buerhaus is a professor of nursing at Vanderbilt University, as well as the Director at the Center for Interdisciplinary Health Workforce Studies. His professional research has included developing, testing and refining nurse measures of care, assessing patient views of nurse practitioners and primary care physicians through national surveys, and understanding employment and earnings in the nurse labor market.
>University: Vanderbilt University >More Details: Online Bio
Said K. Abusalem, PhD, RN – Assistant Professor
Said Abusalem has presenting and published dozens of papers on dozens of topics, including home healthcare and healthcare ethics. He is a member of several professional memberships in both the US and Gaza and teachers regularly on pediatrics and home health.
>University: University of Louisville >More Details: Online Bio
Debra J. Barksdale, PhD, FNP-BC, ANP-BC, CNE, FAANP, FAAN – Associate Professor & Director, Doctor of Nursing Practice Program
Dr. Debra J. Barksdale is an Associate Professor and Director of the DNP program at the University of North Carolina at Chapel Hill. She was one of 19 members appointed to the 21 member Board of Governors for the new Patient-Centered Outcomes Research Institute (PCORI) by the U.S. Government Accountability Office under the Obama Administration, and was the only nurse appointed to the board.
>University: University of North Carolina – Chapel Hill >More Details: Online Bio
Susan M. Adams, PhD, RN, PMHNP, FAANP – Professor of Nursing and Director of Psychiatric Mental Health Nurse Practitioner Program
Susan Adams has been honored with several awards in nursing and education since 2004, including Sigma Theta Tau International Rising Star in Research award, the Tennessee Nurses Association Excellence in Nursing Award, and the International Nurses Society on Addictions, Excellence in Education award. She is a professor of nursing at Vanderbilt University and the Director Psychiatric Mental Health Nurse Practitioner Program.
>University: Vanderbilt University >More Details: Online Bio
Tamara BLAND- MSN, RN – Professor
Tamara Bland is an instructor at Resurrection University, College of Nursing. With a professional specialty in adult health and gastroenterology nursing, she currently teaches Adult Health, Health Assessment and Foundations of Nursing.
>University: Resurrection University >More Details: Online Bio
Yea-Jyh Chen-Assistant Professor
Yea-Jyh Chen is an Assistant Professor at the College of Nursing at Kent State University in Ohio. With a Master’s of Science in Nursing, she is able to teach advanced health classes and research methods in nursing.
>University: Kent State University >More Details: Online Bio
Aline Davis,RN & MSN – Nursing Professor
Aline Davis teaches nursing courses at Lakeview College of Nursing. While she previously worked as an RN in two hospital settings, she currently teaches courses in pediatrics, nursing foundations, and clinical skills.
>University: Lakeview College of Nursing
Martha Swartz, PhD, RN, CPNP, FAAN – Professor of Nursing and Primary Care Division Chair
Yale University’s Dr. Martha Swartz is a Professor of Nursing and is the Primary Care Division Chair in the School of Nursing. She’s held numerous positions of regard in her nursing education career and has publishes a good amount of articles looking to address problems in research methods.
>University: Yale University >More Details: Online Bio
Berry S. Anderson, PhD, RN – Assistant Professor
Assistant Professor in the College of Nursing and Research Scientist in the Brain Stimulation Laboratory at the University of South Carolina, Berry Anderson conducts research focused on the use of brain stimulation technologies to understand brain function and treat psychiatric disorders. He has authored or co-authored over 30 peer-reviewed articles and collaborated on more than 40 clinical research trials, and is a member of the American Psychiatric Nursing Association.
>University: Medical University of South Carolina >More Details: Online Bio
Karen Bankston, PhD, MSN, FACHE – Associate Dean and Professor of Clnical Practice
Karen Bankston is associate dean of clinical practice, partnership, and community engagement at the College of Nursing at the University of Cincinnati. With years of leadership experience across academics, she is responsible for developing and maintaining partnerships and collaborations with nursing and other disciplines to provide leading-edge clinical experiences for students
>University: University of Cincinnati >More Details: Online Bio
Betsy Anderson, Instructor of Nursing
Betsy Anderson is an Instructor of Nursing at Lincoln Memorial University in Tennessee. While she currently teaches nursing for a mental health setting, her experience is primarily as a nurse in the army, emergency rooms, and in psychiatric nursing.
>University: Lincoln Memorial University Caylor School of Nursing >More Details: Online Bio
Jeanette O. Andrews, PhD, RN, FNP, FAAN – Dean and Professor College of Nursing
Dr. Andrews has extensive nursing graduate and interprofessional teaching experiences. She has developed and taught clinical courses for nurse practitioner and Doctor of Nursing Practice (DNP) programs to include pathophysiology, pharmacology, health assessment, and clinical preceptorships.
>University: University of South Carolina >More Details: Online Bio
Charles D. "Chad" Rogers, MSN, RN – Assistant Professor
Chad Rogers has a Master’s of Science in Nursing and is a faculty member at Morehead, teaching nursing programs. His clinical interests include correctional nursing, critical care nursing and emergency nursing, and he has worked in the critical care setting in two area hospitals.
>University: Morehead State University >More Details: Online Bio
Karen Plager, PhD, RN, FNP-BC, Professor
At Northern Arizona University, Karen Plager teaches courses such as Health assessment and Family Primary Health Care Practicum. She has also worked as a family nurse practitioner and conducts research on the possible development of community-based primary health care project.
>University: Northern Arizona University >More Details: Online Bio
Elaine J. Amella, PhD, RN, FAAN – Professor
Dr. Elaine Amella is a Professor in the College of Nursing, at the Medical University of South Carolina. She was previously on faculty at New York University and the University of Arizona. She is also Regional Editor for North America for the Journal of Clinical Nursing, and is on the editorial boards of the Journal of Gerontological Nursing, Geriatric Nursing, and the Journal of Nutrition, Health and Aging.
>University: Medical University of South Carolina >More Details: Online Bio
Mary Ellen Burke-Clinical Assistant Professor
Mary Ellen Burke is a Clinical Assistant Professor at the University of Massachusetts and uses her 10+ years of teaching and mentoring experience to help shape nurses that pass through the school. Having worked firsthand as an RN at the highly regarded St. Peter’s Medical Center, she has built up an impressive resume that equips her with the best teaching abilities.
>University: UMass Amherst >More Details: Online Bio
Carol Lynch, MSN, RN – Nursing Chair
Triton College is a small school out of River Forest, Illinois. There, nursing students can learn the basics of nursing and healthcare to earn an Associate Applied Science degree, and later go on for their BSN at a 4-year school. Carol Lynch has her MSN degree and is an RN, and she works at Triton College as the Associate Degree Nursing Chair.
>University: Triton College
Patricia E. Adams-Graves, M.D., B.S. – Associate Professor
As an Associate Professor of Medicine, Patricia E. Adams-Graves is an integral part of The University of Tennessee’s Health Science Center and has a written a number of pieces for publications. With a rich background in working on sickle cell disease, her work is highly regarded.
>University: The University of Tennessee >More Details: Online Bio
Ruth A. Anderson, PhD, MSN, MA, RN, FAAN – Professor of Nursing
Ruth A. Anderson is a Virginia Stone Professor of Nursing, as well as a Senior Fellow at the Duke University Center for Aging and Human Development. Dr. Anderson focuses much of her research and time on improving the management of nursing homes and has been an innovator on research techniques for understanding the problems faced in these scenarios.
>University: Duke University >More Details: Online Bio
Katherine K. Chappell, MSN, APRN, CPNP
Katherine K. Chappell is the Medical Exam Provider for the Child Advocacy Center of Aiken, focusing on supporting abused children through evaluations. Additionally, she works as the Head of Nursing/First Aid Staff at Camp Wonder Hands, a camp that specializes in working with hard-of-hearing and deaf children.
>University: University of South Carolina >More Details: Online Bio
Sue P. Heiney
Dr. Sue P. Heiney works at the University of South Carolina and has experience in numerous clinical settings, while also maintaining support groups that have international renown. Additionally, she has a seemingly endless list of publications she has worked on, along with research studies, and more.
>University: University of South Carolina >More Details: Online Bio
Melissa Batchelor-Aselage, PhD, RN-BC, FNP-BC
Dr. Melissa Batchelor-Aselage is a member of the Duke University School of Nursing and received the Faculty of the Year Award while still teaching at the University of North Carolina Wilmington’s School of Nursing. Since coming to Duke, she’s also been awarded the National Hartford Centers of Gerontological Nursing Excellence Claire M. Fagin Scholarship for 2012-2014.
>University: Duke University >More Details: Online Bio
Chastity Osborn – RN, MSN
Chastity Osborn teaches at Lakeview College of Nursing and is currently pursuing her Doctorate in Nursing Practice. She’s connected to a number of notable institutions including the American Organization of Nurse Executives.
>University: Lakeview College of Nursing >More Details: Online Bio
Annette De Vito Dabbs, PhD, RN, FAAN – Professor and Department Chair
Annette De Vito Dabbs has been teaching nursing for over ten years, specifically in the areas of ethics, technology, and mixed-methods research. Within the University of Pittsburgh School of Nursing where she currently works, she has served on several committees including PhD Council, Planning & Budget, Academic Integrity, and Evaluation Steering.
>University: University of Pittsburgh >More Details: Online Bio
Judith Gedney Baggs, PhD, R.N., F.A.A.N. – Distinguised Professor
Judith Baggs is the Elizabeth N. Gray Distinguished Professor and the Oregon Health & Science University. Her current research interests include ICU and nursing, end of life care and decision making, and quality care.
>University: Oregon Health & Science University >More Details: Online Bio
Barbara J. Burgel, RN, PhD, FAAN – Professor of Clinical Nursing
Barbara Burgel is a professor of clinical nursing at the University of California. Her clinical practice and research program has focused on the occupational health and safety risks facing immigrant workers, including garment workers, hotel room cleaners, and taxi drivers. Her teaching includes studies in the areas of Environmental Health, Clinical Prevention and Population Health, and others.
>University: University of California – San Francisco >More Details: Online Bio
Basia Belza, PhD, RN, FAAN – Professor
At University of Washington, Basia Belza has taught research courses to undergraduate students, theory courses to PhD students, health promotion courses to DNP students, and gerontology courses to all students. She leads the Coordinating Center for the CDC Healthy Aging Research Network, where she conducts research on healthy aging.
>University: University of Washington-Seattle >More Details: Online Bio
Martha Dewey Bergren, DNS, RN, NCSN, FNASN, FASHA – Professor and Director of Advanced Community Health
Martha Dewey Bergren is the Director of the Advanced Community Health Program at the University of Illinois at Chicago. She also currently teaches courses including Evidence Based Practice Nursing, Health Promotion Theory, and others. During her years of practice and teaching, she has received a dozen awards and fellowships related to nursing and leadership.
>University: University of Illinois – Chicago >More Details: Online Bio
Carmella M. Moran, PhD, RN – Director School of Nursing, Associate Professor of Nursing
Carmella Moran is the director of nursing at the School of Nursing at Aurora University. She has served on several committees throughout Illinois including Illinois Nurse Practice Act Task Force and Kane County Health Department Advisory Board.
>University: Aurora University >More Details: Online Bio
Daniel D. Cline, PhD and RN – Assistant Professor
Assistant Professor Daniel Cline works and conducts research at University of Colorado. He has clinical experience in critical care and emergency nursing. He is also a consultant and faculty member on the National League for Nursing's (NLN) Advancing Care Excellence for Seniors (ACES) Project.
>University: University of Colorado-Denver >More Details: Online Bio
Deborah A. Gross, DNSc, RN – Professor of Nursing
Deborah Gross graduated with her Doctorate in Nursing in 1983 and is an assistant professor at Rush University College of Nursing. Her research areas include Behavior and Behavior Mechanisms and Psychological Phenomena and Processes. She has been serving as chair of the Department of Women's and Children's Health since February 2004.
>University: Rush University >More Details: Online Bio
Bill Cody, PhD, RN, CNE, FAAN
Bill Cody is a professor nursing and the director of nursing at DePaul University in Chicago. Some of his distinguished awards include American Nurses Foundation Scholar, Hunter College Hall of Fame, and Luther Christman Award American Assembly of Men in Nursing.
>University: DePaul University >More Details: Online Bio
Holly Powell Kennedy, CNM, PhD, FACNM, FAAN – Executive Deputy Dean & Helen Varney Professor of Midwifery
Holly Powell Kennedy is the Executive Deputy Dean & Helen Varney Professor of Midwifery at the Yale Graduate School of Nursing. She is also the She is Past-President of the American College of Nurse-Midwives and the first person to be appointed as the Varney Professor of Midwifery at Yale.
>University: Yale University >More Details: Online Bio
Beth N. Bolick,DNP, CPNP-AC, PPCNP-BC, CCRN – Nursing Professor
Beth Bolick is a professor as well as the coordinator of the Acute Care Pediatric Nurse Practitioner Program at Rush University. She received her own DNP from Rush and is currently in the Women Children and Family Nursing department.
>University: Rush University >More Details: Online Bio
Charles A. Vacchiano, PhD, CRNA – Professor
Dr. Vacchiano joined the faculty at the Duke University School of Nursing in 2008. Before that, he spent 26 years in the U.S. Navy as a practicing nurse anesthetist, educator, and researcher. He was named the American Association of Nurse Anesthetist Researcher of the Year in 2007.
>University: Duke University >More Details: Online Bio
Linda Flynn, PhD, RN, FAAN – Professor and Associate Dean for Academic Programs
Linda Flynn is a professor and associate dean for academic programs at the College of Nursing at the University of Colorado. She is a past recipient of the Governor's Merit Award for excellence in research and the C.A.R.E. Award from the New Jersey State Nurses Association. She was inducted as a Fellow in the American Academy of Nursing in 2009.
>University: University of Colorado-Denver >More Details: Online Bio
Linda Phillips, PhD,RN,FAAN
At the UCLA School of Nursing, Linda Phillips is the section chair of the Acute and Chronic Health Sciences. She has taught graduate level courses on gerontology; research methods including developing and testing instrumentation for nursing research, community-based research and grounded theory; and research seminars focusing on the development of research proposals. She has also been published in journals and research papers on elder care and geriatric nursing since 1981.
>University: UCLA School of Nursing >More Details: Online Bio
Dr. Bertha Lane Davis – Professor
Dr. Bertha Lane Davis is currently a professor and director of the Nurse Educator Track and the PhD in Nursing program at Hampton University School of Nursing. She is also a retired Lieutenant Colonel in the United States Army Reserve Nurse Corps.
>University: Hampton University School of Nursing >More Details: Online Bio
Jeanne Alhusen, PhD, CRNP, RN
Jeanne Alhusen is an assistant professor at Johns Hopkins School of Nursing and conducts research in the Department of Community-Public Health. She has developed a program of research in understanding the biological and psychological underpinnings of maternal attachment and its influence on early childhood outcomes.
>University: Johns Hopkins School of Nursing >More Details: Online Bio
Janet L. Larson, PhD, RN, FAAN – Professor and Division Chair
At the University of Michigan, Dr. Larson mentors students in her research laboratory and regularly teaches research seminars for graduate students as well as lectures on topics of respiratory physiology and respiratory pathophysiology at the undergraduate and graduate level. She is also the Division Chair of her department.
>University: University of Michigan – Ann Arbor >More Details: Online Bio
Carol Fowler Durham, EdD, RN, ANEF – Clinical Professor & Director, CERC
Carol Fowler Durham is a clinical professor and director at the School of Nursing at the University of North Carolina. Dr. Durham has been involved in Quality and Safety Education for Nurses (QSEN) as a core faculty since its beginning. She received the Nurse Educator of the Year from the North Carolina Nurses Association in 2005.
>University: University of North Carolina – Chapel Hill >More Details: Online Bio
Demetrius Abshire, MSN, RN, ACNS-BC – Nursing Professor
Demetrius Abshire joined the College of Nursing as part-time faculty in 2009 and currently teaches the Foundations for Professional Nursing course. He has also worked as a nurse in the neurosurgical ICU and in rehabilitation.
>University: University of Kentucky College of Nursing >More Details: Online Bio
Mustafa K. Dabbous, PhD., MS, BS – Professor
Mustafa Dabbous is a professor at the University of Tennessee Health Science Center. He has several publications printed, many about immunizations and biochemistry, including “Binding and subcellular distribution of cyclosporine in human fibroblasts” and “Role of saliva and salivary components as modulators of bleaching agent toxicity to human gingival fibroblasts in vitro.”
>University: The University of Tennessee >More Details: Online Bio
Mary Byrne, PhD, DNP, MPH, CPNP – Stone Foundation and Elise D. Fish Professor of Health Care for the Underserved in Nursing
Mary Byrne teaches at the School of Nursing at Columbia University, with research interests such as pain management for children, early infant and child development, and pediatric HIV-AIDS. She is also the recipient of many awards, including Elected Fellow American Academy of Nursing and the Distinguished Research Scholar Award at the Columbia University School of Nursing.
>University: Columbia University >More Details: Online Bio
Dr. Ruth Ann Belknap-Associate Professor
Ruth Ann Belknap teaches courses such as Culture and Health, Health Issues in the Urban Latino Immigrant Population, and Vulnerable Populations at the Marquette University College of Nursing. She is a member of the Midwest Nursing Research Society, National Association of Hispanic Nurses, Wisconsin Nurses Association/American Nurses Association, and several other professional associations.
>University: Marquette University >More Details: Online Bio
Sandra Gaynor, Associate Professor of Nursing and MS Nursing
Sandra Gaynor is a member of American Organization of Nurse Executives, Illinois Organization of Nurse Leaders, and Center for Ethics and Advocacy. She is an associate professor of nursing at North Park University in Chicago and teaches classes that focus on include human resources, quality initiatives, strategic assessment, budgets, safety and risk management, and current social issues affecting healthcare delivery.
>University: North Park University >More Details: Online Bio
Suzanne G. Leveille, PhD Program Director and Professor, Department of Nursing
Suzanne Leveille is the PhD program direction and a professor in the department of nursing at the University of Massachusetts in Boston. She has an extensive background in gerontological nursing, and is also collaborating on a number of projects involving geriatric physical impairments, the role of neighborhood environment in geriatric falls, and pain management in older adults.
>University: University of Massachusetts Boston >More Details: Online Bio
Stephanie Steiner, MSN, RN, ACNP – Professor and Director of Flight Nursing Program
Stephanie Steiner teaches at the School of Nursing at Case Western Reserve University in Ohio. She is also the director of the Flight Nursing Summer Camp. Her education interests include trauma, critical care transport, and simulation training.
>University: Case Western Reserve University >More Details: Online Bio
Joel G. Anderson, PhD – Assistant Professor of Nursing and Roberts Scholar
Joel G. Anderson is the Assistant Professor of Nursing, while also a Roberts Scholar as a part of the University of Virginia School of Nursing. Interestingly, previous to entering graduate school, he was a manager at two cancer research laboratories. He’s also currently the Research Director at Healing Touch International.
>University: University of Virginia >More Details: Online Bio
Judith Halstead, PhD, RN – Executive Associate Dean for Academic Affairs
Judith Halstead if the Executive Associate Dean for Academic Affairs in the Indiana University School of Nursing. She has a wealth of expert insight into online education and co-edits Teaching in Nursing: A Guide for Faculty.
>University: Indiana University – Purdue University – Indianapolis >More Details: Online Bio
Kim Amer, PhD, RN
Kim Amer is an Associate Professor at DePaul University and does a large amount of work in child and family health. She’s even a member of the Consortium to Lower Obesity in Children in Chicago.
>University: DePaul University >More Details: Online Bio
Kathryn Christiansen, PhD, MA, BSN – Associate Dean and Associate Professor
Kathryn Christiansen is the Associate Dean and an Associate Professor at the University of Illinois at Chicago. She has wide-ranging interests, often working in community health nursing, care coordination and care transitions, among others.
>University: University of Illinois – Chicago >More Details: Online Bio
Kelly M. Bower-Joffe, PhD, MPH, RN, APHN-BC
Kelly M. Bower-Joffe is an Assistant Professor at Johns Hopkins School of Nursing and often looks at substance abuse, uninsured, health literacy, food store availability, obesity, and many other areas. Having attained her doctorate at Johns Hopkins as well, she’s very familiar with the university’s health programs.
>University: Johns Hopkins School of Nursing >More Details: Online Bio
Beth A. Brooks – PhD.,RN & FACHE – President
Beth A. Brooks is the President of Resurrection University and has worked as the Executive Director of the University of Illinois at Chicago’s Institute for Healthcare Innovation. As a graduate of Valparaiso University, she was named one of the 150 most influential people in the university’s history.
>University: Resurrection University >More Details: Online Bio
Edie Barbero, PhD, RN , PMHNP-BC – Assistant Professor of Nursing Coordinator and Psychiatric Mental Health
Dr. Edie Barbero is the Assistant Professor of Nursing at the University of Virginia School of Nursing and is the Coordinator of the Psychiatric Mental-Health Nurse Practitioner Program. The Sigma Theta Tau Honor Society of Nursing has twice recognized her quality of research and even accepted the poster she created on Therapeutic Storytelling for the Biennial Convention.
>University: University of Virginia >More Details: Online Bio
April D. Kidd, BSN, MBA, NEA-BC-Adjunct Instructor
April D. Kidd is an Adjunct Instructor at Hood College where she teaches Community Health Nursing in the BSN Completion Program. Her experience as an Army Community Nurse and currently works to ensure the military health system is aptly equipped to tackle issues resulting from threats, manmade or natural.
>University: Hood College >More Details: Online Bio
Michael E. Galbraith, PhD, RN – Associate Professor of Nursing
Dr. Michael E. Galbraith focuses intently on survivorship and health-related quality of life issues for couples affected by prostate cancer and his research initiatives have been funded by the NIH. Dr. Galbraith also works as a scientific reviewer for journals whose subject matter is men’s health issues.
>University: University of Colorado-Denver >More Details: Online Bio
Marita G. Titler, PhD, RN, FAAN – Professor and Chair, Division of Nursing Business Health Systems
University of Michigan’s Marita G. Titler is the Professor and Chair in the Division of Nursing Business and Health Systems. Her work has garnered accolades and research funding, while she also serves on the NIH and AHRQ study section. Her impressive work keeps a refined focus on health services research, particularly as it is relevant to older adults.
>University: University of Michigan – Ann Arbor >More Details: Online Bio
Patricia Clinton, PhD,RN,ARNP,FAANP – Clinical Professor and Director of Faculty Practice
Patricia Clinton is a Clinical Professor at The University of Iowa where her career of over 30 years has given her increased insight as to how we can address problems such as the skyrocketing cost of health care and various indifferent care systems. She’s also served as Assistant Dean for MSN & DNP Programs, currently working as the Director of Faculty Practice.
>University: University of Iowa >More Details: Online Bio
Rojann Alpers, PhD, RN Associate Professor
Rojann Alpers focuses on research as an Assistant Professor at Arizona State University and has written articles on nursing history, the profession overall, and many more. She’s been awarded numerous nursing education awards, so he work is definitely worth checking out.
>University: ASU College of Nursing & Health Innovation >More Details: Online Bio
Angela M. Allen, RN, BSN, MAT, EdS, EA, PhDc
Angela M. Allen has been awarded an incredibly impressive number of accolades in her time as a Clinical Professor at Arizona State University and continues to make large progress for nursing at the university. Most recently, she was honored with an Association of Rehabilitation Nurses Scholar Award.
>University: ASU College of Nursing & Health Innovation >More Details: Online Bio
Claudia Calle Beal, PhD, MSN
Claudia Calle Beal teaches research, translation science, and ethics as an Assistant Professor in the graduate program. Her work looks at stroke health and has been a huge part to helping better the School of Nursing at Baylor.
>University: Baylor University >More Details: Online Bio
Mohammad Alasagheirin, Assistant Professor of Nursing
As an Assistant Professor of Nursing at Bradley University, Mohammad Alasagheirin works on health-related issues commonly experienced by refugee and immigrants, along with the physical activity of children and their bone growth.
>University: Bradley University >More Details: Online Bio
Theresa Adelman-Mullally, Assistant Professor of Nursing
Theresa Adelman-Mullally is an Assistant Professor of Nursing at Bradley University and teaches Fundamental Nursing Theory and Practicum, as well as classes on substance abuse and mental health. She also has experience working in the US Army Nurse Corp.
>University: Bradley University >More Details: Online Bio
Carol M. Musil, PhD, RN, FAAN – Nursing Professor
Dr. Carol M. Musil is a Marvin E. and Ruth Durr Denekas Professor of Nursing and does extensive work regarding older adults and caregiver status. With an impressive number of published works, there’s no denying how much she has contributed to Case Western Reserve University.
>University: Case Western Reserve University >More Details: Online Bio
Suzanne Bakken, PhD, RN, FAAN, FACMI – Alumni Professor of the School of Nursing and Professor of Biomedical Informatics
Dr. Suzanna Bakken is the Alumni Professor of the School of Nursing and Professor of Biomedical Informatics at Columbia University. She looks thoroughly at HIV/AIDS and her published works and awards signify the value of her work.
>University: Columbia University >More Details: Online Bio
Jeanne Matthews, BS, MS, PhD
Jeanne Matthews is the chair and Assistant Professor of the Department of Nursing, but has previously worked as the chair of the American Public Health Association’s Public Health Nursing Section.
>University: Georgetown University >More Details: Online Bio
Laura Anderko, PhD, RN
Dr. Laura Anderko is an Associate Professor at Georgetown University and has worked on the Environmental Protection Agency’s federal advisory committee, the Children’s Health Protection Advisory Committee. She’s currently active in a handful of notable committees.
>University: Georgetown University >More Details: Online Bio
Marion E. Broome, PhD, RN, FAAN – Dean and Distinguished Professor
Dr. Marion E. Broome is a Distinguished Professor, specifically in Nursing Care, in the School of Nursing at Indiana University. She’s highly regarded in the field and has made incredible contributions throughout her career.
>University: Indiana University – Purdue University – Indianapolis >More Details: Online Bio
Dr. Kim Ferguson, Assistant Professor of Nursing and Assistant Director of the FNP Concentration
Dr. Kim Ferguson is the Assistant Professor of Nursing and the Assistant Director of the FNP Concentration at Lincoln Memorial University. She specializes in areas such as Family Nurse Practitioners, Master of Science courses, child obesity, and rural health and she’s received numerous awards for excellence.
>University: Lincoln Memorial University Caylor School of Nursing >More Details: Online Bio
Shelley F. Conroy, Ed.D., MS, BSN
Dr. Shelley F. Conroy is very active in nursing higher education and works as a Professor and Dean at Baylor University. From leading study abroad trips to working on research endeavors, her experience is hard to match in nursing higher education. To date, she’s been awarded more than $7 million in grants.
>University: Louise Herrington School of Nursing Undergraduate Program >More Details: Online Bio
Vicki Keough, PhD, APRN-BC, ACNP, FAAN – Dean and Professor
Vicki Keough is a Dean and Professor at Loyola University in the Marcella Niehoff School of Nursing. Her published works often include studies on the state of nursing currently. Additionally, she was inducted as a Fellow in the American Academy of Nursing.
>University: Loyola university Chicago >More Details: Online Bio
Deborah Watkins Bruner RN, PhD, FAAN
Deborah Watkins Bruner obtained at Doctorate degree at the University of Pennsylvania with a focus on nursing research and her work has focused on quality of life, patient reported outcomes, symptom management across cancer sites, and more related to cancer. Notably, she was the only nurse to serve as Principal Investigator of one of the National Cancer Institute’s Community Clinical Oncology Programs.
>University: Nell Hodgson Woodruff School of Nursing at Emory University >More Details: Online Bio
Elizabeth J. Corwin RN, PhD
Dr. Elizabeth J. Corwin first worked as a physiologist before becoming a professor and applies her real world experience as a nurse with the rigor of a researcher to create a unique background suited for many situations. Currently, she’s also a Principal Investigator on a $2.4 million dollar award from the NIH.
>University: Nell Hodgson Woodruff School of Nursing at Emory University >More Details: Online Bio
Robin L. Bissinger, Ph.D., APRN, NNP-BC, FAAN – Associate Dean for Academics and Associate Professor
Robin L. Bissinger has made a name for herself in the nursing field as the Associate Dean of Academics in the College of Nursing at the Medical University of South Carolina. She’s incredibly active professionally, also working as the President of the National Certification Corporation and as the Vice-Chair of the Congress on Nursing Practice and Economics, among other organizations she’s active in.
>University: Medical University of South Carolina >More Details: Online Bio
Joyce K. Anastasi
Joyce K. Anastasi works in the NYU College of Nursing as an Independence Foundation Endowed Professor and is the Founding Director of the Division of Special Studies. She’s a leading clinical Scientist in symptom management. With multiple teaching and research awards to her name, she is well accredited in the nursing community.
>University: New York University >More Details: Online Bio
Chrsitine Smith, DNP,MA and BSN – Associate Nursing Professor
Christine Smith is an Associate Nursing Professor helps to train students to work effectively in urban environments that embrace multiple cultures. She teaches at a local shelter teaching health education and invites students to work alongside her.
>University: North Park University >More Details: Online Bio
Shelley Miller, MSN, RN
Shelly Miller is a Professor of Nursing at Oklahoma City Community College and has worked in critical care, focusing on cardiac ICU and open heart recovery. In 1990, she was awarded the Robert A. Watson Cardiovascular Nursing Award and is a member of the Sigma Theta Tau International Nursing Society.
>University: Oklahoma City Community College >More Details: Online Bio
Traci Boren, Professor of Nursing
Traci Boren is a Professor of Nursing in the BADNAP nursing program at Oklahoma City Community College, while simultaneously working as a perioperative nurse. She also spent 8 years working as an Army National Guard medic, so has uniquely suited skills.
>University: Oklahoma City Community College >More Details: Online Bio
Gail M. Houck, PhD, R.N., P.M.H.N.P. – Professor & Program Director for Post-Master DNP
Gail M. Houck is a Professor and Program Director at Oregon Health and Science University. She’s active in publishing articles that analyze various components to the profession, specifically how we can improve the development of children and babies.
>University: Oregon Health & Science University >More Details: Online Bio
Brenda Recchia Jeffers, PhD, RN, Chancellor, Professor
Brenda Recchia Jeffers is a chancellor and professor at St. John’s College, as well as a founding member of Team Illinois, an organization committed to relieving workface shortages. Her notable work in nursing education has placed her on the list, but she’s also recognized for her work at a number of organizations.
>University: St. John’s College >More Details: Online Bio
Kimberly D. Acquaviva, PhD, MSW
Kimberly D. Acquaviva is a tenured Associate Professor at The George Washington University and is also the Director of Faculty Affairs. Dr. Acquaviva has been awarded over $20 million in federal funding and was recently a Fulbright scholar, helping to teach nursing students and physicians in Thailand.
>University: The George Washington University >More Details: Online Bio
Ellen Cram, PhD and RN – Associate Clinical Professor & Assistant Dean
Ellen Cram is an Associate Professor at The University of Iowa and is also the Assistant Dean for Undergraduate and Pre-licensure programs. In 2000, she was recognized as the Outstanding Iowa Nurse Leader of the year and has received other awards.
>University: University of Iowa >More Details: Online Bio
Stephanie Fugate, MSN, ACNP – Nursing Professor
Stephanie Fugate teaches at the University of Kentucky and uses her experience from working in many areas within nursing education to facilitate the most effective learning methods to students. She also helps new graduate students in the BSN Residency Program at UK Healthcare.
>University: University of Kentucky College of Nursing >More Details: Online Bio
Jacqueline Fawcett, Professor, Department of Nursing
University of Massachusetts Boston Professor Jacqueline Fawcett has spent the last 30 years working on a research project centered around the Roy Adaptation Model and has authored numerous conceptual models for nursing. Her impressive resume continues into renown for her meta-theoretical work as well.
>University: University of Massachusetts Boston >More Details: Online Bio
Anne Bruce, RN, PhD-Associate Professor
Anne Bruce is an Associate Professor of Nursing at the University of Victoria and is a PhD Coordinator as well. She has an impressive list of research she’s worked on and a great selection of publications.
>University: University of Victoria >More Details: Online Bio
Debra Sheets- Associate Professor
Working as an Associate Professor at the University of Victoria, Dr. Debra Sheets has over 20 years of clinical nursing experience and chairs the School of Nursing’s Undergraduate Committee. She’s worked as a research affiliate on the Centre on Aging at the University of Victoria and also on the Education Committee and helped conduct review panel work for federal agencies in America.
>University: University of Victoria >More Details: Online Bio
Ruth F. Craven, EdD, RN, FAAN -Professor Emerita
Ruth F. Craven looks in depth behavioral nursing, previously having worked in aging research and gerontological nursing, as well as nursing education. At the University of Washington, she also works with students on caring for the elderly and in-home care methods.
>University: University of Washington -Seattle >More Details: Online Bio
Barbara J. Bowers, Associate Dean for Research and Charlotte Jane and Ralph A. Rodefer Chair.
Barbara J. Bowers works largely with elderly individuals in residential and community settings to see how private and public policies can influence how seniors are cared for. In her time at the University of Wisconsin-Madison, she’s written an impressive array of publications, while also being awarded in 2002 and 2005 for her work in long term care and for the elderly.
>University: University of Wisconsin >More Details: Online Bio
Patricia Flatley Brennan, Lillian S. Moehlman-Bascom Professor of Nursing and Industrial Engineering. PhD
Patricia Flatley Brennan focuses on a very unique aspect of nursing research, specifically looking at how technology can influence self-care methods and reduce diagnosis time. Her research allows students to create integrative computer-based solutions for improving consumer health.
>University: University of Wisconsin >More Details: Online Bio
In April, we commemorate National Minority Health Month, a time to raise awareness about health disparities that persist among racial and ethnic minorities. This year’s theme - “Prevention is Power: Taking Action for Health Equity” - embodies the ambitious goal put forward by the U.S. Department of Health and Human Services (HHS) to achieve “a nation free of disparities in health and health care.”
Despite some recent progress in addressing health disparities, great challenges remain. Minorities are far more likely than non-Hispanic whites to suffer from chronic conditions, many of which are preventable. This is a particularly troubling statistic, because chronic diseases account for seven of the ten leading causes of death in our nation.
For example, African Americans, American Indians and Alaska Natives are twice as likely to be diagnosed with diabetes and Native Hawaiians and Pacific Islanders are more than three times as likely to receive the same diagnosis. And Latinos are twice as likely to die from liver cancer.
While these persistent disparities are deeply troubling, there are some hopeful trends. The gap in life expectancy between African Americans and non-Hispanic whites has been closing, and is now the smallest it’s been since these statistics have been tracked. Additionally, seasonal flu vaccination coverage has tripled for children over the past four years and has contributed to a reduction in vaccination disparities among minority children.
Thanks to the Affordable Care Act, health coverage is now more affordable and accessible for millions of Americans, including minority groups. For minority populations, the law addresses inequities in access to quality and affordable coverage. The impact of the Affordable Care Act on communities across our nation is transformative. Over seven million African Americans, nearly four million Asian Americans and Pacific Islanders, and over eight million Latinos with private insurance now have access to expanded preventive services with no cost sharing. This includes screening for colon cancer, Pap smears and mammograms for women, well-child visits, and flu shots for children and adults. Communities across the country are now stronger because the law invests in creating healthier communities, strong public health infrastructure, and preventing disease before it starts.
During Minority Health Month, we applaud the commitment of all of our federal, state, tribal, and local partners in our shared work to implement the HHS Action Plan to Reduce Racial and Ethnic Health Disparities and the National Stakeholder Strategy for Achieving Health Equity. To learn more about National Minority Health Month and what HHS is doing to achieve health equity, please visit www.minorityhealth.hhs.gov
The United States is rich with diversity, which is reflected in the observances celebrated by its various cultures and populations. Knowledge of the following diversity holidays and celebrations can enhance your workplace diversity and inclusion efforts. (Please note: All dates are for 2014.)
January
January 6 is Epiphany, a holiday recognizing the visit of the three wise men to the baby Jesus 12 days after his birth. The holiday is observed by both Eastern and Western churches.
January 14 is Makar Sankranti, a major harvest festival celebrated in various parts of India.
January 14 is also Eid Milad Un Nabi, an Islamic holiday commerating the birthday of the prophet Muhammad. During this celebration, homes and mosques are decorated, large parades take place, and those observing the holiday participate in charity events.
January 15 (sunset) – January 16 (sunset) is Tu B'shvat, a Jewish holiday recognizing "The New Year of the Trees." It is celebrated on the fifteenth day of the Hebrew month of Shevat. In Israel, the flowering of the almond tree usually coincides with this holiday, which is observed by planting trees and eating dried fruits and nuts.
January 16 is Mahayana New Year celebrated on the first full-moon day in January by members of the Mahayana Buddhist branch.
January 19 is World Religion Day. This day is observed by those of the Baha’i faith to promote interfaith harmony and understanding.
Third Monday in January (January 20) is Martin Luther King Day, commemorating the birth of Martin Luther King, Jr., the recipient of the 1964 Nobel Peace Prize and an activist for non-violent social change until his assassination in 1968.
January 18-25 is the Week of Prayer for Christian Unity. During the week, Christians pray for unity between all churches of the Christian faith.
January 26 is Republic Day of India. This day recognizes the date the Constitution of India came into law in 1950, replacing the Government of India Act of 1935. This day also coincides with India's 1930 declaration of independence.
January 31 is the birthday of Guru Har Rai, the seventh Sikh guru.
January 31 also marks the start of the Asian Lunar New Year, celebrated by many Asian groups including Chinese, Vietnamese, and Koreans. This year is the Year of the Wooden Horse.
January 31-February 14 marks the Chinese New Year. This year is the Year of the Wooden Horse. Chinese New Year is the most important holiday in the Chinese lunisolar calendar and is recognized by gift giving, parades, decorations, and feasting. The celebration culminates with the Lantern Festival on February 14.
February
February is Black History Month in the United States and Canada. Since 1976, the month has been designated to remember the contributions of people of the African Diaspora.
February 8 is Nirvana Day, the commemoration of Buddha’s death at the age of 80, when he reached the zenith of Nirvana. February 15 is an alternative date of observance.
February 17 is President’s Day, originally established to honor Presidents Washington and Lincoln, it now serves as a reminder of the contributions of all U.S. presidents.
February 26 – March 1 are Intercalary Days for people of the Baha’i faith. At this time, days are added to the Baha’i calendar to maintain their solar calendar. Intercalary days are observed with gift giving, special acts of charity, and preparation for the fasting that precedes the new year.
February 27 is Mahashivratri, a Hindu holiday that honors Shiva, one of the Hindu deities.
March
March is Women’s History Month. Started in 1987, Women’s History Month recognizes all women for their valuable contributions to history and society.
March is also National Mental Retardation Awareness Month, which was established to increase awareness and understanding of issues affecting people with mental retardation and other developmental disabilities.
March is National Multiple Sclerosis Education and Awareness Month. It was established to raise public awareness of the autoimmune disease that affects the brain and spinal cord and assist those with multiple sclerosis in making informed decisions about their health care.
March 2 is Losar, the Tibetan Buddhist New Year. Losar, which means new year in Tibetan, is considered the most important holiday in Tibet.
March 5 is Ash Wednesday, the beginning of Lent in the Christian faith. As a display of atonement, ashes are marked on worshippers. Lent, which is observed during the seven weeks prior to Easter, is a time of reflection and preparation for the Holy Week and is observed by fasting, charitable giving, and worshipping.
March 8 is International Women’s Day. First observed in 1911 in Germany, it has now become a major global celebration honoring women’s economic, political, and social achievements.
March 13 – April 15 is Deaf History Month. This observance celebrates key events in deaf history, including the founding of Gallaudet University and the American School for the Deaf.
March 15 (sunset)- March 16 (sunset) is Purim, a Jewish celebration that marks the time when the Jewish community living in Persia was saved from genocide. According to the Book of Esther, King Ahasuerus’s political advisor planned to have all the Jews killed; however, his plot was foiled when Esther, one of the king’s wives, revealed her Jewish identity. On Purim, Jewish people offer charity and share food with friends.
March 16 is Magha Puja Day, a Buddhist holiday that marks an event early in the Buddha’s teaching life when a group of 1,250 enlightened saints, ordained by the Buddha, gathered to pay their respect to him.
March 17 is St. Patrick’s Day, a holiday started in Ireland to recognize St. Patrick, the patron saint of Ireland, who brought Christianity to the country in the early days of the faith.
March 17 is also Holi, a Hindu and Sikh spring religious festival observed in India, Nepal, and Sri Lanka, along with other countries that have large Hindu and Sikh populations. People celebrate Holi by throwing colored powder and water at each other. Bonfires are lit the day before in the memory of the miraculous escape that young Prahlad accomplished when Demoness Holika carried him into the fire.
April
April is Celebrate Diversity Month, started in 2004 to recognize and honor the diversity surrounding us all. By celebrating differences and similarities during this month, organizers hope that people will get a deeper understanding of each other.
April is Autism Awareness Month, established to raise awareness about the developmental disorder that affects children's normal development of social and communication skills.
April 2 is World Autism Awareness Day, created to raise awareness of the developmental disorder around the globe.
April 8 is Ram Navami, a Hindu festival commemorating the birth of Lord Rama, a popular deity in Hinduism. People celebrate the holiday by sharing stories and visiting temples.
April 13 is Palm Sunday, a holiday recognized by Christians to commemorate the entry of Jesus in Jerusalem. It is the last Sunday of Lent and the beginning of the Holy Week.
April 14 (sunset)- April 22 (sunset)is Passover, a Jewish holiday celebrated each spring in remembrance of the Jews’ deliverance out of slavery in Egypt in 1300 B.C. On the first two days of Passover, a traditional Seder is eaten and the story of deliverance is shared.
April 18 is Good Friday, celebrated by Christians to commemorate the execution of Jesus by crucifixion and is recognized on the Friday before Easter.
April 20 is Easter, a holiday celebrated by Christians to recognize Jesus’ return from death after the crucifixion. It is considered to be the most important Christian holiday.
May
May is Asian-American and Pacific Islander Heritage Month in the United States. The month of May was chosen to commemorate the immigration of the first Japanese to the United States on May 7, 1843, and to mark the anniversary of the completion of the transcontinental railroad on May 10, 1869. The majority of the workers who laid the tracks on the project were Chinese immigrants.
May is also Older Americans Month, established in 1963 to honor the legacies and contributions of older Americans and to support them as they enter their next stage of life.
May 21 is World Day for Cultural Diversity for Dialogue and Development, a day set aside by the United Nations as an opportunity to deepen our understanding of the values of cultural diversity and to learn to live together better.
May 25 is Lailat al Mairaj. On this day, Muslims celebrate Prophet Muhammad’s night journey from Makkah to Jerusalem and his ascension to heaven.
June
June is Lesbian, Gay, Bisexual, and Transgender Pride Month, established to recognize the impact that gay, lesbian, bisexual, and transgender individuals have had on the world. Gay, lesbian, and bisexual groups celebrate this special time with pride parades, picnics, parties, memorials for those lost to hate crimes and HIV/AIDS, and other group gatherings. The last Sunday in June is Gay Pride Day.
June 12is Lailat al Bara’a, celebrated as the night of forgiveness by Muslims.
June 14 is Flag Day in the United States. This day is observed to celebrate the history and symbolism of the American flag.
June 15 is Native American Citizenship Day. This observance commemorates the day in 1924 when the United States Congress passed legislation recognizing the citizenship of Native Americans.
On June 16, Sikhs observe the Martyrdom of Guru Arjan Dev. Guru Arjan Dev was the fifth Sikh guru and the first Sikh martyr.
June 19 is Juneteenth, also known as Freedom Day or Emancipation Day. It is observed as a public holiday in 14 U.S. states. This celebration honors the day in 1865 when slaves in Texas and Louisiana finally heard they were free, two months after the end of the Civil War. June 19, therefore, became the day of emancipation for thousands of Blacks.
June 19 is also Corpus Christi, a Catholic celebration in honor of the Eucharist.
The last Sunday in June (June 29) is Lesbian, Gay, Bisexual, Transgender (LGBT) Pride Day in the United States.
June 29 marks the beginning of Ramadan, the Islamic month of fasting. Muslims abstain from eating, drinking, and sexual activity from dawn until sunset, in efforts to teach patience, modesty, and spirituality. This year, the observance lasts until July 29.
July
On July 9, the Martyrdom of the Bab, Baha'is observe the anniversary of the Bab's execution in Tabriz, Iran, in 1850.
July 11 is World Population Day, an observance established in 1989 by the Governing Council of the United Nations Development Programme. The annual event is designed to raise awareness of global population issues.
July 13 is Asala–Dharma Day, which celebrates the anniversary of the start of the Buddha’s teaching.
July 23 is the birthday of Haile Selassie I, the Emperor of Ethiopia, who the Rastafarians consider to be God and their Savior.
July 26 is Disability Independence Day, which marks the anniversary of the 1990 signing of the Americans with Disabilities Act.
July 29 is Eid al Fitr, the Muslim celebration commemorating the ending of Ramadan. It is a festival of thanksgiving to Allah for enjoying the month of Ramadan. It involves wearing one's finest clothing, saying prayers, and nurturing understanding of other religions.
August
August 4 (sunset) - August 5 (sunset) Tisha B’ Av, an annual fasting day, is observed to commemorate the tragedies that have befallen the Jewish people.
August 6 is Transfiguration, a holiday recognized by Orthodox Christians to celebrate when Jesus became radiant, and communed with Moses and Elijah on Mount Tabor. To celebrate, adherents have a feast.
August 9 is International Day of the World's Indigenous Peoples. The focus this year is "Indigenous peoples building alliances: Honouring treaties, agreements and other constructive arrangements."
August 10 is Raksha Bandhan, a Hindu holiday commemorating the loving kinship between a brother and a sister. Raksha means protection in Hindi, and symbolizes the longing a sister has to be protected by her brother. During the celebration, a sister ties a string around her brother's (or brother-figure’s) wrist, and asks him to protect her. The brother usually gives the sister a gift and agrees to protect her for life.
August 12 is Pioneer Day, observed by the Mormons to commemorate the arrival in 1847 of the first Latter Day Saints pioneer in Salt Lake Valley.
August 17 is Marcus Garvey Day, which celebrates the birthday of the Jamaican politician and activist who is revered by Rastafarians. Garvey is credited with starting the Back to Africa movement, which encouraged those of African descent to return to the land of their ancestors during and after slavery in North America.
August 26 is Women’s Equality Day, which commemorates the August 26, 1920 certification of the 19th Amendment to the United States Constitution, which gave women the right to vote. Congresswoman Bella Abzug first introduced a proclamation for Women’s Equality Day in 1971. Since that time, every president has published a proclamation recognizing August 26 as Women’s Equality Day.
August 28 is Janmashtami, a Hindu holiday recognizing Krishna’s birthday. Krishna is the highest god in the Hindu faith.
September
September 10 is Paryushana, the most revered Jain festival comprising eight or ten days of fasting and repentance.
September 11 is the Ethiopian New Year. Rastafarians celebrate the New Year on this date and believe that Ethiopia is their spiritual home, a place they desire to return to.
September 15 – October 15 is Hispanic Heritage Month. This month corresponds with Mexican Independence Day, which is celebrated on September 16, and recognizes the revolution in 1810 that ended Spanish dictatorship.
September 24 (sunset) – September 26 (nightfall) is Rosh Hashanah, a holiday recognizing the Jewish New Year. It is the first of the Jewish High Holy Days, and is marked by abstinence, prayer, repentance, and rest.
October
October is National Disability Employment Awareness Month. This observance was launched in 1945 when Congress declared the first week in October as "National Employ the Physically Handicapped Week." In 1998, the week was extended to a month and renamed. The annual event draws attention to employment barriers that still need to be addressed.
October is also LGBT History Month, a U.S. observance started in 1994 to recognize lesbian, gay, bisexual, and transgender history and the history of the gay rights movement.
October 3 (sunset)- October 4 (sunset) is Yom Kippur. This holiday is the holiest day on the Jewish calendar and is a day of atonement marked by fasting and ceremonial repentance.
October 4 marks the beginning of Dussehra (Dasera), a ten day festival celebrated by Hinus to recognize Rama's victory over evil.
October 8 (sunset)- October 15 (sunset) is the Jewish holiday of Sukkot. It is a time of rememberance of the fragile tabernacles that Israelites lived in as they wandered the wilderness for 40 years. The first day of the holiday is celebrated with prayers and special meals.
October 11 is National Coming Out Day. For those who identify as lesbian, gay, bisexual, or transgender, this day celebrates coming out and the recognition of the 1987 march on Washington for gay and lesbian equality.
Second Monday in October is National Indigenous People’s Day, which recognizes 500 years of resistance and the continued existence of North American Indigenous people. This is celebrated in lieu of Columbus Day.
October 20 is Birth of the Bab, a holiday celebrated by the Baha'i recognizing the birth of the founder of the Baha'i faith.
October 23 marks the beginning of Diwali (the festival of lights), celebrated by Sikhs, Hindus, and Jains. The holiday is observed with decorating homes with lights and candles, setting off fireworks, and distributing sweets and gifts.
November
November is National Native American Heritage Month, which celebrates the history and contributions of Native Americans.
November 3 is Ashura, a holiday recognized by Muslims to mark the martyrdom of Hussain. It also commemorates that day Noah left the ark and Moses was saved from the Egyptians by God.
November 11 is Veterans Day, an annual U.S. federal holiday honoring military veterans. The date is also celebrated as Armistice Day or Remembrance Day in other parts of the world and commemorates the ending of the first World War in 1918.
November 12 is the Birth of Baha’u’llah, a day on which members of the Baha’i faith celebrate the birthday of the founder of the Baha’i religion.
November 20 is Transgender Day of Remembrance, established in 1998 to memorialize those who have been killed as a result of transphobia and raise awareness of the continued violence endured by the transgender community.
November 23 is Feast of Christ the King, the last holy Sunday in the western liturgical calendar. This day is observed by the Roman Catholic Church, as well as many Anglicans, Lutherans, and other mainline Protestants.
December
December 1 is World AIDS Day, which was created to commemorate those who have died of AIDS, and to acknowledge the need for a continued commitment to all those affected by the HIV/AIDS epidemic.
December 8 is Bodhi Day, a holiday observed by Buddhists to commemorate Gautama’s enlightenment under the Bodhi tree at Bodhgaya, India.
December 10 is International Human Rights Day, established by the United Nations in 1948 to commemorate the anniversary of the Universal Declaration of Human Rights.
December 12 is Feast Day at Our Lady of Guadalupe. This day commemorates the appearance of the Virgin Mary near Mexico City in 1531.
December 16-24 is Las Posadas, a nine-day celebration in Mexico commemorating the trials Mary and Joseph endured during their journey to Bethlehem.
December 16 (sunset) - December 24 (sunset) is Hanukkah (Chanukah). Also known as the Festival of Lights, it is an eight-day Jewish holiday recognizing the rededication of the Holy Temple in Jerusalem. It is observed by lighting candles on a Menorah—one for each day of the festival.
December 25 is Christmas, the day that Christians associate with Jesus’ birth.
December 26 – January 1 is Kwanzaa, an African-American holiday started by Maulana Karenga in 1966 to celebrate universal African-American heritage. It is observed by lighting candles to represent each of the holiday’s seven principles, libations, feasting, and gift giving.
A professional practice environment that is supportive of nursing helps explain why Magnet hospitals have better nurse-reported quality of care than non-Magnet hospitals, according to a study.
As published earlier this year in the Journal of Nursing Administration, researchers with the New York University College of Nursing and University of Pennsylvania School of Nursing explored links between recognized nursing excellence and quality patient outcomes.
Only 9% of American hospitals have Magnet recognition, according to an NYU news release, and Magnet hospitals have higher job satisfaction and lower odds of patient mortality than non-Magnet hospitals. Research into the causes of the differences could create an infrastructure for positive change in nurse and patient outcomes.
“Many of the recent efforts to improve quality and enhance transparency in healthcare have been dominated by physician services and medical outcomes,” Amy Witkoski Stimpfel, RN, PhD, assistant professor at NYUCN, said in the news release. “Our study shows that the overall quality of patient care can be optimized when nurses work in a positive environment, with adequate resources and support at the organizational level.”
The study, “Understanding the Role of the Professional Practice Environment on Quality of Care in Magnet and Non-Magnet Hospitals,” focused on cross-sectional data, including the American Hospital Association’s annual survey, and an analysis of 56 Magnet and 495 non-Magnet hospitals.
Witkoski Stimpfel’s team found a clear correlation between positive work environments for nurses and nurse-reported quality of care. Even after taking into consideration hospital characteristic differences between Magnet and non-Magnet hospitals, Magnet hospitals still were positively correlated with higher reports of excellent quality of care.
“Having visible and accessible chief nurses, encouraging and including nurses in decision-making in their unit and throughout the organization, supporting nursing practice and engaging in interdisciplinary patient care are but a few examples of readily modifiable features of a hospital,” Witkoski Stimpfel said.
“Because all organizations, Magnet and otherwise, have the potential to enrich their practice environment, every organization stands to benefit from improving the organization of nursing care.
“Our findings suggest that Magnet hospitals produce better quality of care through their superior practice environments. Hospitals that invest in improving the nursing work environment have the potential to benefit from increased quality of care for their patients and families.”
Witkoski Stimpfel is continuing to research the outcomes associated with Magnet hospitals. Her current project is an assessment of the relationship between Magnet recognition and patient satisfaction in a national sample of hospitals.
As a registered nurse in the cardiac surgery ICU at Beth Israel Medical Center, Valley Fox, RN, BSN, MA, AP, CCRN, witnesses the spectrum of life and death.
Her days are full of pharmaceuticals, imaging studies and other visual elements, which she reinterprets into an artistic language that explores the relationship between body and spirit.
“I take inspiration from the hospital because that’s where I spend my time,” Fox said. “Being in the presence of those images and bodies, it comes through instinctively.”
In one piece of artwork Fox donated to the American Heart Association and the cardiac surgery unit, she subtly embedded a heart in the middle of a flower. Many people did not notice, but her colleagues on the unit spotted it immediately.
“The heart is the center of everybody,” said Cathy Sullivan, RN, BS, MSN, FNP, CCRN, director of patient care services, Beth Israel Medical Center — Petrie Division. “Without your heart, you wouldn’t have a body or soul.”
Beth Israel Medical Center nurse Valley Fox, RN, recently completed a month-long art exhibit at New York University’s medical sciences building called “Origins of Medicine.”
Mary Anne Gallagher, RN, MA, BC, director of quality, standards and practice at Beth Israel, envisioned a fetus and baby in one of Fox’s paintings, which the artist had not intentionally set out to create. “When you are in her presence, there’s a feeling of peace and comfort,” Gallagher said.
Art came first for Fox, who was born with severe myopia. Her inability to see clearly beyond 10 inches went unrecognized until she was in kindergarten, when she received glasses. “As a child, I was always drawing because that’s how I processed reality,” Fox said. “I would play with Play-Doh. I was constantly doing artwork as a child.”
The school allowed Fox, a gifted student, to paint twice a week in her elementary school years, where she developed her skills and creativity. “Everyone has creative capacities,” Fox said.
Her parents encouraged Fox to pursue “a practical degree” rather than art. After completing her nursing school prerequisites and waiting to be admitted to a nursing program, she turned to Chinese medicine. She completed a master of oriental medicine at the Atlantic Institute of Oriental Medicine in Fort Lauderdale, Fla., but the timing was not ideal to set up her own practice as an acupuncture physician.
Still, healthcare intrigued her, and the opportunity to travel, move around and practice in different places cinched her decision to become an RN. She worked in Florida, Illinois and upstate New York before settling in New York City. Nursing is a career path she has not regretted.
“Being a nurse is incredibly rewarding, to help patients when they are in tremendous need and offer support and listen,” Fox said. “I get to share intimate moments with total strangers, and then there are critical moments where we work together as a team and save someone’s life. It’s an incredible opportunity.”
Fox credits her artistic background with the intuitive skills she draws from as a critical care nurse. She considers the interconnectivity of the mind and body and draws from her experience in medicine to pick up subtle clues.
“Sometimes, that right brain element comes through, and we can sense a patient may code and prevent an emergency,” Fox said.
Fox professionally displays and sells her paintings and recently completed a monthlong exhibit at New York University’s medical science building called “Origins of Medicine,” in which she explored the relationship between the mind and body in medicine.
“Valley looks at the patient as a whole and anticipates,” Sullivan said. “That’s the type of nurse you need, one who pays attention to detail. And artists pay attention to details.”
I have been an RN for two years, but have worked for only a couple of months because I got sick. No one wants to hire me without experience. My credentials are perfect. I reside in Florida and cannot relocate because I am a mother of small children. Can you offer some advice?
Wants to Work
Dear Donna replies:
Dear Wants to Work,
Don't be discouraged. The job market is shifting and changing. Even though you are not a new nurse, read “New nurse, new job strategies” to see what's happening and learn creative ways to market yourself (www.Nurse.com/Cardillo/Strategies).
You should start volunteering as a nurse while you continue to look for paid employment. Volunteering is a great way to gain recent relevant experience, to hone old skills and learn new ones, build confidence and expand your professional network. Plus, volunteering often leads to paid employment as it is a way to get your foot in the door somewhere. Look for opportunities at your local public health department, a free clinic, the American Red Cross, a cancer care center or a blood bank.
You also should attend local chapter meetings of the Florida Nurses Association (www.floridanurses.org). You do not have to be a member of ANA/FNA to attend meetings as a guest. This is a great way to reconnect to your profession, get up to date on issues and trends and further expand your network. Networking is well known to be a great way to find and get a job.
When what you're doing isn't working, it's time to try a new approach. You will be able to find work. You'll just have to look in new directions for employment and use a new approach to find and get those jobs. Persistence and determination will always win out in the end.
Modern medicine has helped lead to a surge in average life expectancy, which was only about 36 in the late 1800s. With humans routinely living into their 100s, advances in medical science are to thank. Let’s take a journey through the history of medical advancements.
Cancer 400 BC: Hippocrates uses the term “karcinos” to describe tumors. “Karcinos” evolved into cancer. It’s not yet known what causes cancer, with theories including imbalanced “humors” in the body. Immunization and disease prevention 400 BC: Hippocrates describes mumps, diphtheria, epidemic jaundice and other conditions. Mental illness 400 BC: Mental disorders are understood as diseases rather than symptoms of demonic possession or signs of having displeased the gods.
2nd century AD
Cancer 2nd century AD: Galen describes surgical treatments for breast cancer, which include removing early-stage tumors. But the surgeries are brutal and often fatal. For centuries, these rudimentary surgeries are the only treatment for cancer.
1100s
Immunization and disease prevention 1100s: The variolation technique is developed, involving the inoculation of children and adults with dried scab material recovered from smallpox patients.
1400s
Mental illness 1407: The first European establishment specifically for people with mental illness is probably established in Valencia, Spain.
1500s
Surgery and medical technology 1540 AD: English barbers and surgeons perform tooth extractions and blood-letting.
1600s
Mental illness 1600s: Europeans increasingly begin to isolate mentally ill people, often housing them with handicapped people, vagrants and delinquents. Those considered insane are increasingly treated inhumanely, often chained to walls and kept in dungeons.
1700s
Immunization and disease prevention 1798: Edward Jenner publishes his work on the development of a vaccination that would protect against smallpox. He tests his theory by inoculating 8-year-old James Phipps with cowpox pustule liquid recovered from the hand of a milkmaid, Sarah Nelmes. Mental illness Late 1700s: After the French Revolution, French physician Phillippe Pinel takes over the Bicêtre insane asylum and forbids the use of chains and shackles. He removes patients from dungeons, provides them with sunny rooms and allows them to exercise on the grounds. Yet in other places, mistreatment persists.
1800s
Surgery and medical technology 1818: Human blood is transfused from one person to another for the first time. Mental illness 1840s: U.S. reformer Dorothea Dix observes mentally ill people in Massachusetts, seeing men and women of all ages incarcerated with criminals, left unclothed and in darkness and forced to go without heat or bathrooms. Cancer & surgery/medical technology 1846: Anesthesia becomes widely available, helping expand options for surgery. Among cancer patients, surgery to remove tumors takes off. Surgery and medical technology 1867: British surgeon Joseph Lister publishes Antiseptic Principle in the Practice of Surgery, extolling the virtues of cleanliness in surgery. The mortality rate for surgical patients immediately falls. Immunization and disease prevention 1881: Louis Pasteur and George Miller Sternberg almost simultaneously isolate and grow the pneumococcus organism. Mental illness 1883: Mental illness is studied more scientifically as German psychiatrist Emil Kraepelin distinguishes mental disorders. Though subsequent research will disprove some of his findings, his fundamental distinction between manic-depressive psychosis and schizophrenia holds to this day. Surgery and medical technology 1885: The first successful appendectomy is performed in Iowa. Mental illness Late 1800s: The expectation in the United States that hospitals for the mentally ill and humane treatment will cure the sick does not prove true. State mental hospitals become over-crowded, and custodial care supersedes humane treatment. New York World reporter Nellie Bly poses as a mentally ill person to become an inmate at an asylum. Her reports from inside result in more funding to improve conditions. Cancer 1889: William Halsted develops the radical mastectomy to treat breast cancer; the technique includes the surgical removal of the tumor, breast, overlying skin and muscle. Surgery and medical technology 1890s: Chemical agents are used to minimize germs. Carbolic acid is put on incisions to minimize germs and decrease infection rates. Cancer 1895: Wilhelm Conrad Roentgen invents X-rays. Radiation therapy follows. Surgery and medical technology 1895: The first X-ray is performed in Germany.
1900s
Mental illness Early 1900s: The primary treatments of neurotic mental disorders, and sometimes psychosis, are psychoanalytical therapies (“talking cures”) developed by Sigmund Freud and others, such as Carl Jung. Immunization and disease prevention 1914: Typhoid and rabies vaccine are first licensed in the U.S.; tetanus toxoid is introduced. Immunization and disease prevention 1915: Pertussis vaccine is licensed. Immunization and disease prevention 1918: The Spanish influenza pandemic is responsible for 25 million to 50 million deaths worldwide, including more than 500,000 in the U.S. Cancer 1919: A chemical in the mustard gas used during World War I is found to reduce white blood cells. Chemotherapy is born. Surgery and medical technology 1922: Insulin is first used for treatment of diabetes, allowing diabetics to survive after diagnosis. Surgery and medical technology 1928: Antibiotics dramatically decrease post-surgical infections. Mental illness 1930s: Drugs, electro-convulsive therapy, and surgery are used to treat people with schizophrenia and others with persistent mental illnesses. Some are infected with malaria; others are treated with repeated insulin-induced comas. Others have parts of their brain removed through lobotomies. Surgery and medical technology 1937: The first blood bank opens, helping make more surgery possible by treating bleeding during the procedure. Immunization and disease prevention 1943: Penicillin becomes mass-produced. Mental illness 1946: President Harry Truman signs the National Mental Health Act, calling for the National Institute of Mental Health to conduct research into the brain and behavior and reduce mental illness. Cancer 1947: Chemotherapy records its first, though temporary, success with the remission of a pediatric leukemia patient. Mental illness 1949: Australian psychiatrist J. F. J. Cade introduces the use of lithium to treat psychosis. Lithium gains wide usage in the mid-1960s to treat those with manic depression, now known as bipolar disorder. Surgery and medical technology 1950: John Hopps invents the cardiac pacemaker. Cancer 1950s: Findings related to DNA give rise to molecular biology. Mental illness 1950s: A series of successful anti-psychotic drugs are introduced that do not cure psychosis but control its symptoms. The first of the anti-psychotics, the major class of drug used to treat psychosis, is discovered in France in 1952 and is named chlorpromazine (Thorazine). Studies show that 70 percent of patients with schizophrenia clearly improve on anti-psychotic drugs. Mental illness 1950s: A new type of therapy, behavior therapy, suggests that people with phobias can be trained to overcome them. Surgery and medical technology 1953: A heart-lung bypass machine is used successfully for the first time. Immunization and disease prevention 1955: The first polio vaccine is licensed, pioneered by Dr. Jonas Salk. The Polio Vaccination Assistance Act is enacted by Congress, the first federal involvement in immunization activities. Surgery and medical technology 1957: William Grey Walter invents the brain EEG topography (toposcope). Cancer 1964: A U.S. surgeon general’s report establishes an undeniable link between smoking and cancer. Mental illness Mid-1960s: Many seriously mentally ill people are removed from institutions. In the United States they are directed toward local mental health homes and facilities. The number of institutionalized mentally ill people in the United States will drop from a peak of 560,000 to just over 130,000 in 1980. Many people suffering from mental illness become homeless because of inadequate housing and follow-up care. Immunization and disease prevention 1966: The Centers for Disease Control and Prevention announces the first national measles eradication campaign. Within 2 years, measles incidence decrease by more than 90% compared with prevaccine-era levels. Surgery and medical technology 1967: A heart transplant is performed by South African physician Christian Barnard. The heart recipient survived 18 days until succumbing to pneumonia. Cancer 1971: President Richard M. Nixon signs the National Cancer Act. Cancer 1972: The development of computed tomography (CT) revolutionizes radiology. Cancer 1973: Dr. Janet Rowley shows chromosome abnormalities in those with cancer. Surgery and medical technology 1978: A baby conceived via in-vitro fertilization is born. Mental illness 1980s: An estimated one-third of all homeless people are considered seriously mentally ill, the vast majority of them suffering from schizophrenia. Cancer 1981: FDA approves the first vaccine against hepatitis B, one of the primary causes of liver cancer. Surgery and medical technology 1982: The Jarvik-7 artificial heart is used. Surgery and medical technology 1985: The first documented robotic surgery is performed. Mental illness 1986: Prozac is developed to treat various mental illnesses. Cancer Early 1990s: For the first time, overall cancer death rates begin to fall. Mental illness 1990s: A new generation of anti-psychotic drugs is introduced. These drugs prove to be more effective in treating schizophrenia and have fewer side effects. Immunization and disease prevention 1994: The entire Western Hemisphere is certified as “polio-free” by the World Health Organization.
2000s
Surgery and medical technology 2000: Robotic surgical systems win U.S. Food and Drug Administration approval. Cancer 2001: The FDA approves Gleevec, the first drug to target a specific gene mutation. Surgery and medical technology 2003: The sequence of a complete human genome is published. Immunization and disease prevention 2006: A vaccine is developed to prevent cervical cancer due to human papillomavirus. Immunization and disease prevention 2009: The vaccine court rules that the mumps/measles/rubella vaccine, when administered with thimerosal-containing vaccines, does not cause autism.
We all have moments in which the stress of our jobs threatens to make our heads spin around 360 degrees. Moments like that are fine, but if there’s a trend toward constant head-spinning, then you, my friend, need an intervention.
Tip One: Make sure your personal space is as stress-free as possible. When you come home at night or in the morning, are you faced with stacks of dishes in the sink and cat hair everywhere? You need to start taking care of that stuff on your days off. Your home is a haven. Even with roommates or kids, you can have one space that’s inviolable and neat and clean. That one thing will make such a difference in your mental health, it’s amazing.
Tip Two: Treat your body well. Fast food is good once in a while, but for tip-top functioning, you really need to pay attention to how you feed your body. Good, clean food will help your body and brain work well and will lessen your stress levels immensely. Batch-cooking things you can stand to eat during and after your shifts will make you so much happier than a burger from Big Bob’s Burger Barn.
Tip Three: Simplify. I have six of the exact same uniform, four bras that I know fit perfectly and eight pairs of socks that are identical. I have a zippered makeup bag that I got for a buck at Target that holds all my work stuff, from pens to stethoscope to ID. I have set jewelry to wear to work, and a set time in the morning by which certain things have to be accomplished. This makes my life so much easier, I can’t even tell you.
Integral to this plan is a coffeemaker with a timer. If you don’t own one, go get one.
Tip Four: Know which stress relievers are good in the long run. I’m a big fan of carefully applied general anesthetic in the form of ETOH (as my mother says), but not after every shift. A glass of wine or other Adult Beverage of your choice can be helpful when you’re too wound up to sleep or if your brain simply won’t shut up…but don’t make a habit of it. Exercise is better (and I’ve never found that getting good and sweaty an hour before bed will make me insomniac), venting to a friend is good (especially if she’s not also a nurse), playing catch with your pup or the neighbor’s kids can work. Know what’s healthy (movement, talk, art, music) and what’s not (alcohol, too much food, drugs), and plan accordingly.
Tip Five: Get a massage. Seriously. Touch is amazing for making you feel better. Find yourself a good massage therapist and get the two-hour rubdown. Don’t plan anything at all for the rest of the day. You’d be amazed at how small niggling problems and constant stressors seem when you can barely walk to the car. If you can afford it, do it once or twice a month: It’ll give you something to look forward to, and you’ll feel amazing for at least a day or so.
For nearly a year, the Boston Marathon bombings and their aftermath have haunted Chelsey McGinn, RN, of the Blake 12 Intensive Care Unit (ICU). In December the MGH gave McGinn an opportunity to honor the victims – and begin her own healing process – by running this year’s marathon as part of its Emergency Response Fund team.
“I feel like it’s been almost a year now, and I haven’t really done anything therapeutic since it happened,” McGinn says. “I felt like other people who I worked with found ways to kind of cope with it, but I hadn’t really found that. When this came up, I thought this was a perfect way to celebrate how far the victims have come and recognize my co-workers.”
McGinn is one of six nurses on her unit who are planning to run the 2014 Boston Marathon – five for charity teams and one as a qualified runner. Most are first-time runners, and all say they are running in honor of the three bombing victims who were treated on the unit.
“I had a really hard time afterward, and it lasted longer than I expected,” says Laura Lux, RN, who is running for the American Red Cross. “I’m running because I don’t want to be defeated. I know if he could, my patient would be running just to prove a point. Because he can’t, I feel like I need to do this for him. After watching what he and his family went through, I feel like it’s the least I could do for them.”
Lux says she felt an immediate connection with her patient and his family. “Despite everything they were just so determined and so strong,” she says. “Everyone was angry, but there was good coming from it too. We got to know each other because of it. I felt like he was a family member. It’s the most personal experience of my career.”
Lux’s experience is similar to that of the other nurses who are running, including Emily Erhardt, RN, a trauma ICU nurse and member of the MGH Emergency Response Fund Team, who has stayed in touch with her patient and his family since they left the hospital. “This event affected everyone, so it was one of the few times in my career that I felt like all I could do with the family was cry with them. It’s such a terrible thing that happened that there aren’t words to comfort them. You just have to be there for them,” she says. “A year ago they were strangers to me, but now they’re the most inspiring people in my life. I’m not much of an athlete, but I was really affected by the whole thing, and I wanted to do something more.”
Blake 12 runners receive a boost of support from the Harvard University Employees Credit Union. Included in the photo with members of the ICU are Paul Conners, MGH branch manager; Eugene Foley, president and CEO; and Guillermo Banchiere, MGH director of Environmental Services, who serves as a member of the credit union's board of directors.
Allyson Mendonza, RN, who is running for the Mass General Marathon Team “Fighting Kids Cancer … One Step At a Time,” recalls the moment she knew she too wanted to do something more. Mendonza says her patient had just returned from surgery when she was told President Barack Obama was coming to visit. The woman was excited but was distraught about her appearance, so Mendonza and her colleague soaked her nails and helped shampoo and condition her hair to wash out the cement and clumps of dried blood.
“We just tried our best to make her feel better about herself and feel good for the day ahead. She actually fell asleep. When she awoke, she said, ‘This is the most relaxed I have felt in days.’ It was just so emotional for us and for her,” Mendonza says.
Caring for the marathon victims brought the unit closer together, and staff once again have come together to support and encourage their fellow colleagues.
“The teamwork and the camaraderie were amazing,” saysKatherine Pyrek, RN, who was the charge nurse during the week of the bombing. “Every one of the nurses was affected by what was going on, but they stayed strong and carried on. The bonds the nurses made with the patients and their families were incredible and really went above and beyond.”
Pyrek, who is running for the Mass General Marathon Team, says the Blake 12 runners offer each other advice and encouragement to help in the training process. “We remind why we’re doing this – for our patients and their families,” she says. “I think about the patients when they were in pain and how scared they were. I think that if they get through it then I can get through however many miles I need to run.”
The runners all say they look to Meredith Salony, RN, a veteran marathoner who qualified for the marathon, for guidance. “I’m so proud to be in this unit where there’s so much enthusiasm. Even the people who aren’t running are trying to help out and organize events and find ways for people to contribute,” Salony says.
Each of the nurses says they are overwhelmed when they imagine how they will feel on Marathon Monday.
“I think it’ll be really therapeutic and empowering,” McGinn says. “I’m honored to be a part of it. If I’m ever going to run a marathon, this is the one I want to run. I’ll always remember the way I felt at work that night, and it’s going to be a really nice thing to be able to remember this feeling for the rest of my life too.”
For more information or to support the teams visit www.runformgh.org.
This is the first in a series of articles that MGH Hotline will publish about staff running in this year’s Boston Marathon.
Let’s say you’re a nurse at a local hospital. For the past several weeks, you’ve been for a young boy who needs a heart transplant.
One day, you learn that a donor organ has become available. You are elated – and you decide to share the news on your Facebook page.
“Great news! A new heart has been found for my five-year-old patient at Children’s. Be brave, Aiden – we’re all rooting for you!”
Good idea? Not really.
That’s because a post like this – while well intentioned – is a breach of confidentiality. There’s enough information here to identify the patient, his condition and the hospital where he is receiving treatment. Put it all together, and you’ve got yourself a HIPAA violation.
The truth is, there can be real consequences to nurses’ irresponsible use of social media. State boards of nursing may investigate reports of inappropriate disclosures on Facebook and other social media sites. If the allegations are found to be true, nurses can face reprimands, sanctions, fines, or temporary or permanent loss of their nursing license.
Many organizations have social media policies that govern employees’ use of social media, even if it’s for personal purposes. If yours is one of them, be sure to read and understand the guidelines.
Even if your employer does not have a specific policy, the main rule of thumb should be familiar to you: as a nurse, you have the legal and ethical obligation to maintain patient privacy and confidentiality.
The Health Insurance Portability and Accountability Act (HIPAA) specifically defines “identifiable information” and when and how it can be used. Such identifiable information could cover the past, present or future health of a patient, or it could be something that would lead someone to believe that it could be used to identify a patient. Brush up on your understanding of HIPAA.
How do you avoid problems? Do you need to stop using Facebook altogether if you’re a nurse? No, but you do need to be careful. Here are a few general guidelines:
-Simply put: Don’t reveal any personal health information about your patients in your posts. (And don’t think that it’s OK if you reveal their details but give them a fake name.)
-Don’t post any photos of your patients, even if they are cute kids. Photos are specifically called out in HIPAA as identifiable information.
-Maintain professional boundaries, even online. Friending your patients or patients’ families is, in most cases, a no-no. The Mayo Clinic’s guidelines for employees say, “Staff in patient care roles generally should not initiate or accept friend requests except in unusual circumstances such as the situation where an in-person friendship pre-dates the treatment relationship.”
-Don’t rely on privacy settings. No matter how meticulous you are about privacy settings, there’s no guarantee that a friend won’t like your post so much that she takes a screenshot and posts your “private” message elsewhere.
-Remember that anything online will be there forever, even if you delete it. Someone may have taken a screenshot before you took your post down. If you are under investigation, your posts can be still found on servers.
Pagana, K. (2014, January 21). Facebook: Know the Policy Before Posting [Webinar]. In Nurse.com Continuing Education series. Retrieved from http://ce.nurse.com/course/ce630/facebook/.
A classic “Far Side” cartoon shows a man talking forcefully to his dog. The man says: “Okay, Ginger! I’ve had it! You stay out of the garbage!” But the dog hears only: “Blah blah Ginger blah blah blah blah blah blah blah blah Ginger …”
As a nurse, I often worry that patients’ comprehension of doctors and nurses is equally limited — except what the patient hears from us is: “Blah blah blah Heart Attack blah blah blah Cancer.”
I first witnessed one of these lost-in-translation moments as a nursing student. My patient, a single woman, a flight attendant in her early 30s, had developed chest pain and severe shortness of breath during the final leg of a flight. She thought she was having a heart attack, but it turned out to be a pulmonary embolism: a blood clot in the lungs. Treatment required several days in the hospital. Already far from home and alone, she was very worried that a clotting problem would mean she could no longer fly.
When the medical team came to her room, they discussed her situation in detail: the problem itself, the necessary course of anti-coagulation treatment and the required blood tests that went with it. To me, just at the start of my nursing education, the explanations were clear and easy to follow, and I felt hopeful they would give my patient some comfort.
After the rounding team left, though, she turned a stricken face to me and deadpanned, “Well, that was clear as mud, wasn’t it?”
I sat down and clarified as best I could. But until then, I hadn’t realized what a huge comprehension gap often exists between what we in health care say to patients and what those patients actually understand.
A growing body of literature suggests that these clinical miscommunications matter, because the success of physician-patient interaction has a real effect on patients’ health.
In a 2005 article in the Journal of the American Medical Association, Eric B. Larson and Xin Yao, researchers at the University of Washington, claim that treatment outcomes are better when doctors show more empathy and take the time to make sure patients understand what’s going on.
I saw the importance of caring communication during a friend’s recent heart attack scare. He had a lingering case of bronchitis, and one morning found himself struggling for air. He had pain in his shoulders, back and neck and a feeling of increasing constriction in his chest.
Concerned, his wife took him to the emergency room, where his breathing became even more labored. In the triage area he began sweating profusely and then collapsed. A rapid response team rushed in, put him on oxygen, started an IV, got an EKG. His wife thought she was watching, helplessly, as her husband of more than 20 years died in front of her.
Minutes passed and the code team revived him, but no one told her that he’d passed out because of a protective effect of his autonomic nervous system, not because his life was threatened. No one fully explained that to him, either.
At that point his wife called me, and knowing how confusing modern health care can be, I went to the hospital to help. I caught up with them in the cardiac catheterization lab, where the miscommunications continued. The cardiac cath showed that his arteries were clear — but the diagnosis, explained in technical terms, meant nothing to his wife. It took over 12 hours to learn that his echocardiogram revealed all cardiac structures to be normal. (Also, no one told the wife that her husband would stay overnight in the I.C.U. because protocol required it, not because he actually needed intensive care.)
Although my friend received exemplary care, neither he nor his wife felt that they had. Instead, similar to my patient in nursing school, they felt they had been hijacked to a foreign land. The hospital staff members were obviously dedicated to restoring patients’ health, but they and the work itself came across as alien, obtrusive and impossible to understand. Also, my friend’s problem was correctly diagnosed days later when he went to his primary care physician. Acid reflux was causing his pain; the cure was a prescription for Prilosec.
Interestingly, patients in hospitals report more satisfying interactions with physicians when doctors sit down during rounds instead of standing, according to a 2012 article co-written by the researcher Kelli J. Swayden, a nurse practitioner, in the journal Patient Education and Counseling. Sitting gives the message “I have time,” whereas doctors who stand communicate urgency and impatience.
I don’t mean to blame doctors and nurses; it can be very hard to force yourself to slow down and tune in to a patient’s wavelength when you have other patients and countless pressing tasks to get to.
And that’s especially true today, when hospitals are focused, machinelike, on volume and flow. Bedside manner does not increase efficiency, and it certainly can’t be charged for. Still: My friends had gone from blueberry pancakes at breakfast to worrying that the husband might die, and the closest anyone got to assuaging that fear was the doctor who said, “Well, we’ve ruled out everything that will kill you right away.”
And that’s not good enough, because going to the hospital is an exercise in trust. Ill health is frightening, the treatments we offer can be scary, and stress and anxiety make people poor listeners. Our high-tech scans and fast-paced care save lives, but we need to make time for the human issues that pull at every patient’s heart.
Theresa Brown is an oncology nurse and the author of “Critical Care: A New Nurse Faces Death, Life, and Everything in Between.”
Researchers will enroll around 500 African-American children and adults who have asthma in a multi-center clinical trial to assess how they react to therapies and to explore the role of genetics in determining the response to asthma treatment. This new clinical study, which will take place at 30 sites in 14 states, is aimed at understanding the best approach to asthma management in African-Americans, who suffer much higher rates of serious asthma attacks, hospitalizations, and asthma-related deaths than whites.
The Best African American Response to Asthma Drugs (BARD) study is under the auspices of the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health.
“This large-scale clinical effort is expected to provide new insights into how health care professionals can better manage asthma in African-Americans to improve outcomes,” said Gary H. Gibbons, M.D., director of the NHLBI.
“BARD reinforces the institute’s commitment to understand, reduce, and ultimately even eliminate the disparities in asthma outcomes observed in the African-American population compared to other Americans with asthma,” added James Kiley, M.D., director of the NHLBI Division of Lung Diseases.
BARD will examine the effectiveness of different doses of inhaled corticosteroids (ICS) used with or without the addition of a long-acting beta agonist (LABA). ICS reduce inflammation and help control asthma in the long term. LABAs relax tight airway muscles. This study will compare multiple combinations of medications and dosing regimens to assess the response to therapy. BARD will track whether children and adults respond similarly to the same treatment, and evaluate how genes may affect treatment response.
“While national asthma guidelines provide recommendations for all patients with asthma, it is possible that, compared with other groups, African-Americans respond differently to asthma medications,” said Michael Wechsler, M.D., principal investigator for the BARD study and professor of medicine at National Jewish Health in Denver. “Our study is designed to specifically address how asthma should be managed in African-American asthma patients, both adults and children.”
The BARD study is supported by NHLBI’s AsthmaNet clinical trials network. BARD began enrolling patients on Feb. 10.
To schedule an interview with an NHLBI spokesperson, please contact the NHLBI Office of Communications at 301-496-4236 or nhlbi_news@nhlbi.nih.gov.
About the National Institutes of Health (NIH): NIH, the nation's medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
Written by Elizabeth Swaringen for UNC Health Care
As a nurse at UNC Hospitals, Paula Brown, RN, knows firsthand the difference family presence makes in a patient’s healing. She also knows the importance of the care and feeding of family members — especially when home is two or three hours away.
So volunteering to cook dinner for guests at SECU Family House was a no-brainer for Paula and her 16-year-old son, TJ, a sophomore at Carrboro High School. It just took the inspiration of a like-minded 10-year-old boy to make it a priority in 2014.
“I’ve known about Family House since it was a dream, before the construction even began,” said Paula, recalling a massive yard sale to raise money for the 40-bedroom hospital hospitality house that offers safe and affordable accommodations to seriously ill patients and their families who come to UNC Hospitals for care.
And once Family House opened in March 2008 minutes from UNC Hospitals, Paula had always planned to volunteer, “but sometimes life gets in the way,” she said.
“Then I learned more about the House and the good that happens there from Family House Diaries, the stories that are included in news for employees,” said Paula, who is in her 20th year as a nurse in the post-surgery acute care unit at UNC Hospitals. “It was the awe-inspiring story in October of a 10-year-old boy who cooks and serves that told us the time is now.”
Paula wasted no time getting on the dinner schedule. She called Allison Worthy, who coordinates volunteers at Family House, and nailed down Sunday, Jan. 19. Allison put Paula in touch with volunteers Charles and Patsy Harrison who lead a team that cooks dinner for guests twice a month.
She observed Team Harrison, asked questions and checked out the availability of crock pots and utensils in the community kitchen for the chili and cornbread that she and TJ had already decided would be their debut meal.
“I really enjoy chili that way and wanted to give others the option,” TJ said, surmising correctly that most guests weren’t familiar with it. The Browns offered both a meat chili and a vegetarian chili, again giving guests choices to best suit their palates.
Mother and son spent the day before in prep: chopping the onions and browning the meat for the chili, chopping other vegetables for tossed salad, baking the cornbread muffins and the brownies for dessert. By noon Sunday, four crock pots were hard at work in the Family House kitchen.
“We prepared for about 50, forgetting that it was the MLK Holiday weekend and there would be a slimmer crowd as the hospital clinics were closed on Monday,” said Paula. “But it didn’t matter. Although we had fewer guests than we’d planned for, we had plenty of leftovers, and chili is always better the second day.”
Leftovers are always welcome and disappear at Family House because the illness of a loved one does not follow a mealtime schedule, said Allison, the volunteer coordinator.
“Our guests always comment with gratitude and amazement about the volunteers who prepare the home-cooked meals here and the quality of the food,” she said. “But it’s beyond nourishing their bodies; it’s about the community of support that forms around the shared meals. We’ve steadily added Sunday night meals because Sundays have become a busy check-in day for guests. Like our guests we are grateful that Paula and TJ know their way our around kitchen, especially on Sunday nights.”
Paula and TJ saw — and felt — the gratitude firsthand. A lone female guest showed her appreciation by insisting that Paula accept a cash donation that could be used for the next dinner she and TJ prepare.
“That was one of those arguments that you can’t win, so I graciously accepted her gift, assuring her it wasn’t necessary, but much appreciated,” Paula said, noting that she and TJ had already discussed “next time” even before they had served the first bowl of chili.
And neither will forget the guest who slipped back into the kitchen after dinner, slammed his palm on the countertop to get their attention and declared,
“I just want to thank you. With her treatment my wife hasn’t felt like eating in over a month, but tonight she did. We enjoyed it.”
“I thought we were just feeding people, but it was so much more than that,” said TJ, who enjoys the logistical challenges of cooking, especially for a crowd. “Family House is a haven for people. The reactions to our meal told us that. I had run by the house many times in better weather when training with my cross-country team, but I really didn’t know what goes on here. Cooking here was fun, and I look forward to coming back.”
Cooking at Family House also allows TJ to work towards earning the 25 community service hours he needs for high school graduation. But it’s not about that requirement, both TJ and Paula agreed.
“It’s the reaction we got from people,” he said. “It was emotional and genuine for us all. The fun of the cooking makes the service requirement easier.”
"It’s a win-win for all,” Paula said, beaming.
Will chili be their signature Family House meal?
“We’ll probably branch out, but we’ll keep with comfort foods,” said TJ. “You don’t want to go too exotic. You gotta eat sometime, and we need to make it easy for people to enjoy it, maybe meatloaf and my grandmother’s macaroni and cheese.”
Just as a 10-year-old boy inspired Paula and TJ to step up and cook a fellow nurse told Paula her unit is going to plan a meal at Family House.
“I just hope it’s my day off so I can participate,” she said.
It is imperative that every nurse – new and experienced – realize the healthcare landscape has completely changed. There will be plenty of opportunities for RNs and APNs who stay current with trends in education, technology, care and personal and professional development. Nurses must be willing to step outside their comfort zone and learn new ways — and places — of working and thinking about their profession. Cynthia Nowicki Hnatiuk, RN, EdD, CAE, FAAN, executive director of the American Academy of Ambulatory Care Nurses and the Academy of Medical Surgical Nurses. stresses that, to stay competitive, nurses also will have to be able to articulate the value that they bring to outcomes, beyond tasks, in any setting. So what does every nurse need to do? Here are four key areas:
1| Skill building
Clinical skills alone won’t see us through in this new paradigm. Self-marketing, computer skills, oral and written communication, conflict management, negotiation, leadership and networking skills must be learned and practiced. Hnatiuk said nurses also need to be more business savvy, with an understanding of finances, staffing, acuity and productivity.
2| Education
Higher education is no longer optional. It is a foundation for practice in any setting and fundamental to professional and personal growth and development. Hnatiuk advises that formal and continuing education, along with clinical certification, will help nurses take their practice and careers to the next level.
For those considering advanced practice, particularly becoming nurse practitioners, the NNCC’s Hansen-Turton advises: “Don’t think too long; jump in. Opportunities will be increasing for NPs over the next 5-10 years. NPs are and will continue to be a hot commodity.” Certified nurse midwives, clinical nurse specialists and certified registered nurse anesthetists also will see expanded opportunities.
3| Professional association involvement
Our professional associations are where we connect with one another, form communities, share best practices (local and national), stay current with trends and issues, and find support. Hnatiuk added that through association involvement, you learn more than you could by yourself and progressively learn leadership skills
4| Mentoring
Hnatiuk encourages nurses to take advantage of opportunities to be mentored and to mentor others. “We have so much to share. Mentoring will allow us to achieve all we’re capable of doing.”
For personalized career advice
If you have specific career-related questions, send them to Dear Donna at www.Nurse.com/AsktheExperts/DearDonna for a personalized response.
I'm a recent new graduate and I'm trying to figure out how to setup and update my resume to be more attractive to employers. Are there certain topics or headlines that should be included and what are the rules for putting my clinical experience on my resume?
Wants a More Attractive Resume
Dear Donna replies:
Dear Wants a More Attractive Resume,
Although you may hear varying opinions about whether or not your clinical rotations should be on your new nurse resume, it is a good idea for several reasons. It looks good if you're applying to one of the facilities in that healthcare system where you did some clinical time. This is especially true if you're favorably remembered by a staff member and if you did a clinical rotation at a well-known facility.
It's not necessary to give much detail about each position or to provide dates and time frames other than the year. You can mention significant experiences you had, such as working with ventilators. On the other hand, if you have prior healthcare work experience as an LPN or nurse's aide, it may not be necessary to list clinical rotations. Be sure to include any externships or special internships you did as well. Once you've had your first job as an RN, clinical rotations and externships would no longer be listed.
As far as categories, the other common ones are: work experience; education; licensure/credentials; volunteer work (if applicable); and special skills where you can list other languages you speak, special computer skills or any other noteworthy skills. You'll find very detailed information, including new nurse resume samples, in “The ULTIMATE Career Guide for Nurses” (http://ce.nurse.com/ course/7250/).
A good resume certainly is an important marketing tool but there is much more involved in launching a successful job search, especially as a new nurse. Read “New nurse, new job strategies” (www.Nurse.com/Cardillo/Strategies) to help give yourself an edge when looking for that first full-time position.
Isabel Barradas, 48, has been a doctor for 25 years. In her native Venezuela, she was an orthopedic surgeon and head of a hospital department, with expertise in physical rehabilitation. She speaks three languages and—since marrying an American and moving to South Florida more than a decade ago—is a U.S. citizen.
Barradas passed her U.S. medical licensing exams with flying colors. But she didn't get a residency position in the specialty she loves. "Orthopedic surgery? Forget it. In this country, that is so elite," Barradas says. Competition for the training positions required for medical licensure is fierce, and most go to seniors at U.S. medical schools. Barradas decided that the position she did get—internal medicine in Buffalo, N.Y.—wasn't worth leaving her family in Miami for.
Thousands of foreign-educated doctors living in the U.S. would like to practice medicine here but don't have the time, money or language skills to compete for and complete a residency. Miami's Florida International University offers other options: accelerated programs leading to a bachelor's and master's of science in nursing which train foreign-educated doctors to be nurse practitioners. FIU's programs both give internationally educated professionals an outlet for their skills and helps add much-needed diversity to the health care workforce.
The U.S. faces a dearth of 20,400 primary care physicians by 2025, according to federal statistics. The Association of American Medical Colleges projects a shortage of thousands of surgeons and other specialists too. While an aging population and health insurance expansion increase demand for health care services, medical schools and residency programs aren't producing enough doctors to meet demand.
There are thousands of foreign-educated doctors living in the U.S. who have the expertise needed to address some of this growing need. Every year for the past decade, between 5,000 and 12,000 foreign-educated physicians who have passed their licensing exams apply for a residency position. Typically, about half get one, compared with more than 90 percent of U.S. medical school seniors who apply, according to data from the National Resident Matching Program.
International medical school graduates, like minority doctors, often go on to serve medically underserved populations. Graduates of international medical schools make up a quarter of U.S. office-based physicians, and are more likely than their U.S.-educated peers to treat minority patients, foreign-born patients, patients who speak little English and patients who qualify for Medicaid, according to a 2009 study from the Centers for Disease Control and Prevention.
Demand for highly trained nurses is also growing, particularly for nurses who speak more than one language and reflect the growing diversity of the U.S. population. If highly trained professionals like nurse practitioners and physician assistants were to take on more primary care responsibilities, the shortage of primary care doctors could be cut by more than two-thirds, according to the Health Resources and Services administration.
FIU introduced its accelerated nursing degree program in 2000, in response to pressure from underemployed Cuban doctors living in the area. The FEP-BSN/MSN program began as a bachelor's degree program that prepared students to become registered nurses. In 2010, FIU added a master's degree, and graduates of the full program can now find work as nurse practitioners—an advanced role that can include prescribing medicine and diagnosing patients. In Florida, nurse practitioners earn about $86,800 per year. Barradas hopes to find work with an orthopedic surgeon.
Isabel Barradas (left) and Mariana Luque, trained and credentialed as physicians in their native Venezuela and Colombia respectively, are nursing students at Florida International University. (Sophie Quinton)The program compresses six years of education into four, mostly by moving quickly through undergraduate-level material. English language learners get help with reading and writing academic papers, and courses are scheduled in the evenings or compressed into one day a week to fit the needs of working adults. For the past few years, the graduation rate has been close to 100 percent.
Despite its South Florida roots, the program has begun to attract students from all over the U.S. "I ask them, why don't you just go to the accelerated program where you live? And it's not the same for them," says Maria Olenick, program director. "They choose to come here because they know that there are other people in the same situation."
Most of the 200 doctors enrolled in FIU's program this year are bilingual. About 39 percent are from Cuba, 28 percent are from Haiti, and 6 percent are from Colombia, with the rest hailing from Nigeria to Lithuania. Students are evenly split between men and women, and the average age is about 40. Applicants must be U.S. citizens or permanent residents.
Some doctors are initially reluctant to enter a nursing program, Olenick says, fearing loss of prestige, but usually the negative feelings don't last. "What we're hearing from them is that they're actually really, really enjoy the role of nurse practitioner in the United States, because it's more like the way they practiced in their home countries," she says. American physicians tend to spend less time with patients and more time processing paperwork than their counterparts overseas. Barradas' patients in Venezuela used to come by just to chat.
It's not always easy for graduates of the accelerated degree program to find the kind of work they want, says Carlos Arias, chief operating officer of Access Healthcare. Although they're armed with an advanced nursing degree and have medical training, graduates are often offered entry-level positions with low salaries. Arias, a Cuban-educated doctor himself, now heads a Florida independent practice association that has hired two graduates of FIU's program to date.
Not all graduates choose to enter the workforce right away. The first class of nurse practitioners graduated last summer, and of 55 graduates 12 returned to FIU to enroll in a doctoral program. "We're looking now at making the program a BSN to DNP program, because we have so many that are interested," Olenick says of the doctoral program. "The way that nursing is moving, eventually a DNP will be required to practice as a nurse practitioner."
For the foreign-educated physicians in the program, the doctorate offers another perk. As a graduate, you get to be titled Dr. again.
CORRECTION: An earlier version of this article misspelled the name of Carlos Arias. It also omitted the number of graduates who returned to FIU to enroll in a doctoral program. Twelve did.
It just occurred to me that the new health exchange insurance policies could change the nursing career marketplace and give nurses a lot of new employment options: we can play job Tetris. Why? Read on.
Before the individual policies were available, nurses without spouses or another source of health insurance were bound to full-time work with benefits unless they opted to live dangerously. Individual policies were just totally unaffordable (I used to pay about $1,000 per month for an individual policy when I was self-employed). Now they are affordable, and they are particularly so if you consider the salary differential between full-time and PRN hourly wages. It is usually significant.
This one factor allows some mix-and-match in job searches. Perhaps your dream job has a part-time position available, so you take that and pick up PRN shifts somewhere else. Perhaps you have interests in two areas, so you find PRN positions in both. Perhaps it even works out financially for you to work full-time hours as a PRN nurse where you already are, if you work at one of the hospitals where PRN nurses can always pick and choose hours (this plan will not work if PRN hours are what they were intended to be and not guaranteed).
Disclaimer: this does not include other benefits such as retirement contributions and term life insurance that are generally offered, nor does it generally offer paid time off. Speaking as someone who was self-employed for a decade, I can readily state that employer matching for retirement and paid time off are benefits worth accepting a lower hourly rate than I would get for PRN status. However, I know that for many people health insurance is the sticking point, and for those people a whole new world may have just opened up.
Of course, your mileage may vary with the exchange policies versus a group insurance policy with an employer. I have found so far that with mine, the benefits are either similar to or better than the group policy I used to have, and I even bought a lower-tier policy because I thought it would be much more temporary than it has ended up being. They really do cover preventive screens and such at 100%. They really do pay what they say they will for copays and prescriptions, and this was not the case for my group policy. There was always an exception. As I say, this is my mileage only.
Just think, though, of the possibilities. This is important given the tight job market for nurses right now. What if you were not tied to benefits? Do you have a hobby or a sideline you could monetize and be a nurse two shifts per week? Do you have a previous career you could still put to use part time and pick up shifts now and then as a nurse?
Thinking of job opportunities this way opens up a new range of options if you are willing to, I hate to say it, think outside the box. Just keep in mind the question, “What if I didn’t have to look just in the full-time section?”
The nursing profession is facing multiple challenges in the years ahead. From the Affordable Care Act and its focus on the introduction of electronic medical records, to the aging US population, many people question what healthcare will look like in the future.
What remains certain, however, is the future of nursing is bright. Nurses are a vital part of the health care system and a valuable resource for our society.
What can nurses and nursing industry expect in the years ahead?
At this point in time:
- One third of nurses are over 50 years old. - 1/3 of the current workforce will reach retirement within the next decade or so. - Nurses work more hours now than they did in 2000.
How the Health Care Reform Will Affect Nurses
Nurses will be prepared to take on more responsibility than they currently have.
This will be helpful, since:
- Within 15 years, the country will be short 150,000 doctors. - Primary Care Physicians (PCP) will be in the greatest demand, with an estimated 45,000 needed by 2020. - Millions of new patients are expected to flood the healthcare system as new insurance takes hold. - More nurses will work in rural areas where the nurse may be the only health care provider available.
Ever-Changing Technology
As we move into the future, nursing will change thanks to new technology, such as: - The Computerized Provider Order Entry (CPOE) will reduce medication errors by about 55%. - Medication will be scanned before the patient takes it, to ensure correct dosage and type. - Transcriptions can be replaced by CPOE. - Electronic medical records will link hospitals, physician’s practices and home healthcare agencies.
The nursing profession is facing multiple challenges in the years ahead. From the Affordable Care Act and its focus on the introduction of electronic medical records, to the aging US population, many people question what healthcare will look like in the future.
What remains certain, however, is the future of nursing is bright. Nurses are a vital part of the health care system and a valuable resource for our society.
What can nurses and nursing industry expect in the years ahead?
At this point in time:
- One third of nurses are over 50 years old. - 1/3 of the current workforce will reach retirement within the next decade or so. - Nurses work more hours now than they did in 2000.
How the Health Care Reform Will Affect Nurses
Nurses will be prepared to take on more responsibility than they currently have.
This will be helpful, since:
- Within 15 years, the country will be short 150,000 doctors. - Primary Care Physicians (PCP) will be in the greatest demand, with an estimated 45,000 needed by 2020. - Millions of new patients are expected to flood the healthcare system as new insurance takes hold. - More nurses will work in rural areas where the nurse may be the only health care provider available.
Ever-Changing Technology
As we move into the future, nursing will change thanks to new technology, such as: - The Computerized Provider Order Entry (CPOE) will reduce medication errors by about 55%. - Medication will be scanned before the patient takes it, to ensure correct dosage and type. - Transcriptions can be replaced by CPOE. - Electronic medical records will link hospitals, physician’s practices and home healthcare agencies.
The nursing profession is facing multiple challenges in the years ahead. From the Affordable Care Act and its focus on the introduction of electronic medical records, to the aging US population, many people question what healthcare will look like in the future.
What remains certain, however, is the future of nursing is bright. Nurses are a vital part of the health care system and a valuable resource for our society.
What can nurses and nursing industry expect in the years ahead?
At this point in time:
- One third of nurses are over 50 years old. - 1/3 of the current workforce will reach retirement within the next decade or so. - Nurses work more hours now than they did in 2000.
How the Health Care Reform Will Affect Nurses
Nurses will be prepared to take on more responsibility than they currently have.
This will be helpful, since:
- Within 15 years, the country will be short 150,000 doctors. - Primary Care Physicians (PCP) will be in the greatest demand, with an estimated 45,000 needed by 2020. - Millions of new patients are expected to flood the healthcare system as new insurance takes hold. - More nurses will work in rural areas where the nurse may be the only health care provider available.
Ever-Changing Technology
As we move into the future, nursing will change thanks to new technology, such as: - The Computerized Provider Order Entry (CPOE) will reduce medication errors by about 55%. - Medication will be scanned before the patient takes it, to ensure correct dosage and type. - Transcriptions can be replaced by CPOE. - Electronic medical records will link hospitals, physician’s practices and home healthcare agencies.
For Sharon Hart, the third day after her chemotherapy treatment for acute myeloid leukemia is always the hardest. That’s when she feels weak and sometimes discouraged.
“The blood levels are depleted and I get tired and sick to my stomach,” said Hart, of Bolingbrook.
She was feeling that way Saturday afternoon at Chicago’s Rush University Medical Center when she looked out the window and found reason to smile.
On top of the hospital parking lot, her 14-year-old son William had stomped out a message in newly fallen snow, in letters the length of two cars: HI MOM. The ‘o’ was made into a smiley face.
When he left the hospital hours later, William and his father and uncle added: GOD BLESS U! The gesture not only lifted Hart’s mood, but warmed the spirits of other patients, families, nurses and doctors as news of the message quickly spread. People posted pictures on Twitter, Instagram and Facebook, drawing national attention.
“My son has never done anything like this before,” said Hart, 48. “He is a very caring child and very loving. ... He acted on instinct and from what was in his heart. I’m glad so many people got to see the message and that it touched so many. It shows how big God is.”
Hart was admitted to Rush after she was diagnosed with leukemia on Feb. 3. William arrived at the hospital to visit her and noticed the expanse of fresh snow on the garage. He stomped out the message, then called his mother and told her to look out the window.
“I wanted to send her the message because I thought it would brighten her spirits and help her get through this,” said William, a freshman at Bolingbrook High School. “I would love for her to be happy.
“This has been rough. I’ve been praying a lot and trying to not think about what’s going on so I can do good in school. I keep my hopes up and pray every night that my mommy gets well.”
With the help of a nurse, Sharon Hart climbed out of bed and opened the blinds. That’s when she saw that he had written, ‘HI MOM.’
When William left the hospital hours later with his dad and uncle, the three decided they would extend the message to all the patients. It was viewable from the east side of the hospital from the 9th floor to the top of the building.
“They wanted to write ‘God Bless U All,’ but they ran out of room,” said Deb Song, a spokeswoman for the hospital. So they wrote ‘GOD BLESS U,’ instead.
William said his first message was specifically for his mother. But after the visit, he thought about all the other families. As he and his father and uncle pushed around the snow with their feet, they noticed people gathering at the windows, waving, jumping and taking photos.
“It was very cold out there, but I didn’t care,” he said. “I wanted to get it done and let people see it. It’s amazing because just to see people feel happy feels good.”
A nurse who works the third shift noticed the message because a patient’s daughter was watching the men stomp it in the snow and became emotional. When Angela Washek, 26, a registered nurse in the surgical intensive care unit, looked outside, she thought the men were just playing in the snow, she told the hospital staff. Then she realized that they were shaping letters.
Song said Washek emailed pictures to the medical staff.
“We don’t always get to see the good side of things in ICU,” Washek said. “People come out of surgery and they are in pain and feeling bad. When they feel better they go to another floor. This gave us a glimpse of people at their best. It boosted our morale, that’s for sure.”
Within an hour, staff from other parts of the building were coming over to get a peek at the message, Washek said. Then the story went viral.
“I still can’t believe this,” she said. “People have called from Pittsburgh and Cleveland and said they saw it. People want to care about the good side. A story, even a small one, makes people feel good. We all want to feel good at the end of the day.”
“We got such an overwhelming response from our doctors, nurses and staff who saw it and thought it was wonderful. The gesture was so simple, but so creative and nice,” Song said.
By Monday morning, the snow -- and the message --- had been cleared from the parking, Song said.
But through photos and stories, the power of the gesture has endured.
“She said it was really heartwarming, especially since she works with acutely sick patients, which can be tough,” Song said. “The gesture was so simple, but so creative and nice.”
A qualitative study on assaults on emergency nurses, sponsored by the Emergency Nurses Association, found a need to change the culture of acceptance that is prevalent among hospital administrators and law enforcement.
Better training to help nurses recognize signs of potential trouble also is key, according to researchers, whose study was published Jan. 17 on the website of the Journal of Emergency Nursing.
“Assaults on emergency nurses have lasting impacts on the nurses and the ability of emergency care facilities to provide quality care,” 2014 ENA President Deena Brecher, RN, MSN, APN, ACNS-BC, CEN, CPEN, said in a news release.
“More than 70% of emergency nurses reported physical or verbal assaults by patients or visitors while they were providing care. As a result, we lose experienced and dedicated nurses to physical or psychological trauma for days or sometimes permanently. Healthcare organizations have a responsibility to nurses and the public to provide a safe and secure environment.”
According to Bureau of Labor statistics, an assault on a healthcare worker is the most common source of nonfatal injury or illness requiring days off from work in the healthcare and social assistance industry.
Despite that statistic, the qualitative research study discovered a culture of acceptance among hospital administrators, prosecutors and judges. One emergency nurse assault victim told the researchers the “administration will only take action when some lethal event happens.”
Perhaps in correlation with the culture of acceptance, the study also concluded that emergency nurses and hospital personnel in general are not trained to recognize cues for violent behavior.
“It is imperative that hospitals and emergency care workers address the issue preemptively through adoption of violence prevention education, zero-tolerance policies, safety measures and procedures for reporting and responding to incidents of workplace violence when they do occur,” the researchers noted. “Such actions are necessary to help nurses recognize incipient violence.”
The ENA long has taken the position that healthcare organizations must take preventive measures to circumvent workplace violence and ensure the safety of all healthcare workers, their patients and visitors.
“There will always be the potential for violence against emergency nurses,” Brecher said. “But we must not accept it as the price of helping the sick and injured. With training and a change of culture, we can significantly decrease the occurrence of assaults against emergency nurses.”
The study was conducted using a qualitative descriptive exploratory design. In the fall of 2012, a sample of ED nurses was recruited by email from the roster of ENA nurses and through an announcement on the ENA website. Eight men, 37 women and one person of unknown gender responded to the question, “Tell me about your experience of violence in the emergency setting.” Answers were emailed to and analyzed by the Institute for Emergency Nursing Research.
Only one other previous qualitative study is known to have been conducted to address workplace violence against emergency nurses in the United States since at least 2004, according to the news release.
Last June, the month he turned 90, Dr. Arnold S. Relman, the eminent former medical educator and editor, fell down a flight of stairs at his home in Cambridge, Mass. He cracked his skull and broke three vertebrae in his neck and more bones in his face.
By the time he arrived at the emergency room, blood was flowing into his brain and impinging on his windpipe, leading to severe choking and dangerously low oxygen levels. Surgeons cut into his neck to connect a breathing tube from his trachea to a mechanical respirator.
Amid the disciplined medical havoc, his heart stopped three times. Resuscitation efforts saved his life, but at the cost of several broken ribs. His condition remained precarious as he developed complications and endured still more medical procedures.
Astonishingly, he lived to write about all this. After a painful 10-week hospital stay and months of rehabilitation, he can walk — gingerly, with a cane — and is largely recovered, with his mental faculties intact.
His riveting account of the medical adventure, in the Feb. 6 issue of The New York Review of Books, is a testimonial to the best emergency medical care and a tremendous will to live. At the same time, however, it betrays a surprising lack of awareness of some critical aspects of the medical profession and the nation’s fragmented health care system.
Despite decades as a medical educator, researcher, author and editor of The New England Journal of Medicine, Dr. Relman confesses that he “had never before understood how much good nursing care contributes to patients’ safety and comfort, especially when they are very sick or disabled.” Nor did he appreciate the hypnotizing effects of technology, which robs patients of the physician’s bedside manner and affects the training of younger doctors.
How is it that a leading medical professor like Dr. Relman — who has taught hundreds of young doctors at Boston University, the University of Pennsylvania (where he was chairman of the department of medicine) and Harvard — might not have known about the value of modern-day Florence Nightingales?
A number of doctors who have talked to me about Dr. Relman’s article suggest that the culture of medical education may be largely to blame. For example, younger doctors in hospitals spend part of the day on rounds, following professors in their long white coats. Many of these august figures are supremely confident in their observations and opinions; others are more compassionate.
What professors impart on those rounds can have a major effect on the behavior of younger doctors when they go into practice and teach succeeding generations.
Dr. Relman’s initial care was in a major teaching hospital, Massachusetts General in Boston, where the kind of doctors he taught — students, interns and residents — provided the round-the-clock attention that kept him alive. Yet he did not write directly about their role, referring to them only as “a team.”
On their rounds, some medical professors prefer to talk in a hallway just outside the patient’s room as they discuss test results that are crucial in planning further care. Such behavior appears impersonal, perceived perhaps as a way of shielding bad information.
But many doctors see it as efficient, because they can note the information they deem most important — like heart rate, blood pressure and rate of intravenous drip — by standing at a patient’s door and looking in at the monitors. Feeling no need to go to the bedside, they do not. Instead they rely on nurses, failing to recognize that such behavior omits crucial elements in patient care — the physical touch and the personal touch.
Dr. Relman owes the extension of his life to drugs and devices that did not exist in their present form, if at all, when he was younger. Over the years, the surge in the number of such advances, and most importantly in their hazards, has made work vastly more complicated for doctors, nurses and other health workers. Despite the advantages of technology, tender, loving care from family and nurses is priceless, as is the bedside manner of a sympathetic doctor.
But technology’s monitors, images and devices can deflect that doctor’s attention, as Dr. Relman learned when he reviewed his hospital records and the notes he wrote to nurses and his wife, Dr. Marcia Angell (particularly while he was unable to speak because of the breathing tube).
Instead of descriptions of his appearance and feelings, the doctors’ progress notes in his electronic medical records were filled with technical data. “Conversations with my physicians were infrequent, brief and hardly ever reported,” he wrote, adding:
“What personal care hospitalized patients now get is mostly from nurses. When nursing is not optimal, patient care is never good.”
Many hospital administrators have cut nursing staffs. They say it is to make ends meet; many doctors say it is usually to increase the bottom line.
Nurses’ observations and suggestions have saved many doctors from making fatal mistakes in caring for patients. Though most physicians are grateful for such aid, a few dismiss it — out of arrogance and a mistaken belief that a nurse cannot know more than a doctor.
In many ways, Dr. Relman’s insights reflect changes and generational gaps in training doctors, nurses and other health professionals. Because these disciplines have traditionally been taught in separate silos, they often do not work as tightly as they should.
Now, as health care financing changes and doctors spend more time training in outpatient settings, a growing movement demands coordinating the education of health professionals to prepare them to work more smoothly in teams. If these efforts succeed, perhaps the next generation of doctors will no longer be surprised at the importance of nurses and other allied professionals.
Nurse scheduling platform OnShift raised $7 million in a round led by HLM Venture Partners with additional funding from Draper Triangle Ventures of Pittsburgh, Early Stage Partners of Cleveland, Fifth Third Capital, Glengary LLC of Beachwood, and West Capital Advisors of Cincinnati. This brings OnShift’s total funding to $15 million.
OnShift will use the funds to add between 20 and 25 employees to its 60-person staff, including new engineering and marketing employees.
OnShift is a nurse scheduling and shift management system for long term and senior living care. The cloud-based program can be accessed via web or an app and offers automated scheduling, overtime prevention, and open shift management. The company aims to expand within the assisted living market for now.
“We’re solely focused in that market,” VP of Finance Mike Rich told MobiHealthNews. “There are very specific regulatory needs they have in terms of scheduling that we are able to cater to within our software and within our app.”
Rich explained the technology helps this specific sector of the healthcare market because they have an “extremely thin margin for business” so overstaffing is a big problem for them.
“First and foremost what people talk about is our ability to mitigate overtime, so when a nurse calls out sick, the easiest thing to do is ask a nurse to do a double shift and that instantly puts [him or her] in an overtime position,” Rich said. “What our software does is it lets schedulers see who is able and eligible to take a shift that will not put them in overtime now or in the current day period, and then we can blast a message either through an email or text message to say there’s a position open. Then people get that message and they can instantly say ‘I want that position’. [The message] comes back to the scheduler and literally within 10 minutes they have that schedule filled with a non overtime position.”
According to Rich, 85 percent of staffing in these types of care facilities is done on paper and Excel so if the facility is staffed with 25 people one week, it will most likely be staffed the same even if three patients were discharged. OnShift also takes that into account when staffing assisted living centers.
So far, OnShift is in 1,100 different longterm care facilities and in every US state. The company also doubled in size over the last year.
“Nurses serve in a variety of professional leadership positions, from administrators and unit managers to chief nursing officers and hospital board members. Today, the challenges of leading in an increasingly complex health care environment are great; therefore, nurses need to take every opportunity to develop and hone their leadership qualities and skills. The question for every nurse—no matter the stage of her or his education or career—is: Are you the best leader you can be?” writes Sue Hassmiller, senior adviser for nursing at the Robert Wood Johnson Foundation and director of the Future of Nursing: Campaign for Action, and Julie Truelove, student at the University of Virginia School of Nursing, in an article in the January 2014 issue of the American Journal of Nursing.
The article, “Are You the Best Leader You Can Be?,” discusses the Institute of Medicine’s recommendations on nursing leadership in the 2010 report, The Future of Nursing: Leading Change, Advancing Health. The recommendations call on the health care system to “prepare and enable nurses to lead change to advance health,” by developing leadership programs and providing increased opportunities to lead. The article features a table of nurse leadership programs for nursing students and professional nurses as well as a nursing leadership resource list.
“Nurses with strong leadership and management skills are better prepared to serve individuals and their families and the community, and to collaborate with colleagues,” the authors write. Regardless of where you are in your career, “a leadership program is a step toward becoming the best leader you can be.” Read the full article here.
The American Association of Colleges of Nursing released preliminary survey data showing that enrollment in entry-level baccalaureate nursing programs increased by 2.6% from 2012 to 2013, which marks the lowest enrollment increase in professional RN programs over the past five years.
Findings are based on data reported from 720 of the 858 schools of nursing in the U.S. with baccalaureate or graduate programs. Although RN enrollment increased for the 13th consecutive year, nursing schools have identified a shortage of faculty and clinical education sites as potential barriers to realizing future growth and meeting the nation’s need for healthcare providers.
“Given the calls for a more highly educated nursing workforce from the Institute of Medicine, the Tri-Council for Nursing, nurse employers and other stakeholders, we are pleased to see at least modest growth in the pipeline of new baccalaureate-prepared nurses,” AACN President Jane Kirschling, RN, PhD, FAAN, said in a news release.
Preliminary AACN data also show a strong enrollment surge in baccalaureate nursing programs designed for practicing nurses looking to expand their education in response to employer demands and patient expectations.
The number of students enrolled in baccalaureate degree completion programs, also known as RN-to-BSN programs, increased by 12.4% last year (among 512 schools reporting). This year marks the 11th year of enrollment increases in these programs and offers further validation of the desire among nurses to advance their education to remain competitive in today’s workforce, according to the AACN.
Looking ahead, AACN plans to work collaboratively with stakeholders to ensure that enrollment in both baccalaureate and master’s level degree completion programs for RNs expands even further to meet the recommendations outlined in the 2010 “Future of Nursing” report prepared by the Institute of Medicine, including a goal of 80% of nurses having BSNs by 2020.
Acing an interview: It’s all about how you respond to questions
A strong resume, sent to the right hospitals, practices, or clinics–healthcare employers that you’ve researched online and scored tips from other nurses who work or have worked there–is step one in getting the job you want.
Nurse recruiters, hiring managers, and HR staff, who review your resume, are looking for far more than just making a skill set match. Step two is convincing them that you aren’t just qualified for the position you’ve applied for–you are the position’s best candidate! And, while your resume gets you the face-to-face job interview, it’s the rapport you establish the moment you sit down in front of the interviewer that will land you that job offer. They want to know:
How you communicate your capabilities, experience, achievements, and skills and your expectations about the position for which you are interviewing; and
How you respond (and react) to the questions and situations pitched at you during the interview.
Employers are concerned with three basic questions
Knowing how to respond to the questions you’ll be fielding during an interview–some predictable, some challenging, and some with no “right” answer–doesn’t just position you as a confident and prepared interviewee, it puts you ahead of the competition, too.
Practice answering job interview questions
Ask friends and colleagues about their job interview experiences to get an idea of what questions to expect. Practice answering the questions by consciously thinking about how you will answer them and about personal situations and experiences that will enhance your responses. Below is a list of other useful job interview sources for nurses.
According to career expert Somers, exhibitingthe following traits, characteristics, and actions during an interview will decrease your chances of getting a job offer.
Joe Long first thought of becoming a nurse when his wife was hospitalized for a week during her pregnancy with their second child. He now works at Mercy Hospital Springfield, taking care of patients in the intensive care unit.
“Nursing is manly,” Long said. “It’s not just for women.”
About 6.6 percent of nurses nationwide are male, according to the American Association of Colleges of Nursing. In Springfield, about 7.3 percent of nurses at CoxHealth are male. At Mercy, about 11.4 percent of the nurses are male.
The American Assembly of Men in Nursing was formed in 1971 in Michigan to provide support for male nurses. An Ozarks chapter is being started. There are also chapters in St. Louis and Kansas City. The organization also is open to women.
“It’s a very female-oriented world and we’re OK with that, but men still need to socialize,” said Paul Pope, the chapter president and a nursing instructor at Southwest Baptist University.
The executive director of nursing at Mercy Hospital Springfield is a male nurse, Kurtis Abbey.
Nurses like him have faced some of the obstacles that women entering predominantly male fields have faced. There have been lawsuits and complaints about isolation.
Rick Leroux, a nursing instructor at Southwest Baptist, got into nursing with the encouragement of his aunt. He learned how to make chitchat with children and to be absolutely honest about whether a medical procedure would hurt.
He treasures moments such as an encounter with the adult daughter of a man he had cared for who had a heart attack. She hugged Leroux and thanked him.
“Those are the moments we live for,” Leroux said.
Female employees at Mercy said they appreciate male nurses when it comes to lifting patients. They also value other qualities such as help in dealing with sometimes-disruptive families.
“We have a lot of difficult patients,” said Becky Pierce, who has worked at Mercy for about 40 years. “For each difficult patient, you have family members who sometimes need the physical presence of a man.”
Dr. Tobey Cronnell said male nurses tend to be more supportive of female doctors.
“I particularly enjoy working with male nurses as a female physician,” Cronnell said.
Long recently tended to John Goar, 73, who was admitted to Mercy Hospital Springfield after having trouble breathing.
Long gave him insulin and some other medication and then told Goar that his relatives were on their way to visit.
“He’s as good as a woman,” Goar said.
Long left Goar’s room. He was about halfway through his 12-hour shift. He doesn’t miss his previous career as a loan officer for a mortgage company.
“It’s the first time I have a job where I actually look forward to going to work,” he said.
His tattoo read "White Power" in 3-inch calligraphic letters. Emblazoned across his chest for all to see, the ink wasn't something I would normally have missed during my physical exam. In this case, though, his tattoo had been hidden by a bulky neck collar and the array of lines and tubes that come with being a comatose trauma patient.
Only on my third day of being this man's physician did I find myself confronted with the aggressive declaration.
I found myself wondering whether he would want me, a black woman, to be his doctor.
There was no dissatisfaction apparent in many interactions with his family, but they were somewhat distant. Was the distance born of shock over a relative's sudden, life-threatening injury? Or of discomfort with me?
As physicians, we take note of patients' demographics in part because it helps with diagnosis: Black patient with anemia? Think sickle cell. Greek patient with anemia? Think of the blood disorder thalassemia.
The Hippocratic Oath cautions us against refusing to treat patients based on these characteristics.
Doctors aren't supposed to be racist. We tend to think of ourselves not so much as people with specific identities, but more as disembodied brains and skilled hands ready to go about the work of healing.
My patient's tattoo was an unwelcome reminder that the skin I inhabit can't be checked at the hospital door.
Race is sometimes overtly discussed in health-care encounters, but usually because a patient expresses a preference for a clinician of a particular racial or ethnic background.
It is rarer for a patient to say that he or she does not want to be cared for by certain people. A few high-profile cases in the last several years involved white patients refusing care by black nurses.
While these requests are perhaps reprehensible, more controversial was the facilities' responses - in all the cases, the patients' wishes were honored. Some of the affected nurses successfully sued their employers for accommodating the racist requests, which had essentially allowed prejudice to affect their working conditions.
How should health-care providers respond to a racist, sexist, or bigoted patient? Sachin Jain is a physician of Indian descent who wrote about his experience with a patient who yelled at him to go back to India. Jain chose to yell back, a decision he later questioned.
In the New York Times' "Well" blog, Asian physician Pauline Chen revisits the Jain story and describes her own encounter with a combative swastika-decorated patient in the emergency room. She didn't wait for the patient to express his discomfort with her - she instead chose to remove herself from his presence as soon as it was clinically appropriate.
I explored the topic of racist patients in a piece for the Journal of the American Medical Association this month. I argued that I wholeheartedly reject racism and race-based prejudice, but I also recognize that patients have the right to choose their care providers and to have some control over the conditions of their care.
The therapeutic relationship between doctors and nurses and their patients is founded on mutual trust and respect; when these are missing, communication suffers and care plans fall apart. If I care for a patient who does not want me as a doctor, I have done that patient a disservice.
The responses I received to the JAMA piece were mixed. Many people thanked me for tackling a difficult issue for minority clinicians.
A few, though, criticized me for condoning inappropriate behavior. One person suggested that the clinical encounter could become a "teachable moment" in which I could fight prejudicial tendencies.
As much as I want to stamp out racism, I continue to believe that a one-on-one clinical encounter is the wrong venue to address this issue, for at least two reasons.
First, behavior is difficult to change. If I cannot persuade a patient to stop smoking or to eat more healthily, how will I convince them to shed long-held beliefs?
Second, asking for someone's respect when they are not inclined to give it is an exercise in futility. I learned that in high school.
I do think that there is a role for hospitals and other institutions to express that racism is not tolerated in clinical encounters. Similar to the "no smoking" signs that adorn healthcare facilities, I can imagine a "no offensive language or pre-judging" sign.
Health-care providers are under no obligation to treat patients in nonemergency situations, so perhaps instead of merely changing their clinicians, we should be referring bigoted patients to facilities willing to care for them.
That wouldn't have helped my trauma patient, though. He was at the brink of death, unable to declare his preference for care providers one way or the other.
As a result, he received superior care from people that he might have deemed inferior. Maybe the fact that we saved his life will serve as the ultimate teachable moment.
A study commissioned by Herman Miller Healthcare showed that nurses walk up to four miles a day on their shift. Much of this is due to supplies not being readily available and the need for better communication, like keeping tabs patient location. Technology is beginning to make the job of the nurse easier by giving them better information, leading to less steps.
Real Time Locating Systems
Real Time Locating Systems, also known as RTLS, uses small tags attached to devices, making them easier to find. For example, a typical scenario finds the nurse walking from room to room to locate a blood pressure machine for use in their rounds. With an RTLS tag, the nurse can locate the machine on a dashboard at the nurses station. They may still have to walk to the end of the unit to retrieve the machine, but it will be a direct route.
Patient Locators
Similar to RTLS are devices that patients can wear to indicate their location, according to Villanova University. Tracking down a patient can be time consuming on a busy nursing unit. A nursing aid that has taken a patient to physical therapy and radiology calls up for the patient to come down for a test. The locator tags can prevent the hunting down of people who know where Mr. Johnson is by indicating that he is in PT.
Another use suggested for these locator tags is in monitoring patients who may wander out of their rooms and be difficult to track. Mental health units, neurology units and Alzheimer's treatment centers benefit from these devices.
Tools in Your Pocket
With smartphones and tablets, you can have a number of tools in your pocket to help you get through your day easier.
The Pocket Pharmacist is available for your iPhone, and gives you a drug reference list with interactions. Calculate by QxMD uses current clinical decision trees to determine the best course of treatment.
Other tools to help you with your nursing career include a wage calculator by Intuit to help you precisely calculate your time and paycheck amount, which is handy for those extra shifts and holiday hours you're asked to work. ShiftPlanning is a nursing shift scheduling tool that the charge nurse will find useful for tracking time and adjusting schedules.
Mobile Devices and EHR
Electronic Health Records (EHR) became mandatory as of January 1, 2014, notes USF Health. Institutions must begin making patient records available online. A study by American EHR on more than 800 health practitioners showed that 33 percent with access to EHR used a tablet to access patient information.
As tablets and mobile charts become more available on nursing units, the constant walking back and forth between patient and their information is reduced. Devices such as the iPad EHR by drChrono allow bedside status updates to be made once vitals and other observations are completed.
Patient Workflow
Nursing Critical Care highlights a software system used in a Pennsylvania hospital that helps save steps during a patient's discharge. When the patient is ready to be released, the nurse uses a workflow panel to contact the transportation department to pick up the patient. Once they have arrived and are leaving with the patient, they use the panel to contact the cleaning crew. Once the room is clean, they use the panel to contact the admitting patient, to tell them the room is ready. This keeps the nurse from walking to the room to see the status, so they can report back to admitting that the room is ready for the next patient.
Every year since 2002, nursing has ranked at the top of the list of professions deemed the most trusted in the United States, according to an annual Gallup poll. The poll began including nurses in 1999, and they have claimed the top spot every year except 2001.
“It’s wonderful that nurses remain the most trusted profession in the annual Gallup poll,” said Diana Mason, PhD, RN, president of the American Academy of Nursing (AAN).
Linda Norman, DSN, RN, dean of the Vanderbilt University School of Nursing, said that the recognition is much appreciated by the profession, too.
“I think nurses, as a whole, are very proud of the fact that they are the most trusted profession, and that’s not something they take lightly,” said Norman, who also holds the Valere Potter Menefee Professor of Nursing position at Vanderbilt.
Consistently high ratings
More than 8 out of 10, or 82 percent, of the Gallup poll survey respondents gave nurses a “very high” or “high” rating on their honesty and ethical standards; the next highest professional categories were pharmacists and grade school teachers, tied with 70 percent.
The Gallup organization noted that nurses have received ratings above 80 percent every year since 2005. The profession’s highest rating for honesty and ethical standards was 85 percent in 2012.
“It’s been a very consistent finding,” Norman said. “We are the patient advocates. We’re the ones with patients for longer periods of time than other health care providers, so we have that opportunity to establish trust with them.”
Afaf Meleis, PhD, the Margaret Bond Simon Dean of Nursing at the University of Pennsylvania School of Nursing, agreed.
“Nurses have earned their spot at the top by their stellar devotion to the patient, their mastery of evidence to deliver the best practice, but particularly because they advocate for the patient,” she said. “Patients trust nurses because they deliver the best information at the bedside in difficult times.”
Looking forward
But where do you go from the top? Achieving this distinction should not be viewed as an endpoint or just as an honor, but as a charge to maintain this high level of trust with patients and their families, said Norman.
“Once you’ve gotten there, you need to make sure that it’s important to the profession as a whole to stay there,” she said. “You really embed it into what you do, and what you teach, and how you deliver care.”
And there are still challenges ahead. For example, Meleis cited the variation in laws from state to state that affect how much autonomy and independence that advanced practice nurses have when practicing. In some states, nurse practitioners have much more autonomy than in in other states, where physician supervision is mandatory by law.
“With the Affordable Care Act putting more patients into the healthcare system, we need to develop and implement policies that allow nurses to [practice to] the maximum of their ability without undue restriction,” she said. “This will benefit populations, enhance access, and ensure best implementation of the Affordable Care Act.”
Mason would like to see an elevation in the presence of nurses and the nursing perspective in the shaping of health policy. She noted that a different Gallup poll in 2010 found that thought leaders in health care don’t always include nurses in the role of key decision makers. But nurses can bring a lot to the table when it comes to transforming health care, and they have a responsibility to do so, given the public’s trust in them.
“The American Academy of Nursing is committed to get nurses appointed to local, state and national governing boards of health care organizations and consumer advocacy groups, as well as policy-related advisory bodies,” Mason said.
Encouragement for future nurses
Many nursing leaders also hope that this poll will help convince many people who are considering a career in nursing to take the plunge.
“As this poll shows, the public counts on nurses and respects them,” said Karen Daly, PhD, RN, president of the American Nurses Association (ANA). “Clearly, there are boundless opportunities for those who wish to consider nursing as a profession.”
Norman said she believes that a poll like this one that shows the great trust that people put in nurses can definitely help with recruitment. The results show potential nurses that there is opportunity for finding great meaning in the work, and in making a difference in people’s lives.
“We’ve got to make sure that this really is something that we sell with new nurses--and nurses throughout the profession,” she said.
As the institution of healthcare continues to evolve, nurses across the country are being asked to change with it. It can be easy to lose focus on the larger picture, however, when faced with the day-to-day challenges on the job.
These five reports are an eye-opening look at the healthcare system in crisis, but most importantly, they offer the nursing profession inspiring, actionable plans for how to change it.
Each of these reports is a must-read. They’re engaging and provocative and will help you come to informed opinions about the state of healthcare and your role as a nurse. Consider choosing a report every other month to distribute to your co-workers and then hold semi-formal discussion sessions to explore the themes and how they relate to your experience as a nurse.
In this ground-breaking study, published by Vital Smarts and the American Association of Critical Care Nurses in 2005, seven areas where communication breakdown occurs in healthcare delivery were identified. They found that fewer than 10 percent of healthcare works speak up when they’ve observed medical errors, incompetency and other potential harmful behaviors. One of the more interesting findings of the study was that the few who do speak up in challenging circumstances have better patient outcomes and are more likely to stay in their jobs.
A follow-up to Silence Kills, The Silent Treatment takes a closer look at the many reasons why nurses fail to speak up during crucial moments in healthcare delivery and what identifies the characteristics shared by nurses who find the courage to say something when it counts.
Published in 2010, The Robert Johnson Wood Foundation, along with the Institute of Medicine, presented a call to action. In The Future of Nursing, the authors present data, and outline constructive ways, in which the nursing profession can become a leading voice in the revolution of the healthcare system.
The American Association of Critical Care Nurses published the AACN Standards for Establishing and Sustaining Healthy Work Environments: A Journey To Excellence in 2005. In it, they identify the factors necessary to create and sustain a work environment that empowers nurses to deliver the best care possible. As you read through it, critically think about which standards your institution or unit meet, and which might be areas for improvement.
The Insitute of Medicine recognizes the relationship between a healthy work environment for nurses and optimal patient care outcomes. In Keeping Patients Safe, the IOM provides recommendations that address adequate staffing, trust in organizations, and other “bundles of change” that will ensure an optimal environment for nurses to do the jobs required of them.
Thirty minutes into a flight from Des Moines, Iowa, to Denver on Dec. 30, an intercom announcement requested medical expertise. Linda Alweiss of Camarillo, Calif., and Amy Sorensen of Casper, Wyo., answered the call. Directed to the cockpit, Alweiss told KTLA in Los Angeles that she found the pilot slumped over and mumbling, with an irregular heartbeat.
Passengers helped the two women pull the captain into the galley, where the nurses set up a defibrillator and an IV, according to KTLA. In the meantime, the jet was rerouted to Omaha, Neb.
"This is what happens in movies," Sorensen (spelled Sorenson by some outlets) told ABC News. "This isn't what happens in real life."
A co-pilot safely landed the plane in Omaha, where medics were waiting to further treat the pilot, outlets noted. As the women retreated to their seats, passengers cheered the nurses' efforts, the Star-Tribune wrote. The pilot survived.
In a statement released to media United said: “United flight 1637, a Boeing 737 operating between Des Moines and Denver Monday evening, landed safely in Omaha after the captain became ill. United accommodated the customers overnight, and they continued to Denver the next day.”
A United spokeswoman told The Huffington Post that it was not releasing anymore information on the pilot. She added that she wanted everyone to know "the passengers weren't in any danger."
Sorensen, for one, said her actions weren't really heroic.
"I really don't see myself as a hero," she told ABC News. "I did what I know for a patient that needed it."
The day has finally come: You’ve graduated from nursing school, passed the NCLEX and finally landed your dream job. Now comes the tough/awesome/rewarding part—actually working as a nurse!
When you’re just starting out, it can be tough to know who to listen to and what advice is actually relevant to you. So we asked our Facebook fans for the number-one thing they’ve learned on the job as nurses. Check out their smart, funny and inspiring responses—then let us know what you’d add to the list.
The top 10 things you’ve learned on the job
1. Never pass up an opportunity to eat or pee. —Sylvia Moose Garza
2. You can have a nurse title if you pass state boards, but you can only be a real nurse by having empathy, compassion and treating your patients as individuals—not room numbers or bed numbers. They are humans with their own souls. —Vicky Kelly
3. If it’s open, it could squirt. —Melissa Thomas Goodson
4. Never underestimate the value of listening to a patient and their troubles for a few minutes. Sometimes your ear can make all the difference in somebody’s day, year, situation or sleepless night. —Diane Byrne
5. Nursing is 10 percent skill and 90 percent communication. —Becky Peters Lay
6. Stay calm and don’t panic—98 percent of what you do can’t kill or hurt anyone (I got this piece of advice from a 35-year vet nurse who was my proctor on my first day!). —Anne Marie Dzmura
8. A little teamwork goes a long way! —Kacy Elisha Holland
9. Always be an advocate. Never be afraid to speak up for your patients’ best interest! —Monica Springhart
10. Don’t take life for granted. Stop and smell the roses. Enjoy the simple things, like the ability to take a shower or the human touch. —Kendra Ringuette Jenkins
What’s the number-one lesson you’ve learned as a nurse?
Nurses earn a mean annual wage of $67,930, according to the Bureau of Labor Statistics, and the demand for compassionate and skillful nurses is expected to grow by 26 percent between 2010 and 2020. The journey to become a nurse requires a bachelor's degree or an associate's degree, which means two to four years in the classroom as well as clinical experience in a hospital or clinical setting.
If you are a busy mom already juggling kids and work, finding the time to complete a nursing degree may seem impossible, but the wide selection of online Nursing programs available and the recent expansions in learning technologies are making this career path more feasible.
Online Degrees
There are online programs available that allow students to study both the science and art of nursing. In addition to covering diagnoses, anatomy, drugs, and other science-based topics, aspiring nurses can also learn interpersonal skills like how to be sensitive to patients and their families. These programs appeal to busy people who don't have the time to attend classes during conventional hours, but they are often used by nurses who are ready to take their career to the next level as well.
Masters in Nursing
Nurse practitioners armed with masters degrees can diagnose, treat, and manage a number of diseases and conditions, according to the National Library of Medicine. Nurse practitioners work in cardiology, women's health, or other areas of health care, and they usually earn more and have more responsibilities than their nursing peers. Some nurses even use their master's degree as a launchpad into the administration side of healthcare.
Simulation
Thanks to simulations, many student nurses can now bypass the requirement to shadow professional nurses. This makes pursuing a nursing degree easier for students who are juggling multiple responsibilities or nurses who live in remote areas with few shadowing opportunities.
Advance Healthcare Network reports that nurses can simulate oxygen delivery, work with infusion pumps, and practice other procedures in simulation learning centers. In addition to making learning more flexible for students, simulations also give nurses the chance to think more critically in a safe environment. Students can take a few moments to be extra thoughtful about a situation, without the pressure of worrying that they may lose a real patient with the wrong decision.
Apps Lighten the Load
With your bag already packed to the brim with sippy cups, extra clothing, and other kid-related supplies, you probably don't even have the energy or the strength to haul a massive bag of nursing textbooks around with you. Luckily, there are a host of apps, designed to lighten the load for nursing students.
Apps like Nursing Central have copies of essential reference books like Davis' Drug Guide, selected MEDLINE journals, Taber's Medical Dictionary, and others on them. Essentials for busy students, these apps also prepare aspiring nurses for the use of apps professionally. Recent studies indicate that 90 percent of healthcare professionals avoid misdiagnoses and prescription mishaps when they double check things with apps, according to Medlineplus. Studies like these prove that much of the technology that can help busy people to get nursing degrees will soon be popping up in professional settings as well.
Six nurses began a journey to the Philippines earlier this month. They were strangers in a land torn by Typhoon Haiyan in November. They came out of their two-week medical mission as a team.
That’s how Duluth nurse Anna Rathbun described her time hopping from makeshift medical facilities across Panay Island, which took a direct hit from one of the fiercest and deadliest typhoons in history.
“We ended up working really well together,” Rathbun said of her tour with five other nurses — three from the East Coast, one from Arizona and one from California. She also worked with nurses from other countries.
Rathbun is a registered nurse in the intensive care unit at St. Luke’s hospital, a job that had her well prepared for whatever might come a world away.
“Nurses, especially intensive care nurses, learn to work as a team,” she said. “It’s so important to be flexible and adaptable to change.”
The team went from village to village across the island, setting up in whatever building still was standing, mainly churches and schools.
Rathbun said her only expectation was that she would be treating wounds from the typhoon. She was surprised to see so many people come in for chronic conditions like diabetes, high blood pressure and respiratory conditions.
“It was everywhere we went,” she said. “We got the biggest thanks for the smallest things, like handing out vitamins.”
She provided wound and respiratory care and helped deliver a baby.
Those coming to the islands had their own health issues to deal with, Rathbun said.
“The air quality is so poor that we all had sore throats and stuffy noses almost immediately,” Rathbun said. “I got a sinus infection and upper respiratory infection.”
Rathbun is one of 3,200 nurses from across the country who signed up for a relief effort organized by National Nurses United. It raised money to pay for expenses nurses would encounter traveling to the Philippines. Rathbun couldn’t have gone otherwise.
She had just a two-day notice that she had been chosen for a mission leaving Dec. 9. She was grateful her manager at St. Luke’s was understanding and could grant the leave from work. “I had the go-ahead from day one,” she said.
“It was a whirlwind,” she said of preparing for her journey.
“I’ve always wanted to do some disaster work,” Rathbun said. “I became a nurse to help people.”
But her mother was nervous about her going overseas, Rathbun said. Now that her daughter is home and she has seen and heard of the work she did, Mom is OK.
“She’s really proud,” Rathbun said.
Coming home last Saturday was “reverse culture shock,” Rathbun said.
“You spend two weeks with people who have absolutely nothing. They lost everything,” she said. “And here, we have everything.”
That was especially true in coming home during the last commercial rush before Christmas, a holiday that had a deeper meaning for her after Panay Island.
“I follow local stories and what’s going on (in the U.S.) and I want to say, ‘Hey, there are people on the other side of the world who need help.’”
Anyone who has thought of doing a similar mission should do so, Rathbun said without hesitation.
“If you’re thinking about doing it, take the plunge,” she said. “It will change your life.”
She didn’t want to leave Panay because there is so much medical work still to be done. She’s assuaged a bit by the knowledge that the National Nurses United effort is a long-term one.
“The goal is to continue to provide care,” Rathbun said.
Her group was the third wave to enter the typhoon area. The next group will come from California, New York and Texas. They are expected to depart in early January. Nurses from 50 states and 19 nations have volunteered to help.
“There is still so much work that needs to be done,” Rathbun said. “People can’t afford their medical care, they can’t afford their meds. A lot more has to go on.”
Apple has compiled a list of its top 11 apps available in the App Store that are designed specifically for nurses. And knowing all of the submissions and apps that run through the store every day, if Apple says these are awesome, we are apt to believe it. Or at least, to check them out!
According to Mobi Health News, “most of these nurse apps have remained on Apple’s list since it first published its iTunes section for healthcare providers.” And it makes sense that the company has worked hard to ensure there are good, popular apps available to nurses, as healthcare professionals are known to be some of the first adopters of using smartphones at and for work.
In fact, a study last year by Wolters Kluwer Health’s Lippincott Williams Wilkins (LLW) of 3,900 nurses revealed that in early 2012, 71 percent of nurses were already using smartphones professionally. They’re also being used more and more in nursing school.
“Voalte One is designed to be a unified communications solution enabling phone calls across the hospital VoIP system, text messaging via the user directory, and user-friendly alarm management.”
“Nursing Central helps nurses and students find detailed information on diseases, tests, drugs, and procedures. The moment a question arises you can consult the automatically updating database of 5,000 drugs, find a definition in the dictionary with more than 65,000 entries, interpret hundreds of laboratory and diagnostic tests, and consult the latest disease information. You can also subscribe to your favorite nursing journals and search the entire MEDLINE/PubMed database directly from your mobile device.”
“This app allows novice nurses and nursing students to access over 120 skills and procedures separated by topic areas learned through fundamental nursing courses. Once the user selects the skill, they will be presented with equipment they will need to perform the procedure and a step-by-step approach to performing the procedure safely. In addition, users will have access to basic information related to common subject matter learned in fundamentals courses to utilize in the clinical setting.”
“PatientTouch is a Mobile Care Orchestration solution that enables you to orchestrate people, processes, and data in real time. By connecting frontline clinicians to their patients, care team, and existing EHR infrastructure, PatientTouch improves safety, quality, efficiency, and nursing satisfaction, while reducing costs. Ultimately, PatientTouch allows you to spend more time on direct patient care. PatientTouch delivers Positive Patient Identification (PPID) workflows, clinically contextual communications, and configurable care interventions.”
“Stop using that pager from the ’80s! Medigram for iPhone is a secure group messaging application designed to improve communication and care coordination in the hospital environment.”
“This application allows novice nurses and nursing students to search for over 340 common diseases and disorders, separated by body system. Once the disease/disorder is selected, the user will be able to have useful information right at their fingertips, including a nursing process approach to managing client care. There are simple explanations of what each of the diseases/disorders are and common assessment findings associated with them. In addition, useful information is included that incorporates priority assessments needed for clients with the selected disease/disorder.”
“This app is perfect for both academic and clinical settings, providing clear, concise coverage of 375 of the most commonly performed laboratory tests. Organized by body system and lab panels, and presented in a consistent format with normal findings, indications, test explanation, test results and clinical significance, as well as an overview of order of draw.”
"Preparing for NCLEX? Discover a simpler way to master drug information as part of your NCLEX review. Study thousands of drugs grouped into manageable categories, all with common actions and effects. Quickly access interesting facts about medications that will stick with you as you prepare for NCLEX.”
“The Merck Manuals deliver trusted disease management information to any iOS device and the web. Choose The Merck Manual for Mobile and Web standalone app or bundle it with the Merck Manual of Patient Symptoms and Davis’s Drug Guide to create a versatile point-of-need solution.”
“SHOTS by STFM is an up-to-date digital immunization reference. Perfect for clinicians, teachers, and health care providers or for anyone who need quick answers to tough vaccination questions. SHOTS by STFM is the most comprehensive immunization app available. In addition to the complete set of CDC vaccine schedules and footnotes, it also includes graphics, images, and commentary. Important up-to-date information is available for each vaccine, including: basics, high risk indications, adverse reactions, contraindications, catch-up, administration, epidemiology, brand names, and additives.”
“Lexicomp, the most trusted and comprehensive resource for mobile drug and clinical information for pharmacists, physicians, nurses, and other healthcare professionals.”
Do you use any of these apps? Have other options nurses should be checking out? Tell us about them in the comments below!
Airplane crew members on Reddit seemed to support the idea that such a small gesture makes a big difference.
"As a former FA [flight attendant], I can confirm that it is always appreciated when passengers were nice, or acknowledged us in this way," user MonorailBlack wrote on Thursday. "Flying over the holidays isn't fun - missing Christmas with your family for more than 10 years gets really old. The little things made it more tolerable."
If you enjoy posting photos of your family on Facebook, watching videos on YouTube or pinning pictures of mouth-watering desserts or stylish outfits on Pinterest, you’re not alone. But nurses are increasingly, and more strategically, using social media for professional purposes, too.
AMN Healthcare recently released the results of its 2013 Survey of Social Media and Mobile Usage by Healthcare Professionals, which looks at job search and career trends. The survey found that registered nurses, along with other clinicians, have “dramatically” increased their use of social media for job searching since 2010.
The vast majority of nurses, 88%, report they use social media for personal and/or professional purposes, and nearly half (43%) say they use social media for job searching.
Social media researcher and nurse Pamela Ressler, RN, MS, said she expects that nurses’ use of social media for a variety of purposes will continue to increase.
“Social media in and of itself is maturing,” said Ressler, who recently authored an online curriculum titled “Social Media for Nurses” for Sigma Theta Tau International. “Health care professionals, in particular nurses, have been very slow in the adoption of social media in the way other professions have. We’re a little late to the party but we’re learning.”
“I think the expectation is that people are going to be more involved” in using social media, added Marie-Elena Barry, RN, MSN, senior policy analyst for nursing practice and policy for the American Nurses Association.
Social media for nurses augments other job resources
The AMN survey found that, generally speaking, nurses and other clinicians are using fewer resources to search for jobs, but they’re becoming more discerning in the way that they do so.
Social media is just one of the tools that they’re incorporating into their job seeking, and they tend to use it for looking at job postings, researching companies and seeing if anyone in their network could help them out.
The top RN job search resource is applying directly to a company website, and has stayed steady at 2011 levels of 72%, followed by online job boards at 55% (also remaining steady). Referrals are used by just under half (47%) of all nurses down significantly from 70% in 2011. Other significant shifts in this year’s survey include decreases in nurses’ use of search engines and recruiters.
Eventually, anyone who applies for a job is going to have a direct conversation with a recruiter or human resources member. But long before that step in the process, nurses can use social media to their advantage in gathering information, said Ralph Henderson, president of healthcare staffing at AMN Healthcare. Nurses can use their network of contacts to find out who’s hiring, who may be hiring soon, and what it’s like to work for those health care employers.
“When you do find a job that you’re interested in, use your network to find out more about that organization,” he suggested. “You can use social media to find out what the culture and work environment is like before you apply.”
LinkedIn now in top spot
Another notable finding in this year’s survey: LinkedIn has finally upstaged Facebook in popularity as the main social networking choice for career purposes among health care professionals. Among nurses, 46% ranked LinkedIn as the top general social media site for career purposes, compared to Facebook at 42%.
Given that LinkedIn was designed as a professional networking medium, it’s not too surprising that nurses are turning to it for professional reasons, said Barry.
“It’s a really good way to share your information and people can reach out. It’s a great way to network and get new ideas,” she said.
In fact, Barry noted that she has personally started using LinkedIn much more in recent months for professional purposes. The ANA recently launched a staffing group on LinkedIn, and she’s become very involved in that.
“LinkedIn has become much more robust and has a lot of similarities to the conversational tone of Facebook now, with its groups,” said Ressler. “People are using it in a different way than LinkedIn was originally being used, which was just posting your profile up there and looking for jobs. Now there’s a lot more professional discussion going on on that site.”
Barry and Ressler both suggested that nurses search for groups on LinkedIn that they might already be affiliated with--a professional association, an alumni group or a specialty organization. Then follow companies or universities or organizations of interest, and follow links to new articles and journal postings to keep current.
Even if you are not actively seeking a new job, it’s important to stay active and keep learning, they stressed. Eventually you might need to call upon your network that you’ve already built and nurtured.
When asked which health care-focused social media sites they prefer for career purposes, nurses chose NursingJobs.com as their top choice at 51%; NurseZone.com was also among the top favorites, cited by 32% of the nurses surveyed.
No risky moves
In the nursing profession, you may still hear the occasional tale of social media use gone terribly wrong: a nursing student posts a picture of a patient without the patient’s permission, or a nurse makes an offhand, cutting remark about a colleague on Facebook that comes back to haunt her.
Luckily, those mistakes appear to be fewer and farther between, as nurses have become more social media savvy. But just avoiding egregious problems doesn’t mean you’re making the most out of your social media presence. Managing your online reputation also means putting your best foot forward--at all times.
Henderson said that nurses should carefully consider images or information that they post on a social media platform. Like many, he suggests having a personal (private) presence and a separate professional presence.
On the professional side, Barry said she would encourage nurses to put together a very complete résumé and ask someone to carefully edit it before posting anywhere. Then check with references to make sure they’re on board, and put all that together on LinkedIn--or in shorter formats on other platforms.
Ressler also pointed out that it is important to regularly update your online profile--both to keep it as current as possible and to remind your network of contacts that you’re out there. More and more nurses appear to be taking this advice to heart, with 59% reporting in the AMN survey that they have recently enhanced their social profile for professional purposes.
“Even if you’re not looking for a job right now, people will think of you when something comes across their desks,” she said.
Another important reminder: just because you have privacy settings, it doesn’t mean that the information will necessarily stay private.
“I just think that people need to be cognizant of what you’re posting, any comments or any pictures, because it’s there forever,” said Barry.
Nearly 9 out of 10 (88%) of the nurses surveyed say they use social media for personal and/or professional reasons;
Among RNs who use social media for job searches, 49% use it to look for job postings, 39% to research a company, 25% to see if they know anyone who could help them in their search, 13% to reach out to a recruiter, and 6% to reach out to the HR department;
More than half of the RNs surveyed (54%) said they have looked for a job in the past two years, down from 61% just two years ago;
Most nurses are still applying directly to companies via their websites; this key job search resource remained steady at 72% in 2013;
Nurses who use social media for job searching cited NursingJobs.com as their top site of choice (51%);
Twenty percent (20%) of clinicians have chosen to receive mobile job alerts, a doubling since 2010; RNs and allied health professionals are the most likely to choose this option.






 A steady diet of fast food might hurt your child in the classroom, a new study finds.
A steady diet of fast food might hurt your child in the classroom, a new study finds.

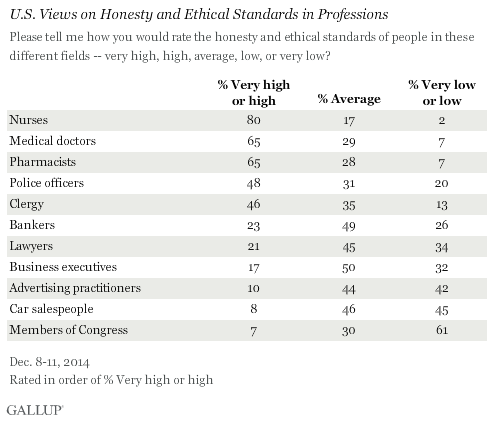





























































 Cesarean delivery was the most common inpatient surgery in the United States in 2011 and was used in nearly one-third of all deliveries, research shows.
Cesarean delivery was the most common inpatient surgery in the United States in 2011 and was used in nearly one-third of all deliveries, research shows.



















.jpg?width=595&height=6111&name=senior_foods_(2).jpg)









 Recently, Medical News Today reported on a breakthrough in xenotransplantation - the science of transplanting functional organs from one species to another. Scientists from the Cardiothoracic Surgery Research Program of the National Heart, Lung and Blood Institute (NHLBI) demonstrated success in keeping genetically engineered piglet hearts alive in the abdomens of baboons for more than a year.
Recently, Medical News Today reported on a breakthrough in xenotransplantation - the science of transplanting functional organs from one species to another. Scientists from the Cardiothoracic Surgery Research Program of the National Heart, Lung and Blood Institute (NHLBI) demonstrated success in keeping genetically engineered piglet hearts alive in the abdomens of baboons for more than a year.






























-resized-600.jpg)































































-resized-600.jpg)










.jpg)












 The single-use timer that will wholesale for about a dollar is designed to make a nurse’s life easier.
The single-use timer that will wholesale for about a dollar is designed to make a nurse’s life easier.


 and Susan Chapman (photos by Elisabeth Fall)")
 to being a nurse. Nurses must be passionate about caring for children and their families and be able to think critically and on their feet. But we also must be able to communicate effectively and efficiently with the family, patient and interdisciplinary team. We must be compassionate and able to stay calm when escalating care is needed. Although there is no one quality or characteristic that is most important for nursing, having a passion for the field, for caring for those in need, for educating others and for continuing your own education ties all the other qualities together. Nursing is not just a job or a career. Being a pediatric nurse is in many ways a calling; it is something that comes from the heart and is a lifestyle you must be passionate about.
to being a nurse. Nurses must be passionate about caring for children and their families and be able to think critically and on their feet. But we also must be able to communicate effectively and efficiently with the family, patient and interdisciplinary team. We must be compassionate and able to stay calm when escalating care is needed. Although there is no one quality or characteristic that is most important for nursing, having a passion for the field, for caring for those in need, for educating others and for continuing your own education ties all the other qualities together. Nursing is not just a job or a career. Being a pediatric nurse is in many ways a calling; it is something that comes from the heart and is a lifestyle you must be passionate about. 

 To be successful, flexibility is the single most important attribute a nurse should have. Throughout nursing school you are taught many skills to prepare you. However, there are some things that cannot be taught, yet are essential to becoming a nurse. As with most things in life, having the right balance is equally as important. Being flexible, yet having the ability to stay focused, is critical to ensure you are providing excellent care to your patients.
To be successful, flexibility is the single most important attribute a nurse should have. Throughout nursing school you are taught many skills to prepare you. However, there are some things that cannot be taught, yet are essential to becoming a nurse. As with most things in life, having the right balance is equally as important. Being flexible, yet having the ability to stay focused, is critical to ensure you are providing excellent care to your patients. 
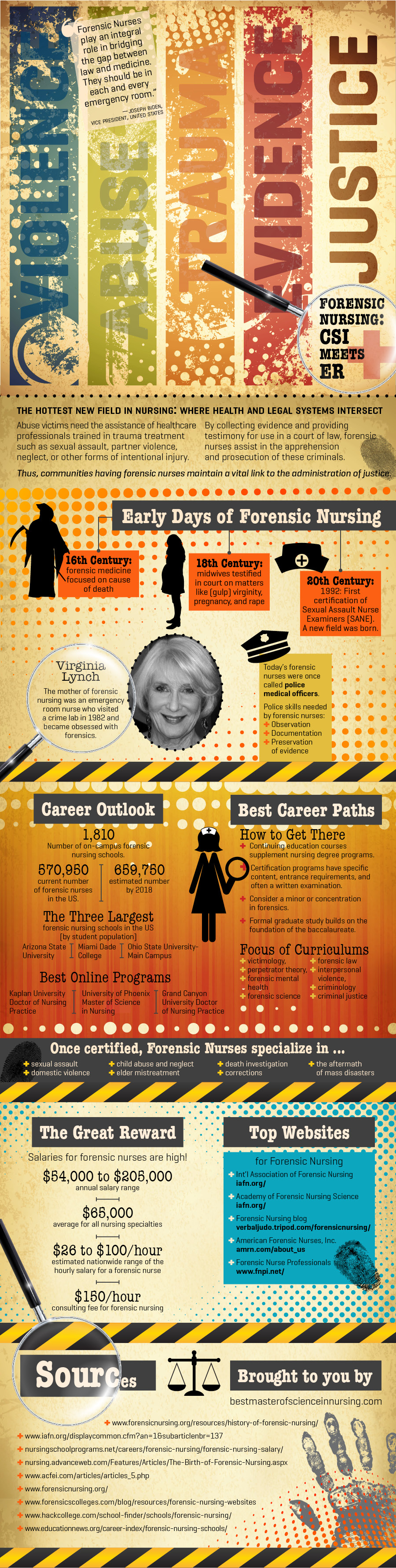

 Tuesday marks the start of National Nurses Week, an annual opportunity for communities to recognize the full range of nurses’ contributions. This year’s theme, “Nurses: Leading the Way,” recognizes nurses as leaders in the field.
Tuesday marks the start of National Nurses Week, an annual opportunity for communities to recognize the full range of nurses’ contributions. This year’s theme, “Nurses: Leading the Way,” recognizes nurses as leaders in the field.
 solution. If a life-threatening problem occurs, the nurse must take action within their scope of practice to save a patient. Nurses must have the ability to think on their feet and assure patient safety.
solution. If a life-threatening problem occurs, the nurse must take action within their scope of practice to save a patient. Nurses must have the ability to think on their feet and assure patient safety.-resized-600.jpeg)
-resized-600.jpeg) When I was a high school volunteer in the ICU of a community hospital in Brooklyn, I watched the nurses care for patients and knew I wanted to be a nurse. As a nurse for more than three decades, I continue to be inspired by nurses every day, individually and collectively.
When I was a high school volunteer in the ICU of a community hospital in Brooklyn, I watched the nurses care for patients and knew I wanted to be a nurse. As a nurse for more than three decades, I continue to be inspired by nurses every day, individually and collectively. -resized-600.jpeg)
-resized-600.jpeg)
-resized-600.jpeg) Nearly every morning for the past 10 years, I have been fortunate to have a chat with Marilyn Liota, RN, as we start our day around 7 a.m. Nearly every conversation begins with Liota saying: “Tell me what is good.” From there, we have gone off in many directions. What a way to open a conversation, and what a way to start the day.
Nearly every morning for the past 10 years, I have been fortunate to have a chat with Marilyn Liota, RN, as we start our day around 7 a.m. Nearly every conversation begins with Liota saying: “Tell me what is good.” From there, we have gone off in many directions. What a way to open a conversation, and what a way to start the day. -resized-600.jpeg)
-resized-600.jpeg) I was 21 years old when I was a new RN on a med/surg floor. On that unit there was no such thing as being alone as a nurse — we worked together as a team. It was scary, overwhelming and exciting at the same time.
I was 21 years old when I was a new RN on a med/surg floor. On that unit there was no such thing as being alone as a nurse — we worked together as a team. It was scary, overwhelming and exciting at the same time. -resized-600.jpeg) I was a new graduate nurse when I started working on the labor and delivery unit at White Plains Hospital. In nursing school, we heard that nurses eat their young, so the support, camaraderie and familylike atmosphere I felt on the unit was something I never expected.
I was a new graduate nurse when I started working on the labor and delivery unit at White Plains Hospital. In nursing school, we heard that nurses eat their young, so the support, camaraderie and familylike atmosphere I felt on the unit was something I never expected. -resized-600.jpeg)
-resized-600.jpeg)










































































































 As a registered nurse in the cardiac surgery ICU at Beth Israel Medical Center, Valley Fox, RN, BSN, MA, AP, CCRN, witnesses the spectrum of life and death.
As a registered nurse in the cardiac surgery ICU at Beth Israel Medical Center, Valley Fox, RN, BSN, MA, AP, CCRN, witnesses the spectrum of life and death. .jpeg) month-long art exhibit at New York University’s medical sciences building called “Origins of Medicine.”
month-long art exhibit at New York University’s medical sciences building called “Origins of Medicine.”.jpeg) Still, healthcare intrigued her, and the opportunity to travel, move around and practice in different places cinched her decision to become an RN. She worked in Florida, Illinois and upstate New York before settling in New York City. Nursing is a career path she has not regretted.
Still, healthcare intrigued her, and the opportunity to travel, move around and practice in different places cinched her decision to become an RN. She worked in Florida, Illinois and upstate New York before settling in New York City. Nursing is a career path she has not regretted. 

 We all have moments in which the stress of our jobs threatens to make our heads spin around 360 degrees. Moments like that are fine, but if there’s a trend toward constant head-spinning, then you, my friend, need an intervention.
We all have moments in which the stress of our jobs threatens to make our heads spin around 360 degrees. Moments like that are fine, but if there’s a trend toward constant head-spinning, then you, my friend, need an intervention. 
 it happened,” McGinn says. “I felt like other people who I worked with found ways to kind of cope with it, but I hadn’t really found that. When this came up, I thought this was a perfect way to celebrate how far the victims have come and recognize my co-workers.”
it happened,” McGinn says. “I felt like other people who I worked with found ways to kind of cope with it, but I hadn’t really found that. When this came up, I thought this was a perfect way to celebrate how far the victims have come and recognize my co-workers.” 
 young boy who needs a heart transplant.
young boy who needs a heart transplant.



 By
By  than one language and reflect the growing diversity of the U.S. population. If highly trained professionals like nurse practitioners and physician assistants were to take on more primary care responsibilities, the shortage of primary care doctors could be cut by more than two-thirds, according to the Health Resources and Services administration.
than one language and reflect the growing diversity of the U.S. population. If highly trained professionals like nurse practitioners and physician assistants were to take on more primary care responsibilities, the shortage of primary care doctors could be cut by more than two-thirds, according to the Health Resources and Services administration.
 Source:
Source:  very loving. ... He acted on instinct and from what was in his heart. I’m glad so many people got to see the message and that it touched so many. It shows how big God is.”
very loving. ... He acted on instinct and from what was in his heart. I’m glad so many people got to see the message and that it touched so many. It shows how big God is.” and editor, fell down a flight of stairs at his home in Cambridge, Mass. He cracked his skull and broke three vertebrae in his neck and more bones in his face.
and editor, fell down a flight of stairs at his home in Cambridge, Mass. He cracked his skull and broke three vertebrae in his neck and more bones in his face. additional funding from Draper Triangle Ventures of Pittsburgh, Early Stage Partners of Cleveland, Fifth Third Capital, Glengary LLC of Beachwood, and West Capital Advisors of Cincinnati. This brings OnShift’s total funding to $15 million.
additional funding from Draper Triangle Ventures of Pittsburgh, Early Stage Partners of Cleveland, Fifth Third Capital, Glengary LLC of Beachwood, and West Capital Advisors of Cincinnati. This brings OnShift’s total funding to $15 million.
 you’ve researched online and scored tips from other nurses who work or have worked there–is step one in getting the job you want.
you’ve researched online and scored tips from other nurses who work or have worked there–is step one in getting the job you want.
 to see, the ink wasn't something I would normally have missed during my physical exam. In this case, though, his tattoo had been hidden by a bulky neck collar and the array of lines and tubes that come with being a comatose trauma patient.
to see, the ink wasn't something I would normally have missed during my physical exam. In this case, though, his tattoo had been hidden by a bulky neck collar and the array of lines and tubes that come with being a comatose trauma patient.




 The day has finally come: You’ve graduated from
The day has finally come: You’ve graduated from 
 like handing out vitamins.”
like handing out vitamins.”